
Abstract
Angiofibroma is a rare, benign vascular tumor traditionally associated with the nasopharynx of adolescent males. In contrast, extranasopharyngeal angiofibromas (ENAs) exhibit a wider demographic distribution and may arise in diverse anatomical sites. We report a case involving a 45 year-old woman presenting with a 4 month history of a mass located on the lateral border of the anterior tongue. Complete excision under local anesthesia was performed. Histopathological analysis demonstrated a proliferation of irregular vascular channels lined by benign endothelial cells, set within a fibrovascular stroma, findings consistent with angiofibroma, and devoid of malignant features. Given that lingual involvement is exceptionally rare, this represents only the second documented case of tongue angiofibroma. The diagnostic challenge is compounded by its overlapping clinical and histological characteristics with other vascular lesions. Surgical removal proved curative, with no evidence of recurrence after 1 year of follow-up. This case underscores the importance of thorough clinicopathological correlation in establishing an accurate diagnosis and expands the recognized spectrum of ENA, reminding clinicians to include this entity in the differential diagnosis of oral soft tissue masses. Our findings significantly enhance clinical awareness and management.
Introduction
Angiofibromas are histologically benign yet locally aggressive vascular tumors characterized by a fibrovascular stroma and irregular blood vessels lined by endothelial cells. 1 While classically described as juvenile nasopharyngeal angiofibromas (JNAs) affecting adolescent males, extranasopharyngeal angiofibromas (ENAs) are rare entities with distinct clinical and epidemiological profiles. ENAs account for ~0.05% of head and neck tumors and exhibit a broader age distribution (8-87 years) and a more balanced sex ratio (male-to-female ratio: 2.13:1) compared to JNAs.1,2 These tumors have been reported in diverse sites, including the nasal septum,1,3 maxillary sinus, 4 ethmoid sinus, 2 larynx, 2 infratemporal fossa, 2 and oral cavity.5-7 Notably, intraoral ENAs are exceedingly rare, with isolated cases documented in the buccal mucosa, 8 mandible,6,7 and palatine tonsil. 2 Within the oral cavity, lingual involvement is exceptionally uncommon, with only 1 prior case reported in the literature. 5 This report presents the second documented case of angiofibroma arising in the tongue, underscoring the diagnostic challenges and clinical significance of this rare presentation. The rarity of lingual angiofibromas, coupled with their histopathological overlap with other vascular lesions, highlights the importance of meticulous clinicopathological correlation to ensure accurate diagnosis, and appropriate management.
Case Presentation
A 45 year-old woman presented to the Ear, Nose, and Throat clinic with a chief complaint of a mass on the tongue. The mass had been present for the past 4 months, gradually increasing in size. It was painless and not associated with any other symptoms. The patient had no significant medical or surgical history. Physical examination revealed a firm, well-defined, smooth, pinkish-white, non-tender mass measuring ~1 × 2 cm on the lateral border of the anterior third of the tongue (Figure 1). The remainder of the head and neck examination was unremarkable. An excisional biopsy of the mass was performed under local anesthesia (Figure 2). Microscopic examination of serial sections demonstrated a neoplastic proliferation composed of a mixture of vascular structures lined by benign endothelial cells, embedded within loose connective tissue, and fibrous stroma. These findings were consistent with a diagnosis of angiofibroma. There was no evidence of malignancy or atypical cellular features (Figure 3). The postoperative period was uneventful, and no tumor recurrence was observed during 1 year of follow-up.

Demonstrates the mass on the lateral border of the anterior third of the tongue.

Shows the site of the mass following excision under local anesthesia.
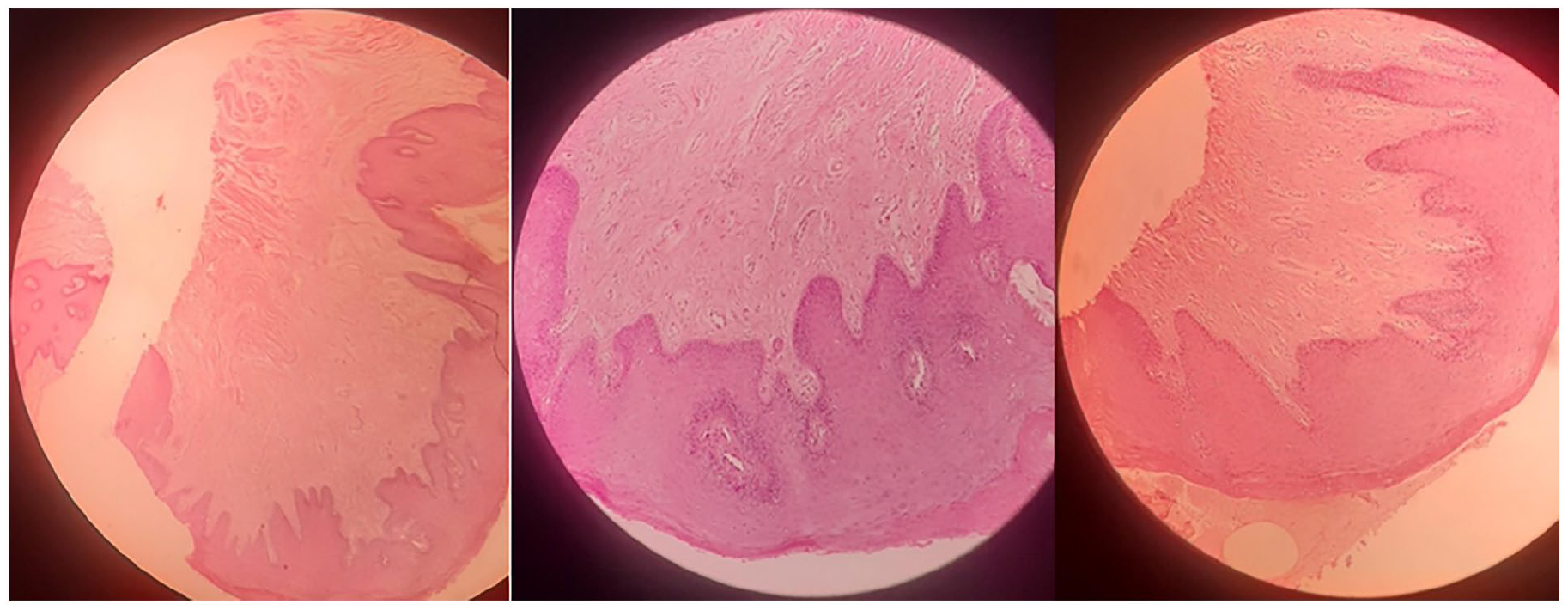
Histopathological examination, stained with hematoxylin and eosin, reveals benign vascular proliferation within a stroma composed of connective and fibrous tissue.
Discussion
The presented case of lingual angiofibroma underscores the diagnostic and clinical challenges inherent to ENAs, particularly given their rarity in the oral cavity. This report represents only the second documented instance of angiofibroma arising in the tongue, emphasizing its exceptional nature. While JNA predominantly affects adolescent males, ENAs exhibit distinct epidemiological profiles, including a broader age range (8-87 years) and a more balanced sex ratio (male-to-female: 2.13:1), as highlighted in recent literature.1,2 The current case aligns with these trends, involving a 45 year-old woman, further supporting the notion that ENAs lack the hormonal and demographic constraints characteristic of JNAs. Clinically, ENAs often present as painless, slow-growing masses, as observed here and in prior reports of nasal septal and mandibular angiofibromas.1,3,6,7 However, their nonspecific symptoms—such as nasal obstruction, epistaxis, or dysphagia—frequently overlap with other vascular or fibrous lesions, necessitating rigorous clinicopathological correlation. In this case, the absence of atypical cellular features or malignancy on histopathology, coupled with the characteristic fibrovascular stroma and irregular vascular channels, confirmed the diagnosis. Similar histological findings were noted in palatine tonsil and mandibular cases,2,6 reinforcing the importance of microscopic evaluation to differentiate ENAs from mimics such as hemangiomas, pyogenic granulomas, or solitary fibrous tumors.
Imaging plays a pivotal role in preoperative assessment. While contrast-enhanced CT and MRI are standard for evaluating tumor extent and vascularity, preoperative embolization—commonly employed for JNAs—is less frequently required for ENAs due to their comparatively lower vascularity. 2 In the current case, the lesion’s small size and superficial location permitted straightforward excision without embolization, consistent with management strategies for buccal mucosal and nasal septal ENAs.3,8 This contrasts with larger, deeply invasive tumors, such as those in the infratemporal fossa, which may necessitate multimodal approaches. 2 No recurrence cases (few in number) have been reported in ENAs, compared to JNAs, where the recurrence rate ranges from 6% to 27.5%.9,10 This favorable prognosis likely stems from their well-circumscribed nature and limited invasiveness, as evidenced by the absence of recurrence in the present case after 1 year. Similar outcomes were reported in mandibular and nasal septal ENAs, underscoring the efficacy of complete surgical excision as the cornerstone of treatment. Notably, the pathogenesis of ENAs remains debated. While hormonal influences and genetic factors (eg, chromosome 17 deletions) have been proposed for JNAs, the etiology of ENAs may involve developmental anomalies, such as ectopic remnants of fascia basalis or vascular malformations.1,3 The current case, alongside lingual and mandibular examples, supports the hypothesis that ENAs arise from pluripotent mesenchymal cells capable of divergent differentiation. 6
ENAs are significantly rarer than nasopharyngeal angiofibromas, and their clinical presentation varies widely depending on location. A review article mentions that the maxilla is the most common site, followed by the ethmoid and nasal cavity. Our case of lingual angiofibroma is exceptionally rare, making it a valuable addition to the literature. 9 A study suggests that ENAs may arise from aberrant embryological remnants of the fascia basalis or from vascular malformations. This supports the hypothesis that these tumors are not hormonally driven like JNAs but may stem from mesenchymal differentiation anomalies. 9 A review emphasizes that while preoperative embolization is standard for JNAs, it is rarely needed for ENAs due to lower vascularity. Our case exemplifies this well, as simple excision was sufficient. Discussing this point could help differentiate surgical approaches for different angiofibroma subtypes. 9
Lingual angiofibroma, though exceedingly rare, warrants inclusion in the differential diagnosis of oral vascular lesions. Meticulous histopathological examination, complemented by immunohistochemistry (eg, CD34, SMA), remains critical for accurate diagnosis. Surgical excision with clear margins ensures favorable outcomes, as demonstrated here and in analogous cases. Long-term follow-up is essential, albeit recurrence remains uncommon in ENAs. This case expands the anatomical spectrum of these tumors and reinforces the need for heightened clinical awareness to avoid diagnostic pitfalls.
Conclusion
This rare case of lingual angiofibroma—only the second reported globally—illustrates the diagnostic nuance required for ENAs. Despite their benign nature, ENAs mimic common vascular lesions clinically, demanding rigorous histopathological evaluation to confirm diagnosis. Complete surgical excision proved curative, with no recurrence at 1 year, aligning with ENAs’ generally favorable prognosis. While preoperative embolization is rarely needed due to lower vascularity compared to JNAs, individualized management based on tumor size and location remains key. Clinicians should consider ENAs in the differential diagnosis of oral soft tissue masses, even in atypical demographics. This case enriches the sparse literature on lingual ENAs, reinforcing the importance of clinicopathological correlation and surgical precision in managing rare entities. Heightened awareness of such presentations ensures timely diagnosis and optimal outcomes, underscoring that rarity should not equate to oversight.
Footnotes
Ethical Considerations
Our institution does not require ethical approval for reporting individual cases. Written informed consent was obtained from the patient for publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The data that support the findings of this study are available from the author or corresponding author upon reasonable request.