
Abstract
Objectives:
To establish a standardized method for classifying nasal septal mucoperichondrial flap (NSMF) thickness using computed tomography (CT) scans and correlate preoperative measurements with intraoperative findings to improve surgical planning and outcomes.
Design:
A retrospective cohort study.
Setting:
A private hospital.
Participants:
A total of 196 adult patients (mean age 31.99 years) who underwent septoplasty between April 2021 and February 2024.
Main Outcome Measures:
The primary outcomes included the optimal CT thickness cutoff to differentiate NSMF as “thin” or “thick” and its sensitivity and specificity. Secondary outcomes included demographic predictors of intraoperative complications.
Results:
Our study determined that a 3.65 mm cutoff in CT scans could differentiate between “thin” and “thick” NSMF with 80.9% sensitivity and 78.5% specificity. The average age of participants was 31.99 years. No gender-based differences were observed in the subjective reporting of nasal thickness during surgery. Logistic regression identified age as a significant predictor for the occurrence of tears during surgery.
Conclusions:
The research validates the use of a 3.65 mm CT scan cutoff for preoperative NSMF thickness classification, correlating with surgical findings and demonstrating high accuracy. These findings suggest the potential for CT measurements to become a routine part of preoperative nasal surgery planning, improving outcomes and reducing the risk of complications. Further investigation into direct measurement techniques for septal thickness is recommended to enhance surgical precision.
Introduction
The nasal septum is composed of cartilage anteriorly and bone posteriorly, and it is enveloped anteriorly on both sides by the nasal septal mucoperichondrial flap (NSMF). The anatomical structure and surgical manipulation of the NSMF are critical in surgeries involving the nasal septum, such as septoplasty. Variability in the thickness of the NSMF is a crucial factor that influences outcomes in these procedures. A thinner NSMF predisposes patients to mucosal tears during surgery, leading to potential complications such as septal perforations. This study aims to assess the correlation between preoperative computed tomography (CT) measurements of septum thickness and intraoperative findings, explore demographic influences on mucosal thickness, and examine how these factors correlate with surgical outcomes, particularly the incidence of mucosal tears. The insights gained will be invaluable for enhancing surgical techniques and improving patient outcomes.1,2
Despite recognizing the clinical relevance of NSMF thickness, the literature lacks a sufficient number of studies addressing this concern. This gap underscores the necessity of a reliable method to assess and classify septum thickness preoperatively. This research seeks to establish a radiological classification for septum thickness using CT scans, correlating it with surgical observations of NSMF thickness to enhance clinical applicability. Prior studies, such as a cadaveric one, have measured septal thickness but lacked practical clinical interpretation. 3
The study hypothesizes that a thinner NSMF correlates with an increased risk of intraoperative mucosal tears. By classifying the septum into “thin” and “thick” categories based on preoperative CT measurements, we aim to provide a predictive tool for surgical complications, thereby facilitating better preoperative planning and patient counseling. The classification system derived from this study could revolutionize the surgical approach to the nasal septum, improving common procedures such as septoplasty. 4
Materials and Methods
Participants
This retrospective study examined 196 adults who underwent septoplasty performed by the principal investigator (AA) at a private hospital between April 2021 and February 2024. Eligible patients were 18 years and older and had received a preoperative CT scan of the paranasal sinuses. Exclusion criteria included nasal septal perforation, active infections, nasal malignancy, or previous surgeries that could impact the thickness of the nasal septum.
Study Design
Septoplasty was performed under general anesthesia with an endoscopic approach. We administered 2 ml of 1% lidocaine with 1:100,000 epinephrine to each side of the nasal septum. A nasal pledget saturated with a 1% xylometazoline solution was placed in each nostril. The surgery commenced with an incision, utilizing the Killian technique; however, if the deviation was anterior, a hemitransfixion incision was the preferred choice. For enhanced visualization, we employed a 4 mm rigid endoscope from Karl Storz. Following the procedure, bilateral intranasal Doyle silicone splints were then inserted, they are typically removed between the fifth and seventh days. We then scheduled follow-up appointments 3 weeks after surgery, with additional visits as required if sinus surgery has been performed.
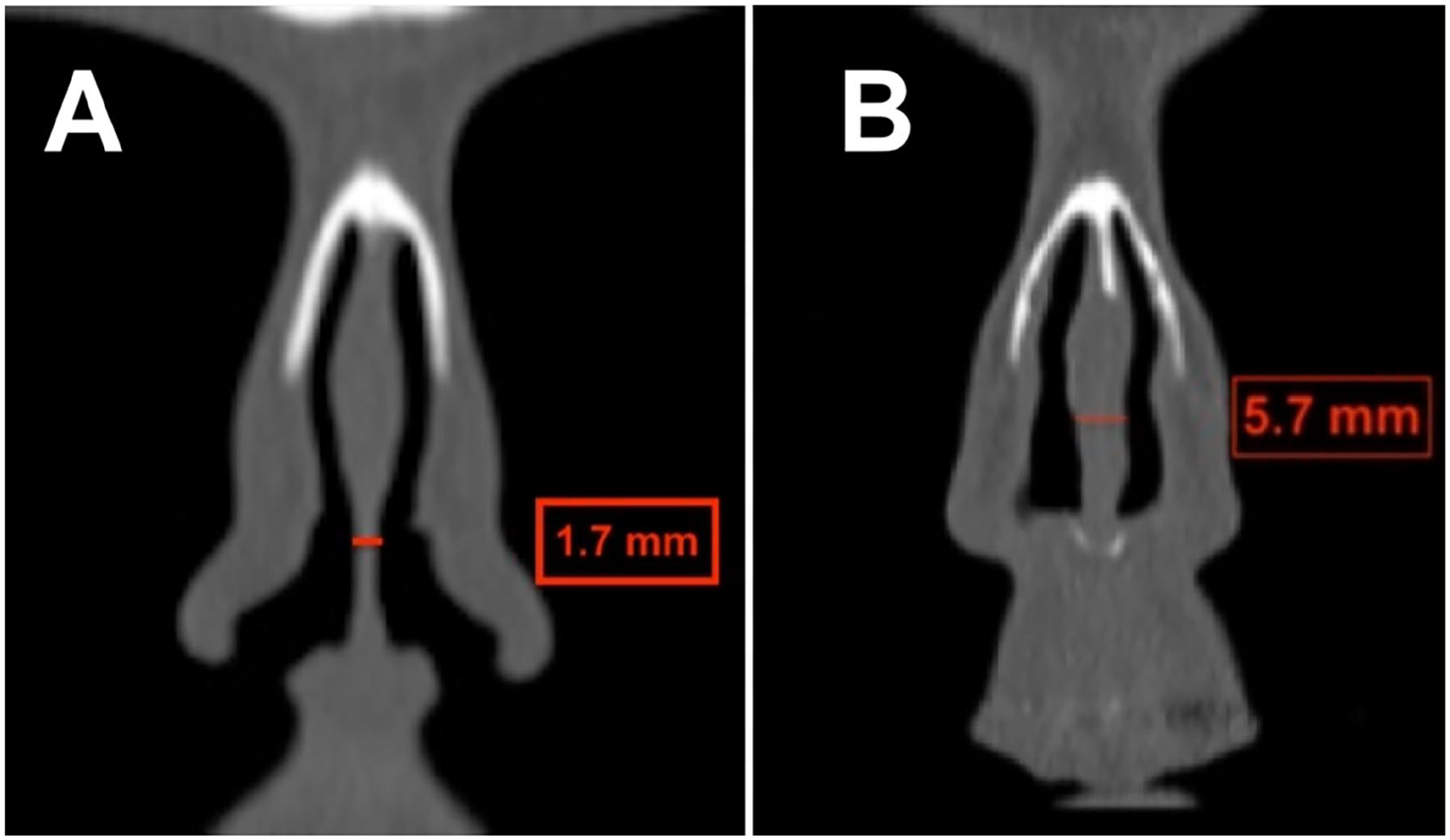
Furthermore, we used standard software to perform radiological CT scan imaging to assess the nasal septum thickness. CT scans were performed using either the GE Healthcare Revelation, capable of 256 slices with Adaptive Statistical Iterative Reconstruction (ASiR) technology for dose optimization, or the Siemens Somatom Definition AS, which offers up to 128 slices and includes Care Dose 4D technology for dynamic dose adjustment. Measurements were taken at the Kilian incision area and saved on an Excel spreadsheet. The imaging protocol included measuring septum thickness at specific anatomical landmarks. Measurements were taken on the coronal plane from the anterior tip of the nasal bone to the nasal spine (Figure 1A) and on the sagittal plane where the lower third intersects with the upper two-thirds (Figure 1B). Utilizing the “ruler” function on the coronal plane (Figure 1C), measurements were recorded in millimeters and rounded to the nearest tenth for accuracy. An independent radiologist, FMA, performed these measurements following a standardization session with surgeon AA to ensure consistency. This approach aimed to align the radiological measurements with the precise locations of incisions, thereby enhancing the relevance of the data to surgical outcomes.
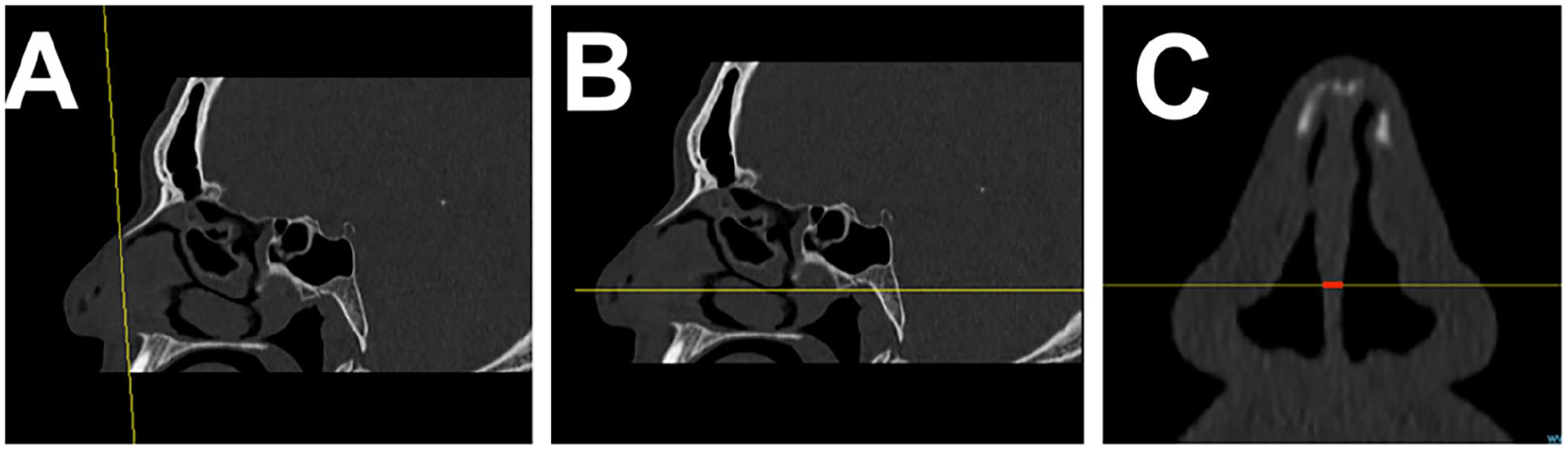
Illustration of the method for determining septal thickness in CT scans. CT measurement technique. This figure illustrates the method for determining septal thickness in CT scans, which is integral to preoperative assessment and planning. (A) The plane is anterior to the nasal bone and anterior nasal spine. (B) The juncture where the lower third intersects with the upper two-thirds on the sagittal plane. (C) Recorded measurement on the coronal plane where (A) and (B) intersect (red line).
Variables
The variables collected and included in the study are as follows:
The classification of NSMF thickness into “thin” or “thick” categories was determined based on intraoperative assessments and documented in the patients’ standard operative records. In Figure 2, an example of thin (Figure 2A) and thick (Figure 2B) as subjectively reported intraoperatively. Measurements of nasal septal thickness on CT scans were conducted blind to the intraoperative evaluations to minimize bias, ensuring that the person measuring the CT thickness was unaware of the intraoperative thickness assessments.
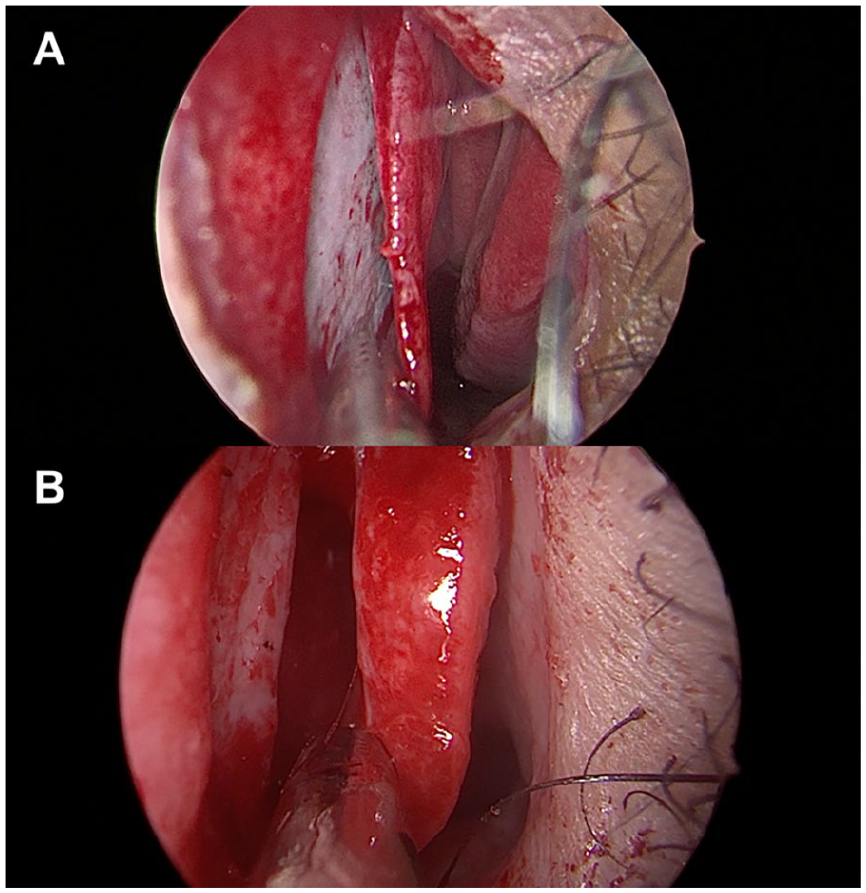
An example of an intraoperative endoscopic view subjectively described as thin (A) versus thick (B) nasal septal mucosa.
Data Analysis
Descriptive statistics, including mean, standard deviation, frequency, and percentage, provided an overview of the sample demographics and septum thickness. Inferential statistics were utilized to compare septum thickness across different groups. The Shapiro-Wilk test assessed the normality of continuous variables. We used ROC curve analysis to identify the optimal cutoff for septum thickness, assessing sensitivity, specificity, positive predictive value (PPV), negative predictive value (NPV), and accuracy. The significance level was established at P < .05, with results presented in tables, graphs, and figures.
Results
Using normality tests (Shapiro-Wilk test), we established that CT thickness and age did not follow a normal distribution (CT thickness P < .001; Age P = .006). Spearman rank correlation was used to assess the relationship between age and CT thickness. For our independent testing, we used the Mann-Whitney U test. The distribution of intraoperative thickness assessments is depicted in Figure 3.
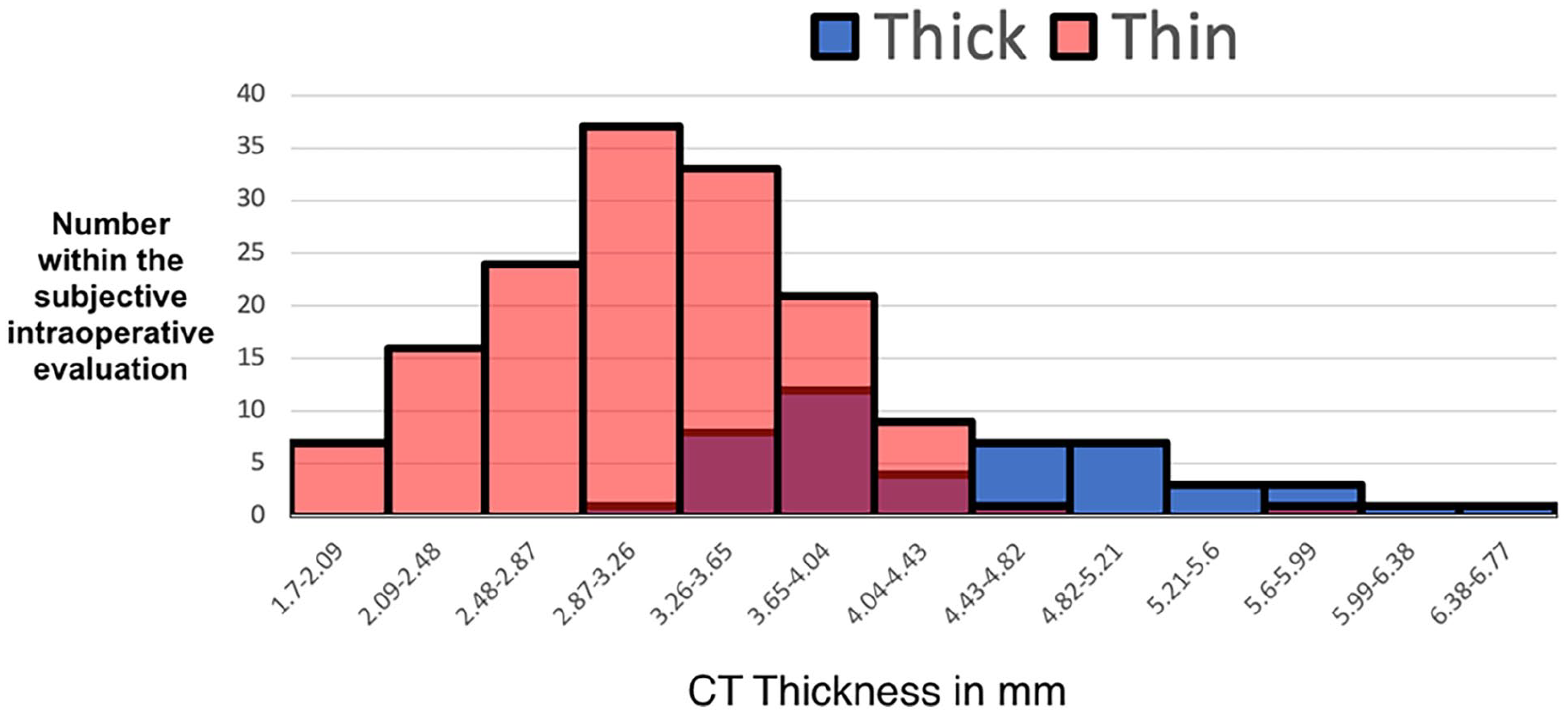
Distribution curve of measured septal thickness. The distribution curves depict the overlap of CT-measured thickness for the categorized “thin” and “thick” groups as per subjective intraoperative evaluation. CT, computed tomography.
Descriptive Statistics
In the study with participants ranging from 18 to 63.7 years, the average age was 31.99 ± 8.82 years (95% CI: 30.75–33.23).
The study’s procedural data revealed that Functional Endoscopic Sinus Surgery (FESS) was performed in 53.1% of cases. Most incisions (79.1%) were on the left side. The most common finding was small unilateral tears in the flap (less than 5 mm) at 49.5%, followed by larger unilateral tears (16.3%), no tears (30.6%), and small bilateral tears (3.6%).
Independent Samples Test
The Mann-Whitney U test indicated no significant age difference at the time of surgery between patients with “Thin” versus “Thick” NSMF (U = 2982.500, Z = −1.531, P = .126). However, there was a significant difference in septum CT thickness: the “Thin” group had a mean thickness of 3.15 mm (SD = 0.66, 95% CI: 3.04–3.26), while the “Thick” group exhibited a mean of 4.40 mm (SD = 0.85, 95% CI: 4.15–4.65). This difference was statistically significant (U = 813.000, Z = −7.936, P < 0.001), reinforcing the relationship between subjective assessments and objective CT measurements.
Gender did not have a significant effect on subjective reports of nasal thickness during surgery, with a Chi-Square value of 0.003 and an asymptotic significance of 0.957. Furthermore, the presence of tears did not demonstrate a significant correlation with assessments of nasal thickness, as reflected in a Pearson Chi-Square value of 0.049 and an asymptotic significance of 0.824. A significant gender difference in CT thickness was observed, with males (N = 137) having a mean thickness of 3.5162 ± 0.9 mm (95% CI: 3.3647–3.6674), which was thicker than that of females (N = 59), who had a mean thickness of 3.2949 ± 0.8 mm (95% CI: 3.0718–3.5181). The Mann-Whitney U test confirmed this difference as statistically significant (U = 3284, Z = −2.081, P = 0.037). In addition, the mean age at surgery was 32.42 years (95% CI: 30.90–33.95) for males and 30.98 years (95% CI: 28.80–33.16) for females.
The Mann-Whitney U test revealed no significant age difference between genders at surgery (U = 3726.5, Z = −0.865, P = .387). However, patients undergoing Functional Endoscopic Sinus Surgery (FESS) with septoplasty (mean age = 33.47 years) were significantly older than those with septoplasty alone (mean age = 30.32 years), with a U value of 3741.5, Z score of −2.631, and P = 0.009). The Mann-Whitney U test showed no significant difference in CT thickness of septum between patients with tears (mean = 3.414 mm, SD = 0.89775, 95% CI: 3.2617–3.5662) and those without (mean = 3.530 mm, SD = 0.86657, 95% CI: 3.3061–3.7539), with a U value of 3727.000, Z score of −0.965, and P-value of.334, suggesting no correlation between CT thickness and tear occurrence.
Chi-Square tests revealed a significant association between gender and CT thickness classification post-3.65 mm cutoff (Pearson Chi-Square value of 8.691, df = 1, and P = .003), with more females than males classified as “below/thin” and vice versa for “above/thick.”
ROC Curve Analysis
Figure 4 shows a highly significant area under the curve for CT thickness [AUC = 0.884, se = .025, P < .001, 95% CI (0.835, 0.933)]. This confirms that a 3.65 mm cutoff can effectively classify NSMF thickness with a sensitivity of 80.9% and specificity of 78.5%. The PPV is 54.29%, while the NPV is high at 92.86%, thus reliable detection of “thin” mucosa in surgery. Subjective assessments had an accuracy of 79.08% compared to CT scans.
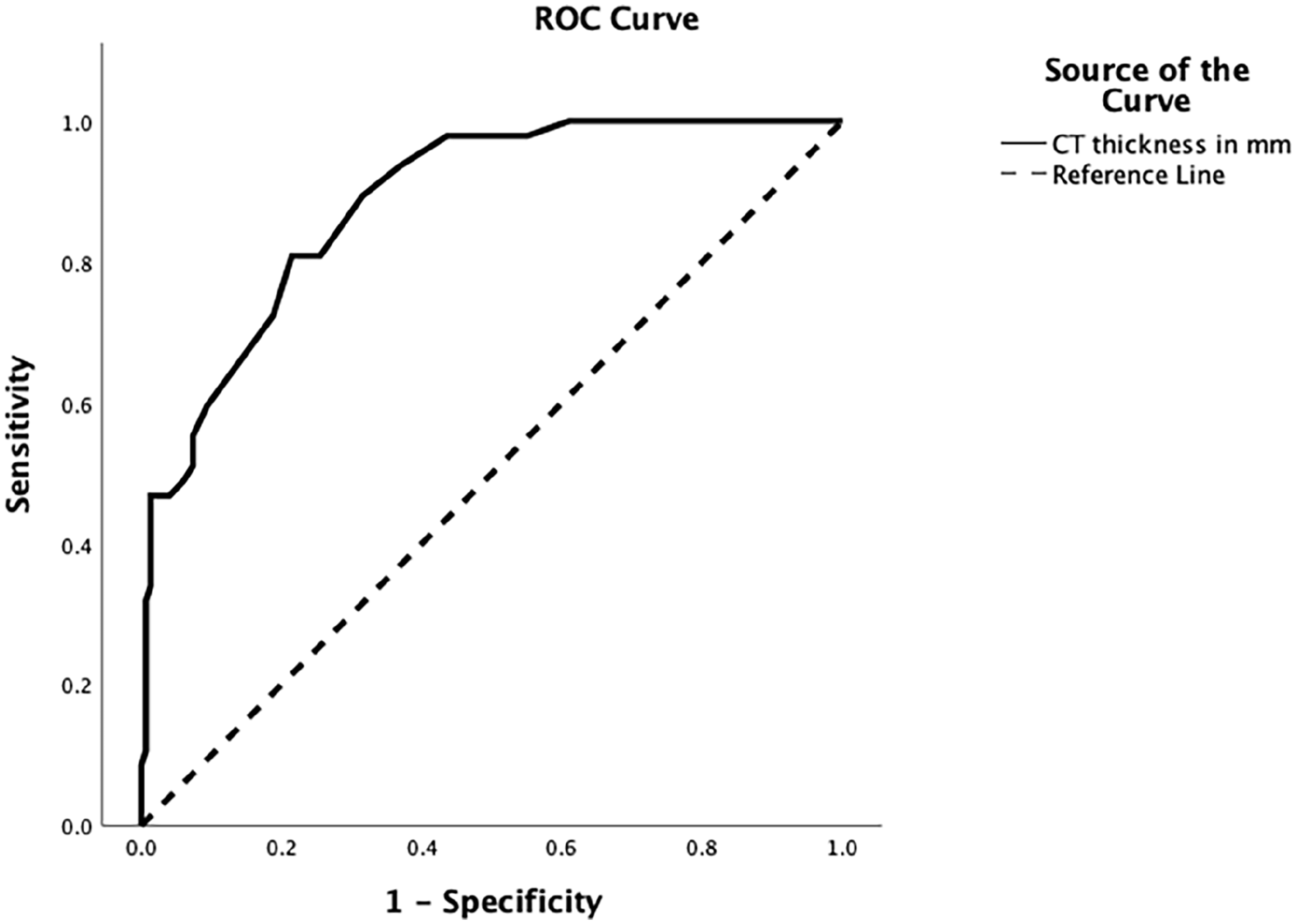
ROC analysis. The ROC curve demonstrates the diagnostic ability of CT-measured septal thickness to differentiate between “thin” and “thick” nasal septal mucoperichondrial flaps using the established cutoff value. CT, computed tomography. ROC, receiver operating characteristic.
Logistic Regression
Logistic regression identified age as a predictor for tear occurrence, with each year increasing the odds of no tear by 6.6% (P = .001, OR = 0.934), and the model’s overall fit is evaluated using the −2 log-likelihood, Cox & Snell, and Nagelkerke R Square values, alongside the Hosmer and Lemeshow Test, with a chi-square of 13.370 and a significance of .100, suggesting an adequate fit. The classification table shows the model’s predictive performance, with an overall percentage correct of 66.8%.
Table 1 delineates the comparative data on age and CT thickness pertaining to the “Thin” versus “Thick” classifications based on intraoperative assessments. Table 2 details the analysis of variables by CT Thickness Cut-off and statistical significance.
Comparative Data on Patient Age, Gender, and CT-Measured Septal Thickness.
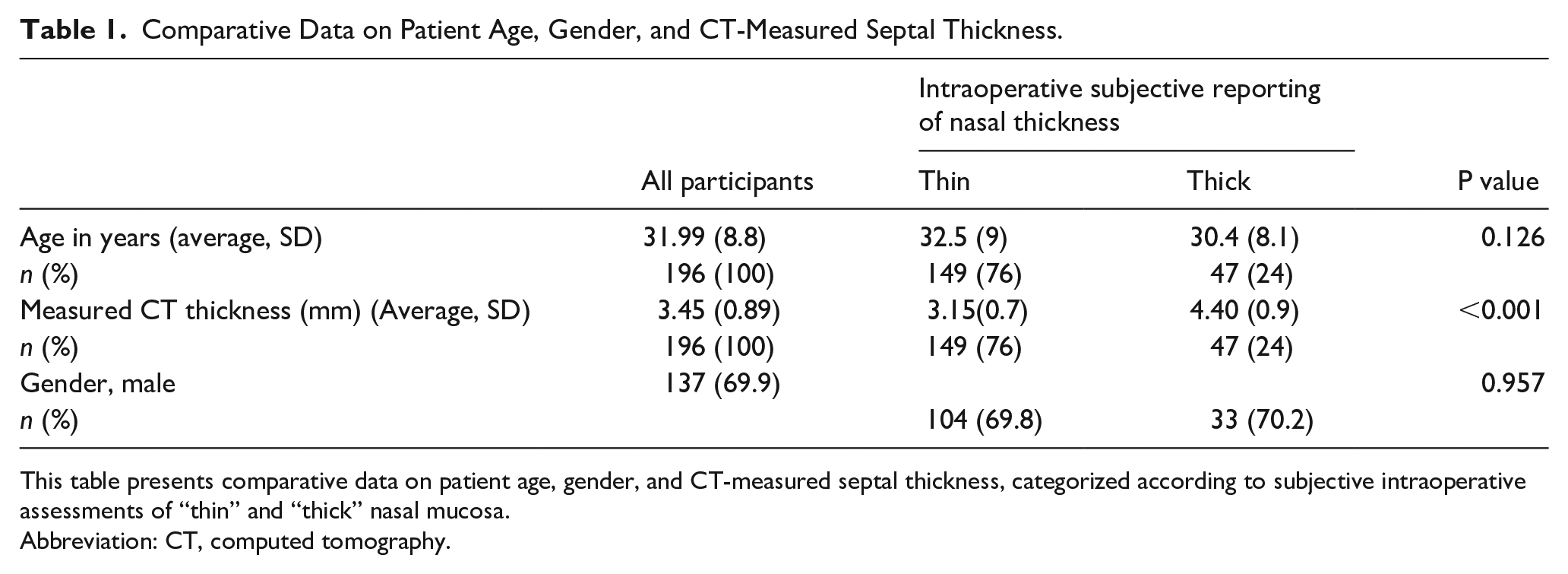
This table presents comparative data on patient age, gender, and CT-measured septal thickness, categorized according to subjective intraoperative assessments of “thin” and “thick” nasal mucosa.
Abbreviation: CT, computed tomography.
Analysis of Variables by CT Thickness Cut-off.
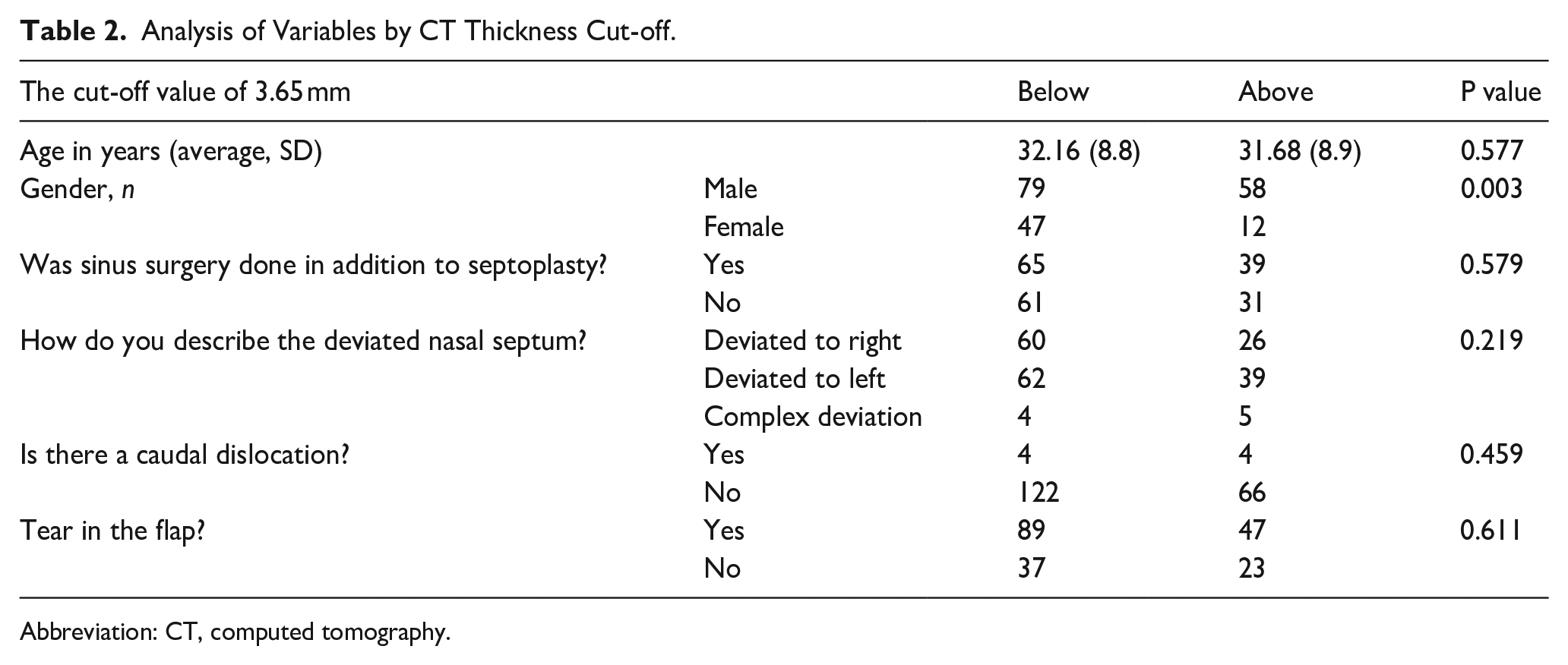
Abbreviation: CT, computed tomography.
Ethical Considerations
The study protocol was designed in adherence to ethical guidelines and was approved by the Institutional Review Board.
Discussion
The study findings indicate that using CT scans to measure septum thickness correlates well with intraoperative observations. A threshold of 3.65 mm effectively distinguishes between thin and thick flaps, exhibiting 80.9% sensitivity and 78.5% specificity, achieving an overall accuracy of 79.08%. These results highlight the utility of high-resolution CT imaging in preoperative assessments. However, our comprehensive literature review did not reveal any prior studies that categorize nasal septum thickness based on CT findings.
In a cadaver study utilizing Techlock GM-21 Calipergauze, the septal thickness was measured post-making parasagittal incisions to expose the septum. Variability in thickness was observed across different regions: the base anterior to the vomer was the thickest area, whereas a section just above the base was the thinnest. Measurements showed that the anterior-inferior region above the thinnest part was thinner compared to the superior-posterior part, indicating a gradient in septal cartilage thickness throughout the nasal septum. 5
The septal cartilage thickness in previous studies was observed to vary between 0.8 mm and 2.2 mm. Similarly, the mucosal thickness ranged significantly, from 0.3 mm to 3.7 mm, indicating a notable variability in these measurements across different parts of the nasal septum. 6 In the study by Thamboo et al., 7 thickness measurements were specifically taken at the thickest soft tissue areas on one side of the septum mucosa in various nasal regions. Recorded measurements showed an average anterior septum thickness of 3.28 mm (SD 0.13 mm) in control subjects, 3.0 mm (SD 0.13 mm) for Empty Nose Syndrome (ENS) patients, and 3.04 mm (SD 0.16 mm) for those with past inferior turbinate reduction without ENS, with no significant statistical difference between these groups.
In discussing the results of this study, we reflect on the alignment of subjective intraoperative assessments with objective CT measurements of nasal septum thickness. The study finds no significant difference in the age at surgery when comparing “Thin” versus “Thick” mucosa, while a significant difference in CT thickness between these groups is noted. Gender shows no significant influence on the subjective reporting of nasal thickness, and tear occurrence shows no correlation with subjective nasal thickness assessments. Notably, males exhibit thicker septum than females on CT.
Age differences between males and females at surgery are insignificant, while FESS with septoplasty is more common in older patients. A related study on complications in endoscopic sinus surgery patients identified the average age to be approximately 36 years. 8 Tear presence shows no significant correlation with CT thickness. The study also illustrates procedural trends with the majority of incisions on the left and the prevalence of small unilateral flap tears. Furthermore, the study introduces a standardized 3.65 mm cutoff for CT thickness classification with high sensitivity, specificity, and accuracy.
The significant association between gender and CT thickness classification after the 3.65 mm cutoff is discussed, revealing gender disparities in nasal septum thickness. Literature is lacking studies that directly compare nasal mucosa thickness between genders, making our findings particularly significant. Based on the results provided, females are more likely to have a “thin” nasal septum when using a cutoff value of 3.65 mm for septal thickness. The data show that out of 59 females, 47 (approximately 79.7%) fall under the “Below” category for thin septal mucosa, compared to 79 out of 137 males (approximately 57.7%) being classified as “Below.” Logistic regression highlights age as a significant predictor for the occurrence of tears during surgery, emphasizing the importance of age in preoperative planning. Logistic regression showed that each additional year decreases the risk of mucosal tears by 6.6%. This finding might seem counterintuitive since mucosal atrophy typically increases with age. However, the literature review reveals that age was not a significant risk factor for septal perforations in a study 1 involving 143 patients undergoing septoplasty or septorhinoplasty, where age did not differ significantly between those with or without perforations (P = .665). While not all mucosal tears lead to permanent septal perforations, further research is needed to thoroughly examine the impact of age on tear and perforation risk.
The ROC curve analysis revealed an AUC of 0.884, demonstrating the efficacy of CT in discriminating mucosal thickness. The established threshold of 3.65 mm is corroborated by its notable sensitivity and specificity, contributing to its clinical applicability. A high NPV underscores its effectiveness in correctly identifying “thin” mucosa, an essential clinical advantage. Conversely, the PPV suggests potential enhancements in detecting “thick” mucosa. Overall, the reliability of CT for preoperative evaluation is affirmed, although optimization could further its precision.
The discussion is enhanced by data visualizations, including ROC curves, which substantiate these findings. In addition, it acknowledges the necessity for continued research aimed at improving the predictability and prevention of surgical complications. These complications, particularly mucosal tears that could lead to nasal septal perforation, adversely affect patients’ quality of life. 9
The findings from this study have significant implications for clinical practice and patient care in nasal surgery. This is apparent when having the majority of patients with thin intraoperative NSMF as shown in the study 76%. The potential for CT scan measurements as a reliable preoperative assessment tool for nasal septal mucoperichondrial flap thickness is highlighted, which could facilitate surgical planning and potentially mitigate the risk of intraoperative complications like mucosal tears. Incorporating CT measurements alongside other known risk factors for septal perforation, such as untreated bilateral corresponding mucosal tears, could enhance the predictability and management of surgical outcomes. 1 The establishment of a 3.65 mm cutoff for distinguishing thin and thick flaps offers a practical guideline that could be generalized to improve surgical outcomes, Figure 5 shows an example of a thin and thick septum utilizing the cutoff value.
An example of thin (A) and thick septum (B) on CT scans. CT, computed tomography.
In Huntley et al.’s 10 research, among 21 patients, 52.4% (11 patients) experienced nasoseptal flap perforations during the harvesting process, with perforation sizes between 3 mm and 15 mm, averaging at 7.3 mm, primarily at the maxillary crest or septal spur. Despite these perforations, no postoperative cerebrospinal fluid leaks were reported. However, the findings’ broader applicability is limited due to the study’s small sample size and study design.
The resolution of CT scans introduces a potential limitation in accurately measuring the septum thickness. While high-resolution scans enhance detail, they may not eliminate inherent variability in measurements due to software limitations in precisely placing ruler borders. This limitation underscores the need for careful interpretation of CT-based thickness assessments and suggests the exploration of more direct or advanced measurement techniques as a future standard for accurate septum thickness evaluation.
In addition, factors like the nasal cycle or the use of decongestants, which might affect the septum thickness, warrant consideration in subsequent studies. 11 Incorporated into our study limitations, we acknowledge that due to the scarcity of prior research in this field, we were unable to estimate an a priori sample size. Consequently, we included all patients within a designated time frame instead.
Further research is warranted to affirm the proposed classification system and to investigate whether individuals with thinner septum are more susceptible to complications such as intraoperative tears, enduring septal perforations during septoplasty, and cerebrospinal fluid leaks in skull base repair utilizing nasoseptal flaps.
In conclusion, this study validates the use of a 3.65 mm threshold on CT scans to categorize nasal septal mucoperichondrial flaps as “thin” or “thick,” aligning well with surgical observations. This standardization could enhance surgical planning, reduce complications, and improve patient outcomes. The research encourages the integration of such measures in preoperative routines and calls for further studies to advance measurement methods for greater precision and clinical relevance.
Supplemental Material
sj-xlsx-1-ear-10.1177_01455613251332156 – Supplemental material for Computed Tomography Assessment of Nasal Septal Mucosa: Establishing Criteria for Thickness Classification
Supplemental material, sj-xlsx-1-ear-10.1177_01455613251332156 for Computed Tomography Assessment of Nasal Septal Mucosa: Establishing Criteria for Thickness Classification by Ahmad Alroqi, Fadi Mamdouh Arafeh, Mohammed Alyousef, Saud Alromaih and Saad Alsaleh in Ear, Nose & Throat Journal
Footnotes
Acknowledgements
We would like to acknowledge the use of ChatGPT, an AI language model developed by OpenAI, to assist in the editing and paraphrasing of this document to enhance clarity and readability. The intellectual content, analysis, and conclusions of this research were developed independently by the authors.
Statements and Declarations
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.