
Abstract
Chondromas are benign cartilaginous tumors that frequently occur in the long bones, pelvis, sternum, ribs, and scapula. They seldom develop in the head and neck region, and there have been rare reports of them arising in the nasal septum. Although the mainstay of management is surgery, surgical treatment strategies vary depending on the size, location, and extent of the disease. Herein, we describe a case of huge chondroma originated from the anterior nasal septum, which was completely removed by endoscopic septoplasty approach thorough modified Killian incision.
Introduction
A chondroma is a benign cartilaginous neoplasm predominantly composed of mature hyaline cartilage. 1 It is found mostly in the small bones of the hands and feet, although it can also occur in long, tubular bones, primarily the humerus, femur, and ribs. 2 However, chondromas rarely develop in the head and neck, especially in the nasal septum. 3 Although surgical excision is the treatment of choice for nasal septal chondroma, different approaches may be utilized depending on the size, location, and extent of the disease. 4 This case report describes huge chondroma arising from the anterior nasal septum, which was completely removed by endoscopic septoplasty approach thorough modified Killian incision. This study was approved by the institutional review board of Pusan National University Hospital.
Case Report
A 71-year-old woman was referred to our clinic with an incidentally found mass in the anterior nasal cavity. She had experienced progressive left nasal obstruction for 2 months. She had no relevant medical history and no other symptoms. Endoscopic examination showed a bulging lesion with a normal mucosa lining at the anterior septum (Figure 1). A computed tomography scan of the paranasal sinuses demonstrated a 3.0 × 2.3 × 3.0-cm sized lobulated mass in the anterior nasal septum extending to the bony defect on the hard palate. A deviation of the septum to the left side was also identified (Figure 2). On magnetic resonance imaging (MRI), a solid mass had intermediate signal intensity on T1-weighted images (T1WIs), high signal intensity on T2-weighted images, and capsular enhancement on gadolinium-T1WIs (Figure 3). Considering the location of tumor, transseptal endoscopic removal was performed under general anesthesia. At first, septoplasty began with modified Killian incision on the right side. After elevation of the mucoperichondrial flap, the deviated septal bone and cartilage were selectively removed, preserving an L-strut of dorsal and caudal cartilaginous septum at least 1.5 cm long. A firm to hard mass lesion was found on the inferior portion of the cartilaginous nasal septum. Results of a frozen biopsy reported low-grade cartilaginous tumor. It was well circumscribed and could be shelled out easily. The mass and cartilaginous nasal septum was completely removed with grasping forceps and D-knife under direct visualization using a nasal endoscope (Figure 4). There was a bony destruction on the hard palate and that lesion was drilled out without mucosa injury. Histological examination showed benign lesion consists of fibrous tissue and vessels with lacunae containing benign chondrocytes, consistent with chondroma (Figure 5). The patient had an uneventful recovery, and nasal obstruction disappeared. Endoscopic examinations and MRI performed 12 months postoperatively demonstrated no evidence of recurrence (Figure 6).
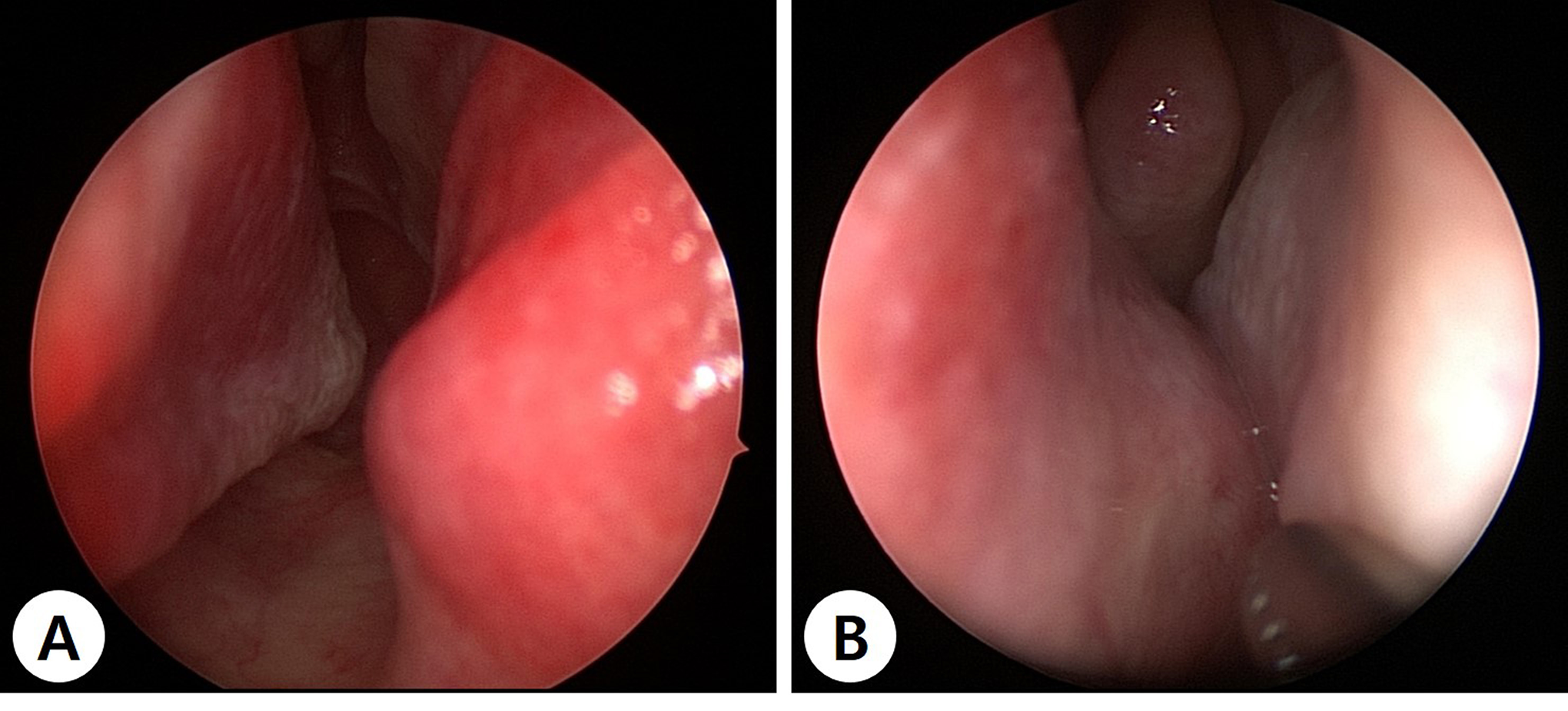
Preoperative endoscopic findings of nasal septal mass. Right (A) and left (B) nasal endoscopy shows a smooth-surfaced mass with a normal mucosa lining at the anterior nasal septum.
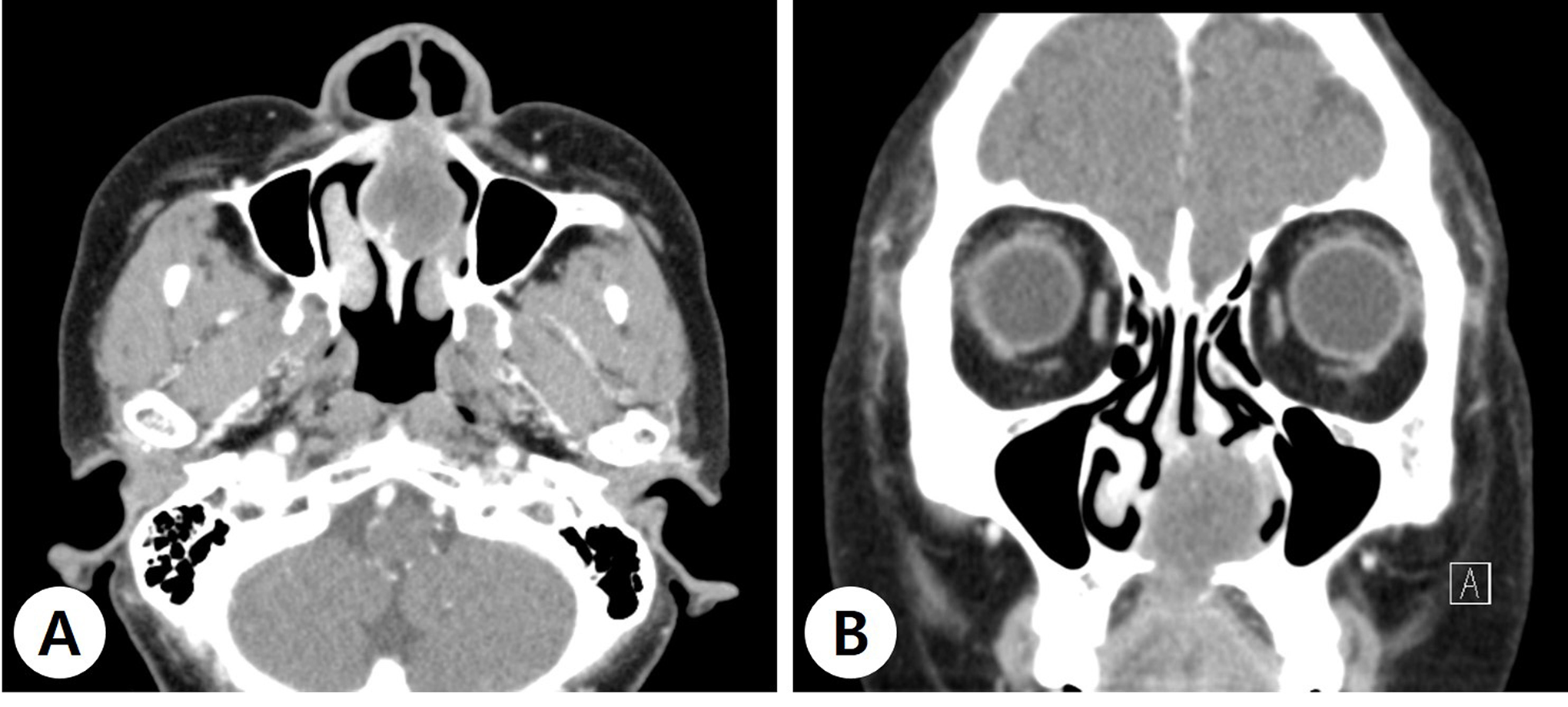
Preoperative paranasal sinus computed tomograms. Axial (A) and coronal (B) images show a 3.0 × 2.3 × 3.0-cm sized lobulated mass in the anterior nasal septum extending to the bony defect on the hard palate.
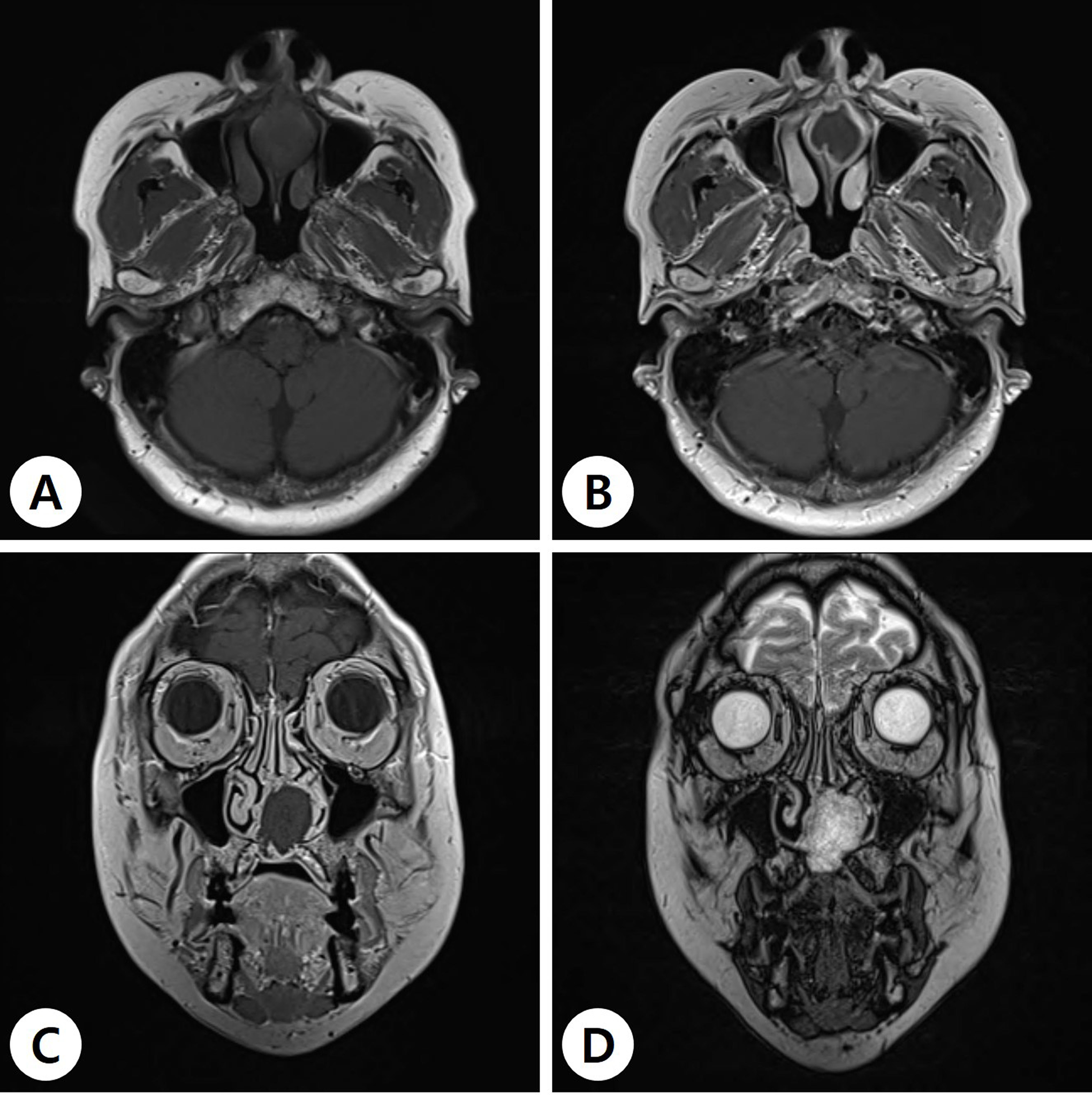
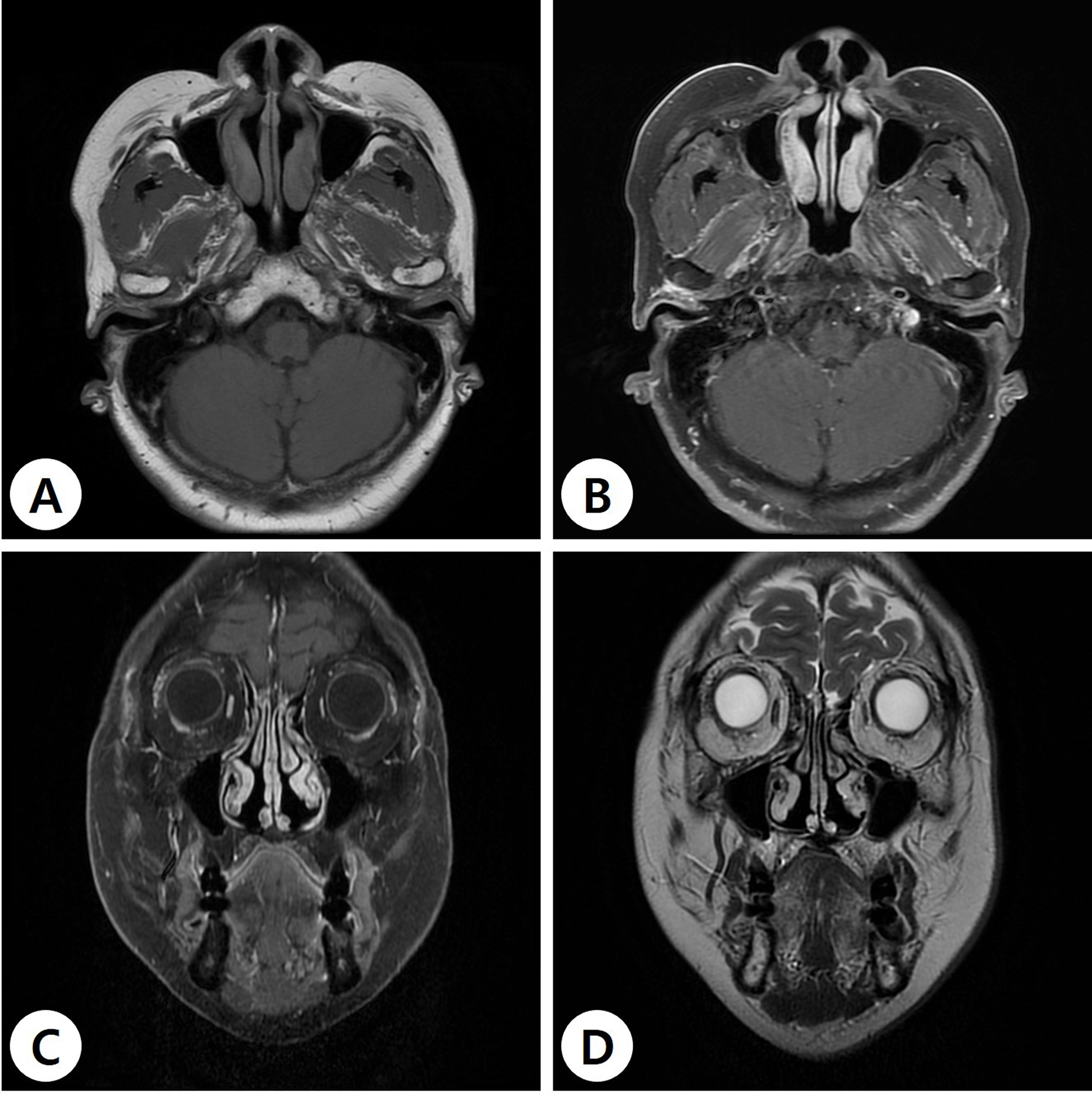
Preoperative paranasal sinus magnetic resonance images. The solid mass with scallop margin shows intermediate signal intensity on T1-weighted image (T1WI) (A), capsular enhancement on post-contrast T1WI (B, C), and high signal intensity on T2-weighted image (T2WI; D).
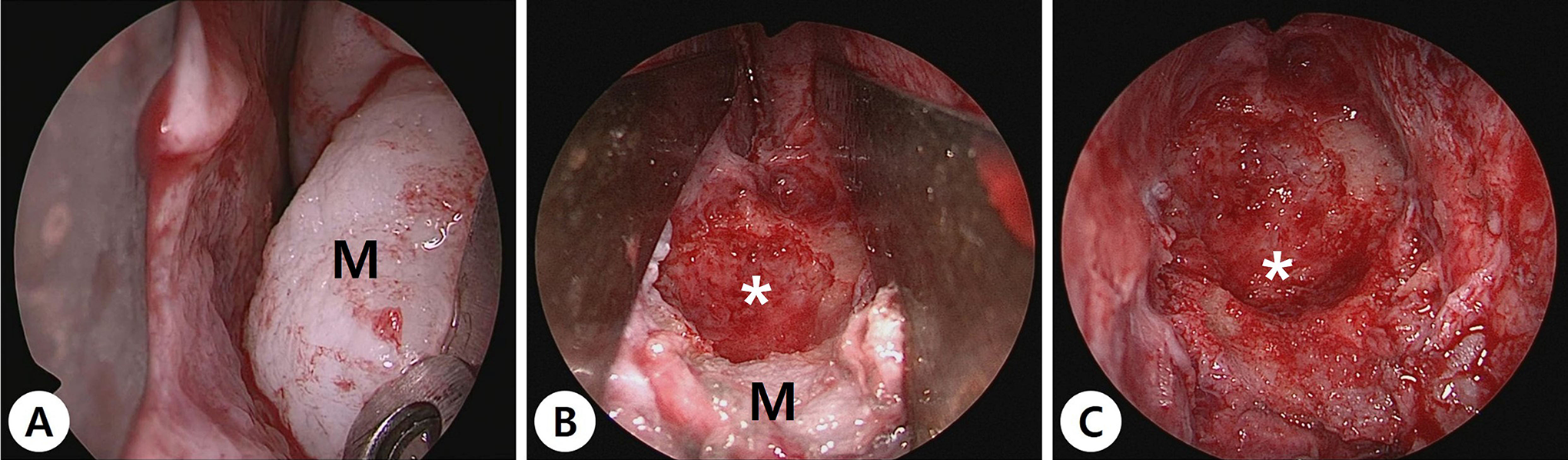
Intraoperative endoscopic findings via endoscopic septoplasty approach. (A) The whitish mass (M) is noted in the anterior nasal septum. (B) Most of firm mass is removed, and remnant mass is detected in the inferior portion of anterior nasal septum. (C) After complete removal of anterior nasal septal mass, bony dehiscence in noted in the hard palate (asterisk).
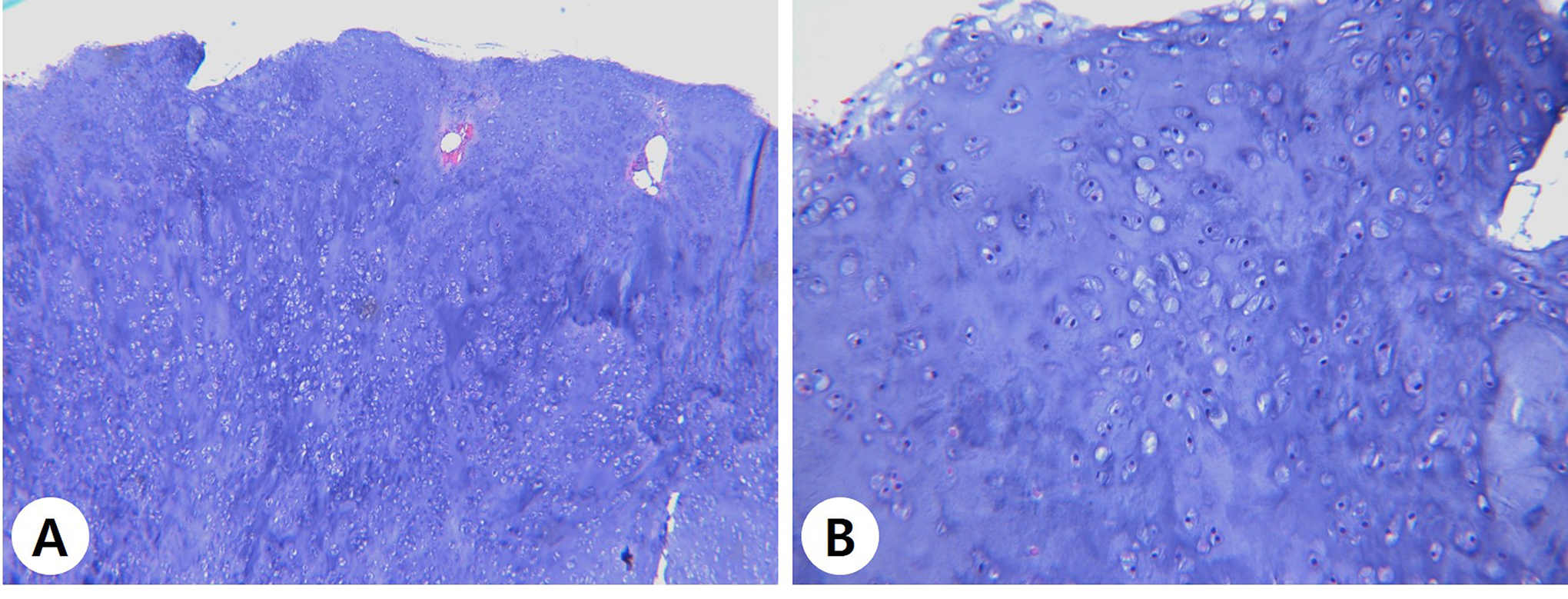
Histologic findings of chondroma. (A) The tumor is composed of fibrous tissue and vessels with lacunae containing benign chondrocytes (hematoxylin and eosin [H&E], ×40). (B) The chondrocytes exhibit minimal to mild cytological atypia (H&E, ×200).
Postoperative paranasal sinus magnetic resonance images. T1-weighted image (T1WI) (A), post-contrast T1WI (B, C), and T2-weighted image (T2WI; D) at postoperative 1 year show no evidence of remnant tumor or recurrence.
Discussion
Cartilaginous tumors are the second most common bone neoplasms. Only 10% of cases occur in the head and neck region. 3 The most common site in the head and neck is the ethmoid sinus, followed by the maxilla, larynx, nasal septum, hard palate, nasopharynx, and alar cartilage. 5 However, chondromas of the anterior nasal septum are extremely rare and almost always arise from the posterior bony septum. 4 The peak age at presentation is between 20 and 30 years, with no sex predilection. 5 The most accepted concept in the development of nasal chondroma is “cell rest theory,” which explains the chondrogenesis from paranasal sinuses, tubinates, hard palate, and posterior part of nasal septum. 2,4,5 Although trauma, metaplasia, and heredity may also play a role in the pathogenesis of the tumor, these were unlikely in this case due to the absence of a trauma history and the patient’s unremarkable family history. 4
The symptoms of nasal chondromas depend on the tumor’s location, size, and growth rate. Common presentations include nasal obstruction and epistaxis. 6 Extension into the orbits or maxilla may cause proptosis, epiphora, diplopia, blindness, displaced teeth, uneven jaws, and facial asymmetry. 5,6 However, nasal chondromas do not usually present with pain because they are benign lesions and slow-growing neoplasms. 5 In this case, the patient complained of nasal obstruction on left sides because nasal cavity was obstructed by a huge nasal septal chondroma with septal deviation.
The diagnosis is confirmed by histopathologic examination. The typical microscopic features of chondroma include small cartilage cells, pale vacuolated cytoplasm, and small dark-stained nuclei. 2,3 However, malignant tumors are twice as common as benign cartilaginous tumors in the head and neck region. 5,6 Therefore, careful consideration must be given to differentiate a chondroma from a low-grade chondrosarcoma. Malignant features such as necrosis, pleomorphism, or mitoses should be ruled out. Furthermore, the presence of anisocytosis should be identified as it could signify a transition stage from a chondroma to a low-grade chondrosarcoma. 4
Although the surgical excision is the treatment of choice, different approaches may be utilized depending on the size, location, and extent of disease. 2 A lateral rhinotomy approach is usually preferred for a large chondroma arising from anterior nasal septum or one with paranasal sinus involvement. 3,4 Although this approach affords excellent exposure of the nasal cavity mass, the lateral rhinotomy incision causes a large facial scar of the external skin. In the present case, endoscopic septoplasty approach was used to remove huge chondroma originated from the anterior nasal septum thorough modified Killian incision. This technique ensured complete exposure of the caudal end of the septum, wide excision of the anterior septal chondroma, and preservation of septal mucosa. However, regular follow-up is needed because, although rare, chondroma may undergo malignant transformation, with subsequent metastatic spread. 3,5
Despite the rarity of chondroma in the anterior nasal septum, it should be considered in the differential diagnosis of a nasal septal mass, especially with smooth surface and normal appearing mucosa. Complete surgical removal via endoscopic septoplasty approach may be considered for this lesion if possible, with maintaining the integrity of nasal septum and avoiding scarring.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.