
Abstract
Acute suppurative thyroiditis (AST) is a rare endocrine emergency, typically of bacterial origin, that can lead to significant morbidity and life-threatening complications. It is far less common than other inflammatory thyroid conditions, such as subacute thyroiditis, and may mimic noninfectious inflammatory disorders. Case 1 describes a 40-year-old man with a 5-day history of anterior neck swelling and odynophagia. Physical examination and imaging confirmed AST with retropharyngeal space involvement. He was treated with broad-spectrum intravenous antibiotics and thyroid abscess aspiration. Case 2 involved a patient with an 11-day history of fever and odynophagia. Imaging, including computed tomography and neck ultrasound, revealed a left thyroid lobe abscess extending into the retropharyngeal space. Further evaluation led to the diagnosis of a fourth branchial cleft cyst and a left pyriform fossa sinus tract. A multidisciplinary approach successfully managed both the acute infection and the underlying anatomical anomaly. Retropharyngeal extension of suppurative thyroiditis is exceedingly rare but signifies a severe disease progression with complex clinical implications. This report highlights the need to consider suppurative thyroiditis in the differential diagnosis of midline cervical infections.
Keywords
Introduction
Acute suppurative thyroiditis (AST) is an exceptional inflammatory condition of the thyroid gland that was significantly more common in the pre-antibiotic era. Although uncommon, its potential to cause substantial morbidity and life-threatening complications underscores the importance of prompt diagnosis and treatment. Here, we present 2 cases of AST complicated by retropharyngeal space involvement.
Case 1
A 40-year-old man presented with a 5-day history of midline neck swelling, odynophagia, chills, diaphoresis, and fatigue. His medical history was significant for Graves’ disease, previously treated with radioiodine (I-131) 7 years prior, with no subsequent follow-up. Physical examination revealed a warm, tender anterior neck mass.
Laboratory studies showed an elevated C-reactive protein level of 141 mg/L (reference: <5 mg/L), normal leukocyte count, and marked hypothyroidism. Contrast-enhanced neck computed tomography (CT) demonstrated a left-sided intrathyroidal hypodense area with an associated retropharyngeal space abscess (Figure 1A and B). Ultrasound-guided fine-needle aspiration (FNA) of the thyroid abscess yielded 3 mL of frank pus (Figure 1C). Cultures grew Streptococcus constellatus, Streptococcus anginosus, and Gemella bergeri with normal cytology.
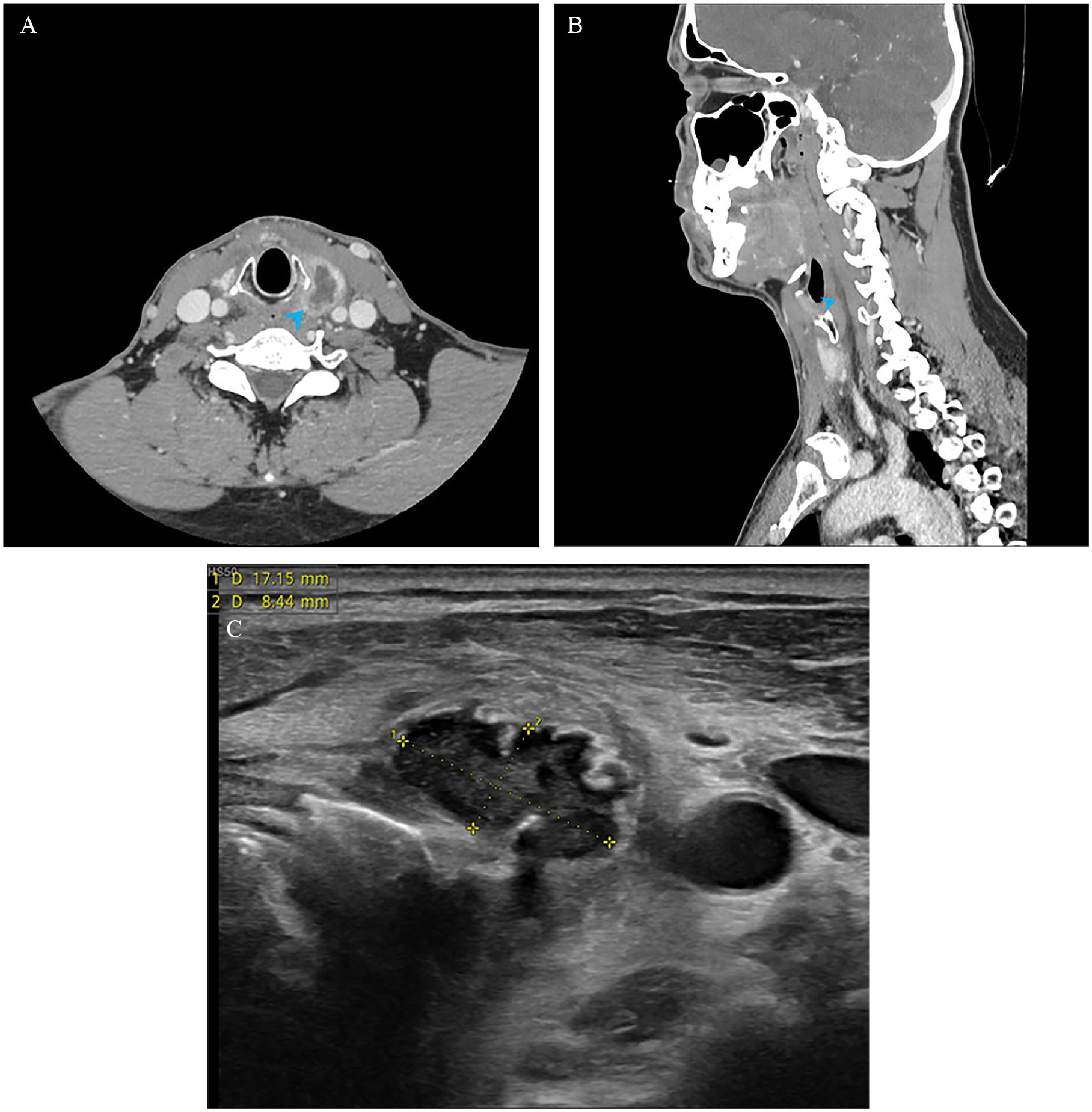
Computed tomography and ultrasound images of case 1. (A) Axial computed tomography shows a left intrathyroidal abscess with peripheral enhancement (arrowhead). (B) Midsagittal reformat of the same study reveals a rim-enhancing retropharyngeal abscess (arrowhead), extending from the level of the hyoid bone to the level of the seventh cervical vertebra. (C) Transverse ultrasound image at the level of thyroid gland displays a poorly defined 18 × 8 × 16 mm heterogeneous mass within the left thyroid lobe, consistent with a thyroidal abscess.
The patient was treated with a 5-day course of intravenous amoxicillin-clavulanic acid, leading to complete clinical resolution. Follow-up CT confirmed full resolution of the retropharyngeal abscess. A barium esophagram showed no evidence of a left pyriform fossa sinus tract.
Case 2
A 3-year-old boy with no prior medical history presented with an 11-day history of fever and worsening odynophagia. One week earlier, he had been evaluated in the emergency department and diagnosed with pharyngitis and left acute otitis media, for which he was prescribed oral amoxicillin.
Laboratory investigations revealed an elevated C-reactive protein level of 86 mg/L (reference: <5 mg/L) and a leukocyte count of 21.1 G/L (reference: 5.5–15.5 G/L) with 92% neutrophilia. Physical examination showed anterior cervical enlargement, which was firm and tender to palpation. Contrast-enhanced CT demonstrated a large retropharyngeal abscess and a hypodense lesion in the left thyroid lobe (Figure 2A and B).
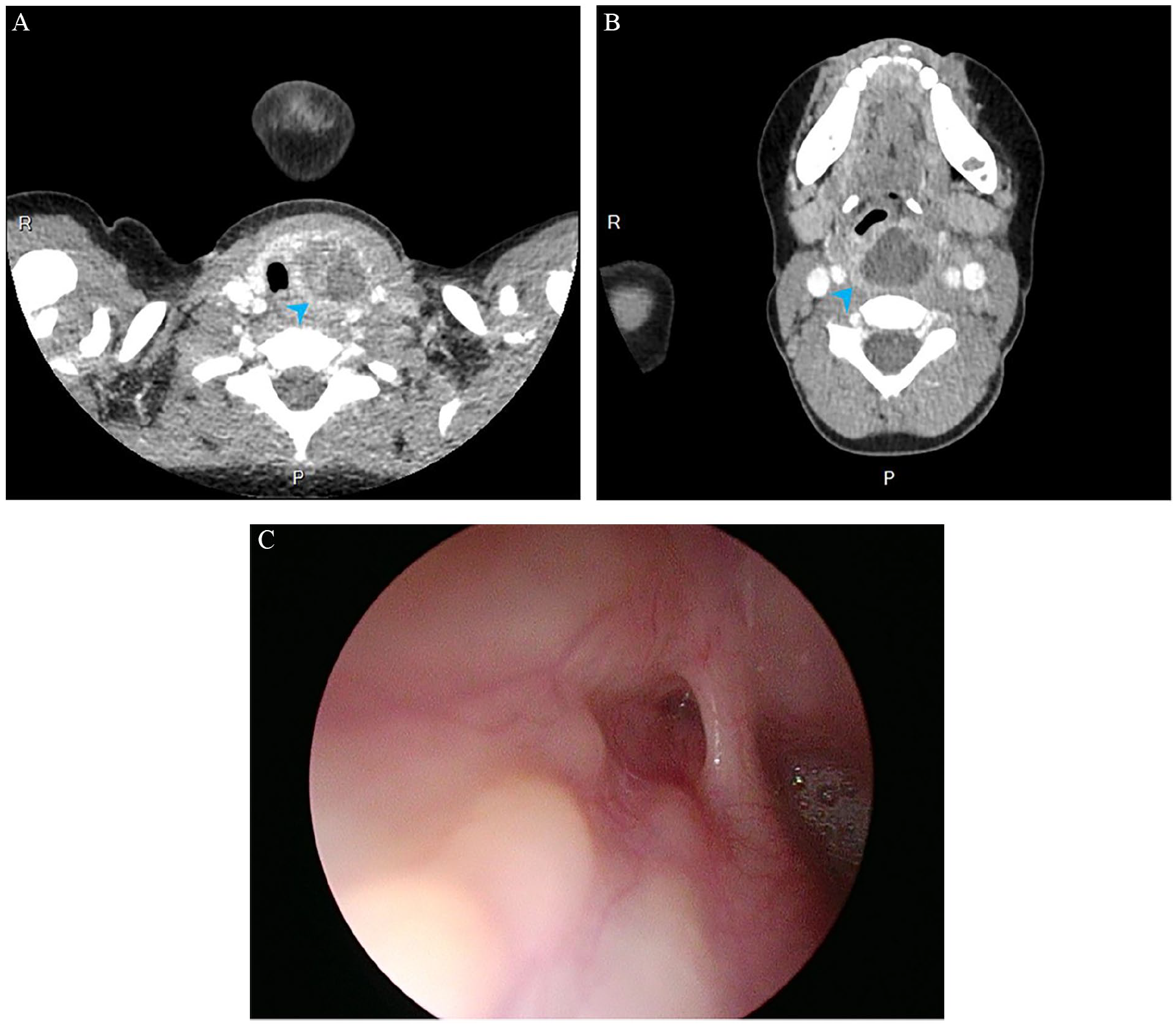
Computed tomography and endoscopic images of case 2. (A) Axial computed tomography demonstrates a left-side rim-enhancing intrathyroidal abscess (arrowhead) indenting and displacing the left thyroid lobe. The trachea is deviated to the right but not compressed. (B) Another axial computed tomographic image of the same study at the level of the hypopharynx shows a rim-enhancing, voluminous retropharyngeal abscess (arrowhead). (C) Endoscopic examination of the left piriform fossa reveals a pit at the piriform apex characteristic of a patent piriform fossa sinus tract, which was cauterized and subsequently sutured endoscopically during the same examination.
The patient underwent transoral incision and drainage of the retropharyngeal abscess along with ultrasound-guided needle aspiration of the left thyroid abscess. Cultures grew S. constellatus and S. anginosus with normal cytology. He showed significant postoperative improvement and received targeted intravenous antibiotic therapy based on sensitivity results. The patient was discharged on hospital day 7 with a course of oral antibiotics and follow-up instructions.
One month later, magnetic resonance imaging revealed a left infrahyoid cystic lesion consistent with a fourth branchial cleft cyst. Direct suspension laryngoscopy identified a left pyriform fossa sinus tract, which was managed with transoral cauterization using trichloroacetic acid followed by suturing with 5-0 Vicryl (Figure 2C). At the 1-month follow-up, the patient remained asymptomatic, with no signs of infection or abscess recurrence.
Discussion
AST with subsequent thyroid abscess formation represents a rare but potentially life-threatening endocrine emergency.1-11 Its true incidence is likely lower than the reported 0.1% of thyroid pathology due to case overlap and misclassification as subacute thyroiditis.1-11 The condition affects approximately 2 patients per year in large tertiary care centers.1-11
First described by Bauchet in 1857, AST exhibits a slight female predominance and has been reported across a wide range of ages.1-11 Its highest prevalence in women occurs during their childbearing years, potentially due to the higher incidence of thyroid neoplasia and hypertrophy in this population. In addition, physiological anatomical changes during puberty, menstruation, and pregnancy—such as moderate thyroid enlargement and increased vascularization—may contribute to increased susceptibility to infection.
The thyroid gland is relatively resistant to infection and direct bacteria inoculation. Proposed protective mechanisms include its rich blood and lymphatic supply, high iodine content, hydrogen peroxide production, and encapsulation within a fibrous capsule, all of which may inhibit thyroid suppuration.1,2,4-6,8-10
An occult pyriform fossa sinus tract and immunocompromised conditions—including Acquired Immunodeficiency Syndrome, hematologic malignancies, and uncontrolled diabetes—are well-documented risk factors for thyroid suppuration, with the latter being the most common overall.1-4,12 Additional predisposing factors include thyroglossal duct remnants facilitating midline infections, underlying thyroid disorders such as chronic autoimmune thyroiditis, goiter, and thyroid malignancy, as well as a patent foramen cecum and congenital branchial fistulas.1-4,12 Direct spread from adjacent suppurative infections, penetrating neck trauma, and invasive procedures such as FNA or thyroid biopsy have also been implicated.1-4,12
Infection may arise directly from the pretracheal space due to esophageal perforation, dental abscesses or their treatment, and systemic autoimmune disorders.1-4 9,10,12 In addition, cases of lymphatic or hematogenous spread from distant sites have been reported in the literature.5-9
Surgical site infections are extremely rare.5-9 Although wound infections occur in 0.3% to 2.4% of thyroid surgeries, the incidence of suppurative complications following thyroid procedures ranges from 0.1% to 1%.5-9
The pyriform fossa sinus tract, an uncommon third and fourth branchial anomaly, presents with diverse clinical and imaging features, often making diagnosis challenging. 13 It typically manifests as left-sided suppurative thyroiditis but can also appear prenatally or in the neonatal period as a cystic neck mass, potentially leading to airway compromise and respiratory distress. 13 This anomaly is more common in children and young adults and is associated with recurrent infections.2,10,13
In pediatric cases of suppurative thyroiditis, the presence of a narrow sinus tract is generally suspected, as it can intermittently trap food residue, secretions, and oropharyngeal flora, predisposing the thyroid to infection. 13 Infectious thyroiditis is often preceded by an upper respiratory infection, which may trigger inflammation of the sinus tract and facilitate pathogen transmission to the thyroid gland.
All children with recurrent or left-sided suppurative thyroiditis—even those experiencing their first episode, without left-sided involvement, or with bilateral disease—should undergo thorough evaluation for a pyriform fossa sinus tract.2,10,12-15 Barium esophagram is the most sensitive imaging modality, with direct endoscopic visualization serving as a secondary approach.2,10,12-15 Up to 70% of pediatric patients with suppurative thyroiditis may have an underlying pyriform fossa sinus tract.2,10,12-15
Congenital anatomical anomalies should be considered in all patients with thyroid abscesses, regardless of age.2,10,12-15 A multimodal diagnostic approach, including both ultrasound and esophagram, is often necessary for confirmation.12-15 Recently, minimally invasive transoral endoscopic cauterization has emerged as the preferred treatment for sinus tract closure, offering outcomes comparable to open surgery with lower morbidity and fewer complications.12-15 This procedure is frequently performed during the initial endoscopic diagnostic evaluation.12-15
AST is most commonly caused by bacterial pathogens, primarily gram-positive organisms, in immunocompetent individuals.1-12,16 By contrast, infections due to fungi, parasites, or viruses are more frequently observed in immunocompromised patients, tend to be chronic and insidious, and typically present after a prolonged symptom duration.1-12,16 In adults, Staphylococcus aureus and Streptococcus pyogenes account for more than 80% of cases and are the sole pathogens in over 70% of infections.1-12,16 In pediatric patients, alpha- and beta-hemolytic Streptococcus and various anaerobes are implicated in approximately 70% of cases, though mixed infections are identified in more than 50%.1-12,16 In addition, gram-negative anaerobic bacilli are increasingly recognized as causative pathogens in suppurative thyroiditis.1-12,16
AST typically presents with the abrupt onset of painful, asymmetric, and predominantly left-sided anterior neck enlargement, which moves during swallowing.1-12 This is associated with local inflammatory signs, level VI lymphadenopathy, and fever.1-12 Additional symptoms may include limited cervical extension, involuntary depression of the chin during swallowing, dysphagia, dysphonia, and drooling. In rare cases, dyspnea and stridor may occur, necessitating urgent tracheostomy.1-12 Systemic toxicity signs may also be present. Symptoms typically develop over several days to a few weeks.1-12 A thyroid abscess may, though rarely, present as a pulsatile mass. 17 In children, symptoms are often more pronounced than in adults.
Laboratory findings usually show leukocytosis with a left shift and elevated acute inflammatory markers.1-12 Thyroid function varies depending on the etiology and time course of the thyroiditis. Although transient or permanent hypothyroidism or even thyroid storm may occur as a result of the disease or its treatment, euthyroidism is most commonly observed.1-12 Patients with fungal thyroiditis, characterized by diffuse inflammation and necrosis, are likely to be hypothyroid, while those with mycobacterial infections are more likely to present with hyperthyroidism.1-12
In Case 1, the patient’s history of Graves’ disease, treated with radioactive iodine therapy 7 years prior, is relevant, as this treatment often leads to hypothyroidism. Studies have shown that most patients develop hypothyroidism within the first year post-treatment. 18 Therefore, the patient’s hypothyroidism may be attributed to the prior therapy or could result from the AST itself, as the infectious process can impair thyroid function.
If left untreated, AST can result in mortality rates of up to 12%, with fungal infections having the highest mortality at 33%, making timely diagnosis essential.1-12 Several studies report that up to 12% of patients present with severe thyroiditis requiring intensive care unit admission.1-12
Although rare, local and systemic complications can arise from the disease process or inadequate or delayed treatment, and these complications can be life-threatening. Potential sequelae include airway compromise due to extrinsic compression or perforation of the trachea, retropharyngeal space involvement, or laryngeal edema necessitating tracheostomy.1-12 Other complications may include internal jugular vein thrombophlebitis, cutaneous fistula, Horner’s syndrome, transient vocal cord paralysis, abscess rupture leading to pneumonia, descending mediastinitis, pericarditis, sepsis, and death.1-12 Rheumatic fever has also been reported following group A beta-hemolytic streptococcal thyroiditis.1-12 The thyroid’s close proximity to the retropharyngeal space allows for the spread of infection through fascial planes and lymphatic channels, facilitating the progression of complications.
Painful thyroiditis encompasses infectious thyroiditis, subacute thyroiditis, traumatic thyroiditis, and radiation-induced thyroiditis. Subacute thyroiditis is the most common cause of thyroidal pain, typically presenting with transient thyrotoxicosis, followed by transient hypothyroidism and, in most cases, eventual euthyroidism.2,4,6-10 It is a self-limiting condition that may present with similar local signs to AST, though systemic manifestations tend to be less severe.2,4,6-10
The differential diagnosis for painful thyroiditis also includes hemorrhage into a thyroid cyst or nodule, fulminant thyroid carcinoma (usually anaplastic), painful Hashimoto’s thyroiditis, amiodarone-induced thyroiditis, and radiation-induced thyroiditis.2,4,6-10 Nonthyroidal causes of neck pain include infected thyroglossal duct or branchial cyst, cervical adenitis, anterior cervical cellulitis, perichondritis of laryngeal cartilage, infected cystic hygroma, and globus hystericus.2,4,6-10
Thyroid ultrasonography is the imaging modality of choice for evaluating AST. It is essential for detecting the spread of infection to contiguous structures, defining the anatomy in preparation for surgical exploration, guiding radiologically assisted drainage of a thyroid abscess, and monitoring the response to antibiotic therapy. Characteristic findings on ultrasound vary depending on the phase of AST but typically include a unifocal perithyroidal hypoechoic space, effacement of the plane around the thyroid gland, and a hypoechoic area within the thyroid.1-3,10-12
Ultrasound-guided FNA biopsy is the gold standard diagnostic test for managing AST.1-3,10-12 It allows access to both intra- and extra-thyroidal abscesses for gram stain, culture, and cytologic examination.1-3,10-12 FNA can help differentiate subacute thyroiditis in cases with a thyrotoxic presentation and exclude other thyroid pathologies, including malignancy.1-3,10-12 In addition, it can be performed to relieve pressure on a displaced trachea in patients with compromised airways.1-3,10-12
The cornerstone of management for AST includes blood cultures, aspiration or surgical drainage of pus, and prompt intravenous empirical broad-spectrum antibiotic therapy.1-4,10-12 Appropriate antibiotic regimens include clindamycin alone, a combination of penicillin and a beta-lactamase inhibitor, or a combination of metronidazole and a macrolide.1-4,10-12,16 Antifungal therapy should be added to the initial regimen in immunocompromised individuals.1-4,10-12,16 If there is extensive involvement of nearby structures, surgical debridement may be required. Managing the underlying predisposing conditions is also crucial for optimal outcomes.
Conclusion
This case report emphasizes that AST, though rare, can progress to involve the retropharyngeal space, presenting significant diagnostic and management challenges. It underscores the importance of considering congenital anatomical anomalies in patients with thyroid abscesses, regardless of their age. AST should be included in the differential diagnosis for any patient presenting with midline neck swelling. A thorough and proactive treatment approach, including prompt diagnosis, appropriate imaging, and timely interventions, is crucial for ensuring optimal patient outcomes, particularly when complicated by anatomical anomalies or retropharyngeal space involvement.