
Abstract
Riedel’s thyroiditis is a rare inflammatory disease characterized by extensive fibrosis, often mimicking malignancy. The concurrent presence of Riedel’s thyroiditis with noninvasive follicular neoplasm with papillary-like nuclear features (NIFTP) is exceptionally rare and has not been previously reported. A 63-year-old male presented with an acute onset anterior cervical mass, fever, and dysphagia. Imaging revealed a large cystic mass in the right thyroid lobe extending into the mediastinum. Initial treatment with antibiotics led to partial improvement, but persistent swelling necessitated a deferred total thyroidectomy. Intraoperatively, the thyroid gland was fibrotic and adherent to surrounding structures. Histopathological examination confirmed Riedel’s thyroiditis with extrathyroidal extension and an underlying NIFTP. Postoperatively, the patient developed left vocal cord paresis and primary hypoparathyroidism. Systemic fibrotic involvement was ruled out through a thoracoabdominal-pelvic computed tomography (CT) scan. This case highlights the diagnostic challenges, atypical presentation, and management strategies of this unique coexistence, initially masquerading as a thyroid abscess.
Introduction
Riedel’s thyroiditis is a rare, chronic inflammatory disease of the thyroid gland characterized by the replacement of normal thyroid tissue with dense fibrosis. It was first described by the German surgeon Bernhard Riedel in 1896. This condition is exceptionally rare, occurring in only 0.06% of all thyroidectomies, with most reports limited to case studies and small case series.
The fibro-inflammatory process in Riedel’s thyroiditis extends beyond the thyroid gland, often involving surrounding vital structures, leading to compressive symptoms and endocrine dysfunction. It may also be associated with various systemic fibrotic disorders.1,2
Due to the firm nature of the mass, diagnosis can be challenging without biopsy and histopathological confirmation, as Riedel’s thyroiditis may closely resemble anaplastic thyroid cancer, thyroid angiosarcoma, or lymphoma.3,4 In the literature, only a few cases have been reported with the concurrent presence of Riedel’s thyroiditis and other thyroid diseases. However, there have been no reported cases of Riedel’s thyroiditis occurring alongside a noninvasive follicular thyroid neoplasm with papillary-like nuclear features (NIFTP).
We present a rare case of Riedel’s thyroiditis associated with NIFTP, highlighting the diagnostic challenges and an unusual presentation mimicking a thyroid abscess.
Case Presentation
A 63-year-old male patient was admitted to the ENT department with an anterior basicervical tumor that had been developing for approximately 1 week, associated with fever and dysphagia. His medical history included hypertension, diabetes, and hepatitis B. Two weeks before admission, he had a viral infection. He did not report dysphonia or clinical signs of dysthyroidism. On physical examination, a firm, poorly-defined, and painful 5 cm basicervical mass was noted, which was mobile with swallowing (Figure 1A).
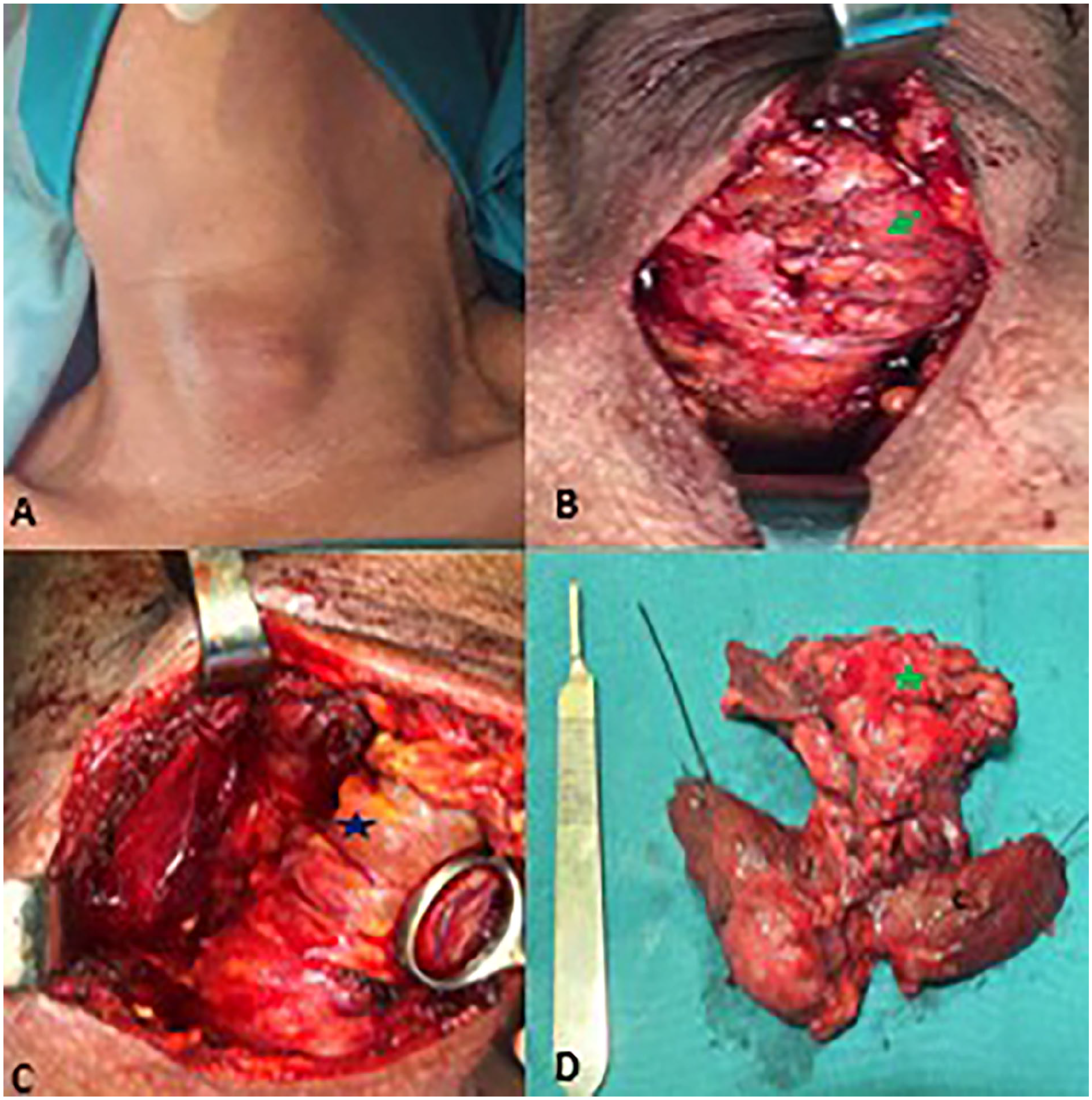
(A) Physical examination: a 5 cm firm mass at the lower cervix with local inflammatory signs. (B) Preoperative view: after subcutaneous dissection: it is noted that the infrahyoid muscles are infiltrated and unrecognizable (green arrow). (C) The right lobe is fibrosed and harbors an inferior nodule (blue star). (D) Specimen of total thyroidectomy extended to the infrahyoid muscles (green star).
Inflammatory signs extended into the mediastinal region. No suspicious cervical lymph nodes were detected. Biochemical analysis revealed peripheral hyperthyroidism with negative thyroid autoantibodies and elevated inflammatory markers.
Cervical CT imaging detected a 42 × 60 mm right isthmo-lobular cystic mass extending into the mediastinum and exerting a mass effect on the trachea (Figure 2).
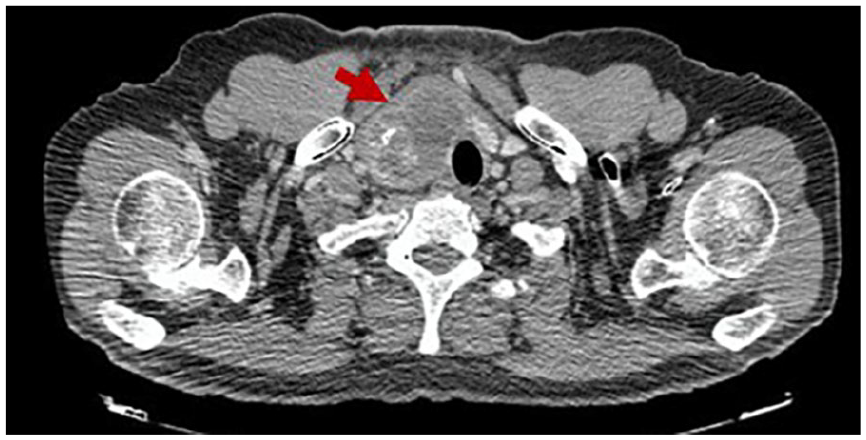
Cervical CT scan: The right thyroid lobe is completely occupied by a hypodense mass exerting a mass effect on the trachea.
The patient received a 17 day course of antibiotic therapy, leading to improvement in the local condition, although a 3 cm residual swelling persisted. A deferred total thyroidectomy was subsequently performed.
Intraoperatively, the thyroid gland was hard, fibrotic, and adherent to the subhyoid muscles, with a 4 cm nodule in both lobes (Figure 1B-D).
Histopathological examination confirmed Riedel’s thyroiditis affecting both thyroid lobes with extrathyroidal extension, involvement of the subhyoid muscles and perithyroid soft tissue, and underlying goiter. Additionally, a NIFTP was identified, along with multiple vesicular adenomas. The inflammatory infiltrate was composed of fibrosis-rich lymphocytes, plasma cells, histiocytes, and neutrophils (Figure 3).
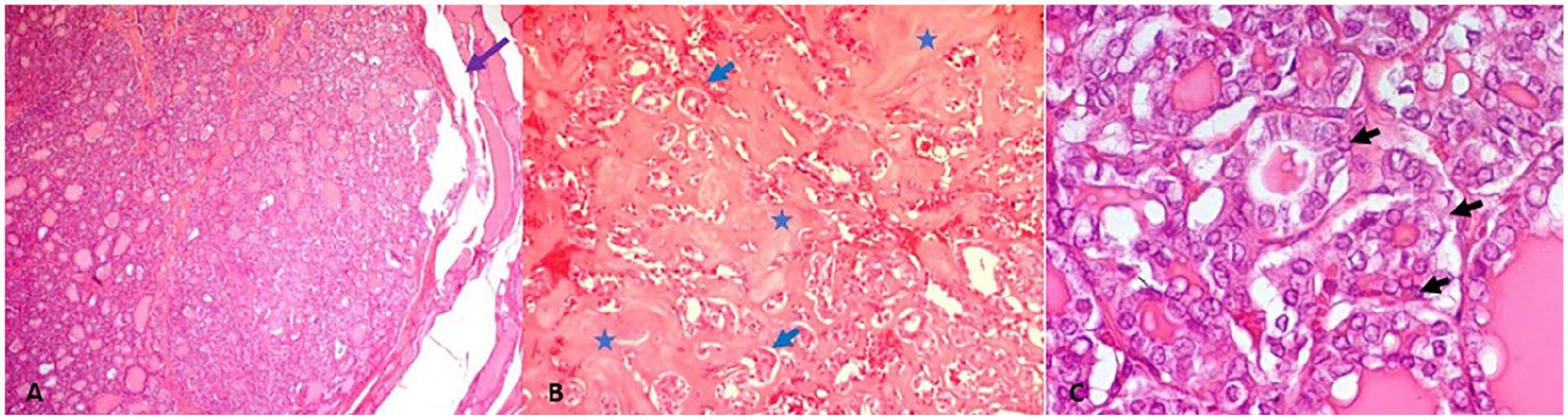
Histologic features: (A, HE ×40) the nodule is finely encapsulated, supporting the diagnosis of NIFTP. (B, HE ×100) Atrophic follicular structures (blue arrow) are observed, with marked peripheral fibrosis (blue star). The presence of dense fibrosis with glandular atrophy is suggestive of Riedel’s thyroiditis. (C, HE ×400) Follicular cells exhibit nuclear atypia (black arrows), consistent with noninvasive follicular thyroid neoplasm with papillary-like nuclear features.
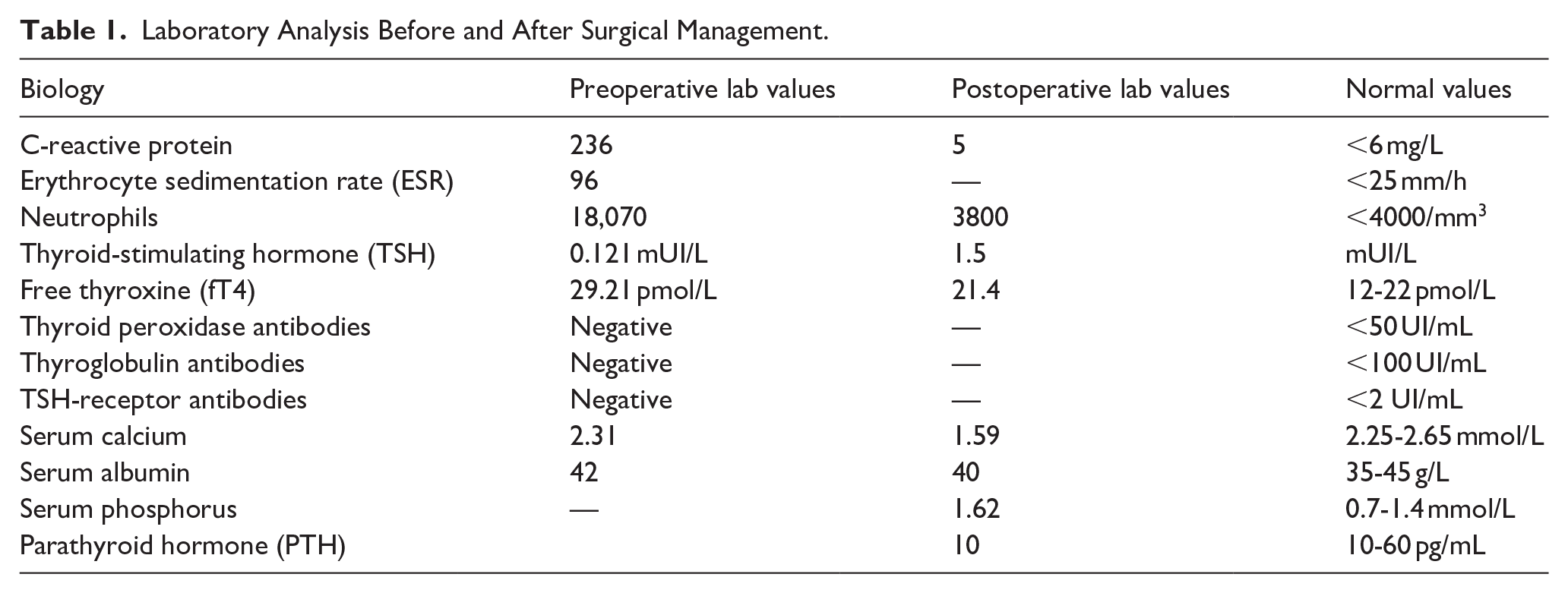
Postoperatively, the patient developed left vocal cord paresis. Levothyroxine replacement therapy was initiated at a dose of 150 µg/day. Early-postoperative hypocalcemia was observed (Table 1), with a low parathyroid hormone level confirming primary hypoparathyroidism. The patient was started on calcium supplementation and alfacalcidol, which successfully normalized serum calcium levels. He was referred to the endocrinology department for a follow-up.
Laboratory Analysis Before and After Surgical Management.
Additionally, the patient developed trigger finger in the left second digit postoperatively, which was treated with corticosteroid injections, leading to symptomatic improvement. A thoracoabdominal-pelvic CT scan was performed and showed no evidence of systemic fibrosis.
Discussion
Riedel’s thyroiditis is a rare chronic thyroid disease with an estimated incidence of 1.06 cases per 100,000 people and occurs in approximately 0.06% of thyroidectomies. At the Mayo Clinic, over 64 years until 1985, a study identified only 37 cases of Riedel’s thyroiditis among 57,000 thyroid surgeries, highlighting the rarity of the disease. Just like other thyroid disorders, Riedel’s thyroiditis predominantly affects women, with a female-to-male ratio of 4:1. 1 Reported patient being a male does not coincide with gender distribution. At Mayo, Riedel’s thyroiditis tends to affect individuals aged 30 to 60 years.2,3,5
The pathophysiology of Riedel’s thyroiditis remains controversial. The exact etiology of the condition is not known, but the current view favors it to be an autoimmune disorder or a local manifestation of a systemic fibrotic process based on the association of Riedel’s thyroiditis with other fibro-inflammatory conditions like retroperitoneal fibrosis, mediastinal fibrosis, sclerosing cholangitis.1,5 While genetic factors, viruses (eg, Epstein-Barr), and smoking have been suggested, no strong evidence supports these hypotheses.
Currently, the systemic autoimmune hypothesis has the most support and Riedel thyroiditis is now often classified as part of IgG4-related disease. 1 The study conducted by Dahlgren et al revealed that tissue analysis from Riedel’s thyroiditis patients has shown elevated IgG4:IgG ratios (44%-56% in some cases), although not universally across all cases.3,5
Presentation and diagnosis are often complex. It commonly manifests as a painless, hard goiter with local compression symptoms, such as dyspnea, stridor, hoarse voice, and dysphagia.2 -4,6
Our patient’s initial acute presentation over a few days was atypical. Clinico-biological parameters and cervical ultrasonography suggested a thyroid abscess, warranting initial antibiotic therapy. This represents an exceptional presentation of RT, rarely documented in the literature. Geissler et al reported a similar case of a patient with a rapidly-evolving obstructive goiter over 1 week, secondary to a sterile abscess within Riedel’s thyroiditis. 7
An alternative hypothesis is an associated subacute thyroiditis, given the patient’s history of viral infection, local inflammatory signs, and elevated erythrocyte sedimentation rate. This possibility is further supported by the presence of mild initial hyperthyroidism. The coexistence of Riedel’s thyroiditis with subacute thyroiditis is exceedingly rare, with only a few cases reported in the literature. 8
The presentation of Riedel’s thyroiditis might also mimics an invasive thyroid malignancy, which may coexist with Riedel’s thyroiditis, including papillary thyroid carcinoma, anaplastic thyroid carcinoma, thyroid sarcoma, and lymphoma.
Histopathological examination of the surgical specimen revealed a dense inflammatory infiltrate, diffuse vascular obstruction within fibrotic foci, and areas of necrosis. These findings are consistent with underlying subacute thyroiditis and may partly explain the acute onset of goiter in our patient.
On the other hand, the association of Riedel’s thyroiditis with a thyroid nodule has been rarely reported in the literature. Ozgur et al documented the first case of asymptomatic Riedel’s thyroiditis associated with a benign follicular adenoma. 2 This would represent the second reported case in the literature of a concomitant association between Riedel’s thyroiditis and thyroid follicular adenomas. Estimates as high as 38% associate Riedel’s thyroiditis with similar fibro-sclerotic processes in other areas. 5 The lesions appear in the lacrimal glands, orbits, parotid glands, mediastinum, coronary arteries, retroperitoneal tissues, bile ducts, and pancreas in varying combinations in the syndrome of multifocal fibro-sclerositis. 3 Fibrosing involvement of the pituitary gland has also been reported by Davies et al.2,9
Biochemical abnormalities often include hypothyroidism and hypocalcemia.2,5 The progression of fibrosis in the thyroid correlates with the onset of primary hypothyroidism, which occurs in 25% to 80% of patients. 1
Preoperative evaluations of thyroid function and calcium-phosphorus metabolism were normal, confirming that the primary hypoparathyroidism and hypothyroidism in our case were iatrogenic rather than resulting from fibrous invasion of the thyroid and parathyroid glands. Furthermore, clinical, laboratory, and radiological investigations revealed no systemic fibrosing involvement other than Riedel’s thyroiditis. The presence of a trigger finger in our patient is likely attributable to thyroid dysfunction, as several authors have reported an association between musculoskeletal manifestations and thyroid disease, particularly hypothyroidism.10,11
The concurrent presence of Riedel’s thyroiditis and other thyroid diseases has been reported. In the present case, Riedel’s thyroiditis was additionally accompanied by a NIFTP, which is a recently-defined thyroid nodule category characterized by follicular architecture with papillary nuclear features but lacking classical papillary carcinoma features like papillae or psammoma bodies.
At the molecular level, NIFTP is characterized by the absence of BRAF V600E mutations, as well as other high-risk mutations. 12
According to the ATA guidelines on thyroid nodules and differentiated thyroid cancer, thyroid lobectomy is generally sufficient for managing NIFTP. In our case, however, the diagnosis of NIFTP was made incidentally following histological examination after a total thyroidectomy. Rare cases of an association between Riedel’s thyroiditis and papillary carcinoma have been reported.12 -14
To our knowledge, this is the first reported case of NIFTP combined with Riedel’s thyroiditis. The European Society for Medical Oncology considers NIFTP to have a low risk of recurrence and recommends follow-up similar to that for low-risk papillary thyroid carcinoma. 15 Thyroglobulin assay and cervical ultrasound were planned in the follow-up of the patient.
Regarding the treatment of Riedel’s thyroiditis, no standardized protocol exists due to the rarity of the disease and the lack of outcome studies. Partial or total thyroidectomy is reserved for cases with compressive symptoms; however, surgical intervention is challenging because of extensive fibrosis and has been complicated in 39% of cases by left vocal cord paresis and hypoparathyroidism as observed in our case. Since recurrence is not uncommon in Riedel’s thyroiditis, various therapeutic options are available. These include glucocorticoids, immunosuppressants such as mycophenolate mofetil, selective estrogen receptor modulators like tamoxifen, and rituximab for severe or refractory cases. 16
Approximately one-third of patients may develop other fibrosing disorders within 10 years, although disease-specific mortality is rare. Nevertheless, long-term and close monitoring is essential, to detect potential relapses or the development of extrathyroidal fibrosing symptoms.1,2
In our case, given the improvement in compressive symptoms, it was decided to re-evaluate the patient over time—clinically, biochemically, and by cervical ultrasound—and to maintain him solely on substitution therapy for his hypothyroidism and hypoparathyroidism.
Conclusion
In summary, this case emphasizes the intricate interplay of multiple disorders underscoring the complexity of managing thyroid diseases. It highlights the possible simultaneous occurrence of Riedel’s thyroiditis with NIFTP and follicular adenoma in a single patient, while also showcasing the overlapping manifestations of Riedel’s thyroiditis with subacute thyroiditis, which can further complicate diagnosis and treatment. This case highlights the need for multidisciplinary approach and tailored management strategies to optimize patient outcomes.