
Abstract
Subcutaneous cervical emphysema refers to the presence of air or gas trapped beneath the skin in the neck or cervical region. It typically occurs when air is introduced into the tissues due to trauma, infection, or medical procedures that disrupt the respiratory tract. Diagnosis is based on clinical presentation in addition to chest and neck radiographic examinations. Subcutaneous cervical emphysema resulting from swimming is extremely rare, and patients may be asymptomatic or present with crepitus, neck swelling, and dysphonia. In severe cases, life-threatening complications can occur, such as airway compromise or tension pneumothorax. The authors of this manuscript report a rare case of a 9-year-old female, previously healthy, who presented with subcutaneous cervical emphysema following a swimming training session. This patient was followed up for 1 month with conservative management and experienced self-resolution of her symptoms. Early diagnosis, monitoring, and initiation of treatment are highly recommended to prevent any long-term or life-threatening complications.
Introduction
Emphysema is a condition characterized by the abnormal presence of air within body tissues. 1 Air expansion can affect both subcutaneous and deeper tissues, with the latter posing a greater risk for clinical deterioration. This can lead to serious complications including pneumomediastinum, pneumoperitoneum, pneumoretroperitoneum, pneumothorax, and possibly respiratory and cardiovascular collapse. 2 Subcutaneous emphysema is the presence of air in the subcutaneous layer of skin and can result from different etiologies. 3
Cervical emphysema specifically describes the presence of air in the face and neck region. It was first described by Knott in 1850, mainly due to increased intrathoracic pressure associated with acute and chronic underlying lung disease. 4 Although this etiology remains the most common, several others have been reported in the literature, including trauma or iatrogenic injuries related to the use of instruments in the upper aerodigestive tract, traumatic intubation, or head and neck surgery. 4 In rare cases, a pathological cause could involve a life-threatening infection of the neck spaces with gas-forming bacteria.
Although there are several reported cases resulting from diving—where alveolar rupture occurs due to the higher pressure of gases in the lungs compared to atmospheric pressure—there are very few cases resulting from swimming.5,6 This study aims to report a case of cervical subcutaneous emphysema resulting from swimming and to review the literature.
Case Report
A 9-year-old girl presented to her pediatrician with bilateral neck swelling, more severe on the right. She had no respiratory distress, no sore throat, and no hoarseness. The swelling occurred immediately after swimming practice. The patient is a swimmer and swims daily for 2 to 3 hours. Recently, she had participated in a competition that required intense workouts.
Her pediatrician ordered a computed tomography (CT) scan of the neck and referred her to our clinic. Physical examination was unremarkable except for bilateral neck crepitus involving levels 2 to 5. Flexible fiberoptic laryngoscopy revealed no abnormalities. A CT scan of the neck showed the presence of bilateral subcutaneous emphysema, more prominent on the right side, involving the superficial and deep fat planes of the neck. The emphysema extended to the superficial layer of the deep cervical fascia surrounding the sternocleidomastoid muscles and superiorly to the submandibular, masticator, jugolo-carotid, para-pharyngeal and parotid spaces (See Figures 1 and 2).
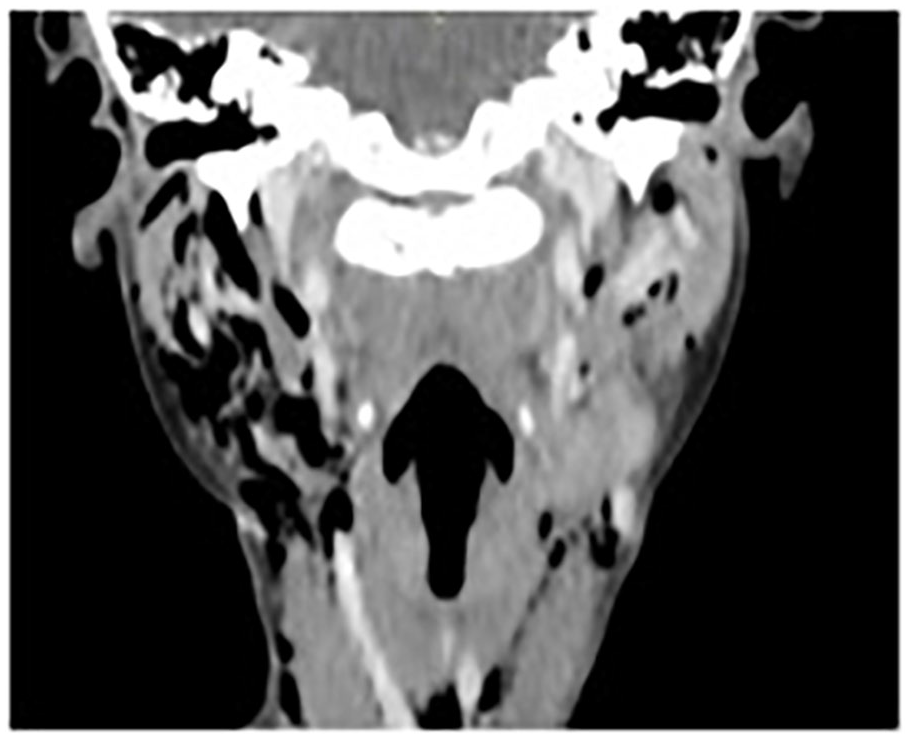
A coronal cut of the CT neck shows the presence of bilateral subcutaneous emphysema, right more than left, in the superficial and deep fat planes of the neck. CT, computed tomography.
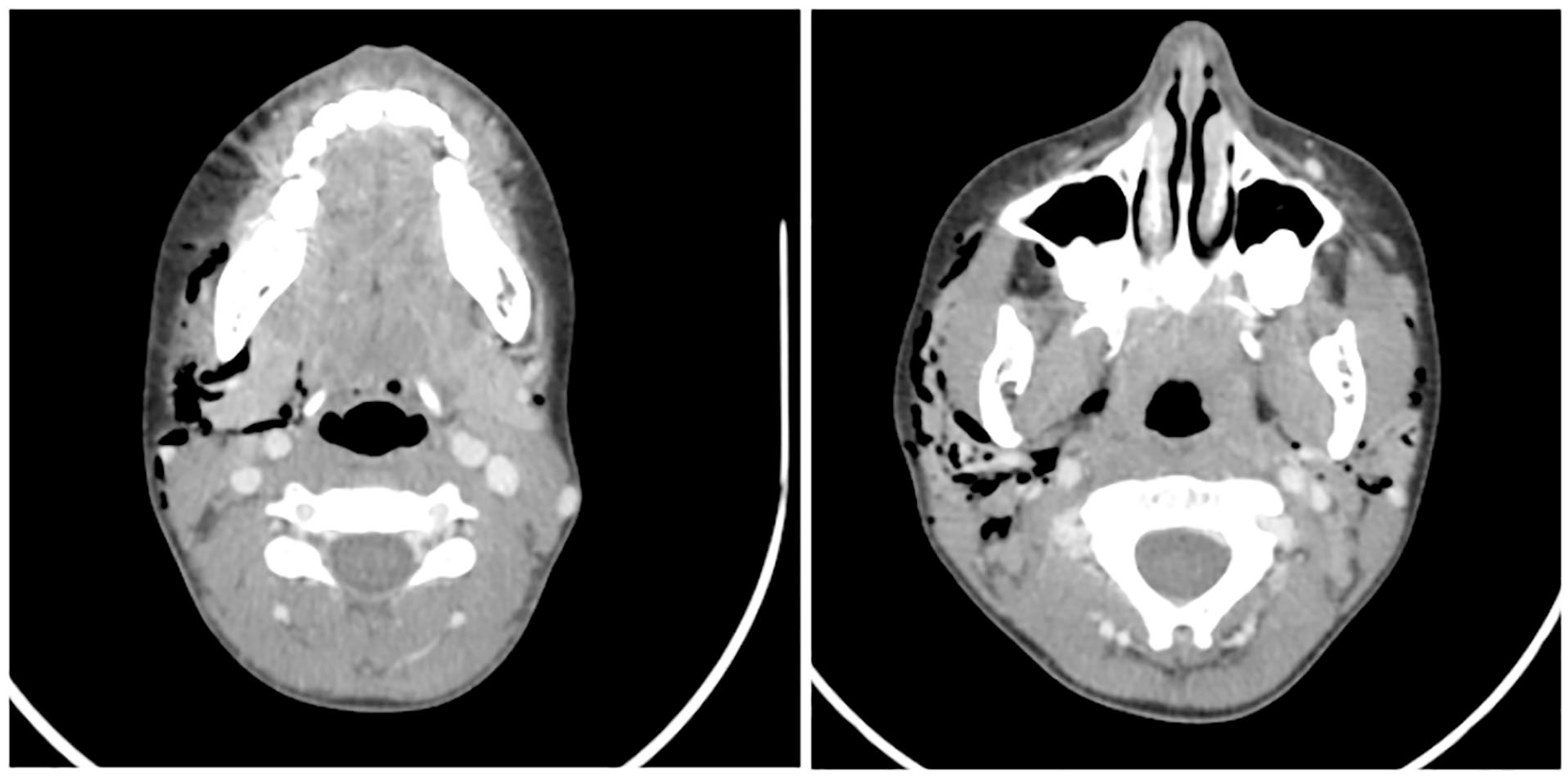
Subcutaneous emphysema involving the superficial layer of the deep cervical fascia surrounding the sternocleidomastoid muscles extending superiorly to involve the submandibular, masticator, jugolo-carotid, para-pharyngeal, and parotid spaces.
Following our first visit, the patient was conservatively managed with analgesia and was advised to avoid physical exertion, as she was asymptomatic. After 1 week, the patient showed complete resolution of her symptoms. However, 3 weeks later, she resumed swimming and experienced another episode of subcutaneous emphysema, though less severe. At this point, the decision was made to stop swimming for 1 month, after which her symptoms self-resolved. She then resumed her usual workout routine with no further episodes. Written informed consent was obtained from the patient’s parents for anonymized information to be published in this article.
Discussion
The development of subcutaneous emphysema is believed to result from various pathophysiologies. Injury to the parietal pleura allows air to pass into the pleural and subcutaneous tissues. 2 Alveolar rupture causes air from the alveolus to spread into the endovascular sheath and from the lung hilum into the endothoracic fascia, spreading to the cervical viscera and other connected tissue planes. 2 Air can also originate from external sources, such as gas-forming bacteria in necrotizing infections. 2 Once present in the subcutaneous areas, air preferentially accumulates in regions with the least tension until pressure increases enough to dissect along other planes, causing extensive spread.
Clinically, patients with cervical subcutaneous emphysema can present with dysphonia, neck swelling, crepitus, odynophagia, dyspnea, and pain.1,4 Presentation and severity of symptoms can vary widely depending on the degree of cervical emphysema present and occasionally, patients can be asymptomatic. In severe cases, life-threatening complications such as airway compromise or tension pneumothorax may occur. 4 Treatment depends on the severity of each case, ranging from conservative management with analgesia and avoidance of intense physical activity to tracheostomy with surgical dissection of facial planes. 7 Oxygen supplementation therapy has been associated with a more rapid recovery, although prophylactic antibiotics remain controversial. 4 Most studies recommend antibiotic treatment only if infection is suspected. 1
In the literature, most cases of cervical subcutaneous emphysema and pneumomediastinum are reported in divers, where the pathophysiology involves increased intrathoracic pressure leading to alveolar rupture. A similar mechanism is seen in swimmers, as described in a 1999 case report of a 19-year-old collegiate swimmer who developed pneumomediastinum following strenuous swimming and breath-holding exercises. The swimmer presented with anterior neck pain and dyspnea, and imaging revealed free air in the cervical and mediastinal tissues. Management involved temporary cessation of athletic activity, with a full resolution of symptoms. 8
Another case report from 2005 described a 12-year-old synchronized swimmer who developed pneumomediastinum due to repetitive Valsalva maneuvers during prolonged training. The authors highlighted the significant physical demands of synchronized swimming and the role of breath-holding in increasing intrathoracic pressure, which can result in alveolar rupture. In this case, conservative management with oxygen therapy and observation led to a complete resolution of symptoms within a few days. 9
In 2014, Lowrie et al reported an unusual case of spontaneous cervical emphysema following swimming. To the best of our knowledge, this is the only other reported case of isolated cervical subcutaneous emphysema in the literature. Lowrie et al described a case of a 17-year-old male patient who presented to the emergency department with a sore throat, odynophagia, and dysphonia, the day after his routine swimming training session and was found to have cervical emphysema. He was conservatively managed with complete resolution of symptoms. 4 Similar to our patient, the symptoms were mild and did not warrant intervention. Close observation and monitoring for worsening respiratory signs and symptoms were a key factor in treatment until our patient fully recovered. Initial assessment of any patient with suspected subcutaneous emphysema includes a soft tissue radiograph of the chest and neck. CT is not indicated unless greater detail or surgical intervention is warranted. 4
Our patient’s presentation aligns with these reported cases, where repetitive physical exertion and minor non-traumatic events, such as swimming, can induce subcutaneous emphysema or pneumomediastinum. Although the etiology in this case was low impact, it underscores the importance of recognizing subtle clinical presentations and monitoring for complications. Close observation and avoidance of physical exertion are critical in preventing symptom recurrence. In addition, our case adds to the limited literature on cervical subcutaneous emphysema due to swimming, emphasizing the role of repetitive swimming practice and competitive training as potential triggers.
Return-to-play considerations in sports-related pneumomediastinum remain controversial, with no clear guidelines. Some studies recommend a gradual return to activity after 7 to 10 days of symptom resolution, with follow-up imaging to rule out complications such as pneumothorax. Our approach aligned with this recommendation, as we temporarily restricted swimming until symptoms resolved and gradually resumed activity. 8
This case demonstrates that cervical subcutaneous emphysema, while rare in swimmers, should remain in the differential diagnosis for athletes presenting with neck pain, swelling, and crepitus, particularly after exertional activities involving breath-holding.
Conclusion
The authors report a rare case of cervical subcutaneous emphysema following a swimming session. Patients typically present with dysphonia, odynophagia, dyspnea, and neck swelling. Severe cases require careful observation for life-threatening complications such as airway compromise or tension pneumothorax. Diagnosis is mainly clinical, with initial assessment using chest and neck radiographs. Conservative management, including analgesia, oxygen therapy, and observation, is recommended for mild cases. Severe cases may require tracheostomy and surgical intervention.
Footnotes
Acknowledgements
None.
Ethical Considerations
Our institution does not require ethics approval for reporting individual cases. Written informed consent was obtained from the patient’s parents for the publication of this article.
Author Contributions
J.A.C.: literature review, data collection, manuscript writing – original draft. I.C.: literature review, data collection, manuscript writing – original draft. R.J.: literature review, manuscript writing – review and editing. R.A.B.: conception, supervision, manuscript writing – review and editing.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The data that support the findings of this study are available from the author or corresponding author upon reasonable request.