
Abstract
Introduction
Over the past few decades, the incidence of thyroid cancer has been rapidly increasing worldwide. 1 Owing to the increasing use of ultrasound, many early thyroid tumors have been discovered, most of which have a good prognosis after surgery. 2 Therefore, patients are paying more attention to improving their quality of life after surgery. In the past 20 years, various endoscopic surgeries based on mature surgical techniques and good therapeutic effects have been developed and successfully applied to the treatment of benign lesions and early differentiated thyroid cancer to reduce the occurrence of cervical scars. 3
At present, many thyroid surgeries can be completed through the oral cavity, areola, chest and breast, axilla, subclavicular, or trans ear approaches, each with its own advantages and disadvantages in implementation. 4 The transoral approach can thoroughly clean the central lymph nodes and without external scarring to the body, 5 whereas other endoscopic thyroid surgeries through other approaches will still leave varying degrees of scars on relevant parts of the body.
However, all approaches other than the transoral approach involve clean incisions, which do not have an increased risk of infection. Transoral thyroid surgery involves a clean-contaminated incision, raising concerns about postoperative infection. Since this surgery was created for cosmetic needs, any increase in the rate of infection would undoubtedly indicate failure of the surgery. Therefore, most of the time, clinicians continue to administer intravenous and oral antibiotics after surgery to prevent infection. 6 Owing to the lack of evidence, the use of antibiotics during the perioperative period has not been standardized and has been highly controversial. Anuwong et al analyzed the infection rates of 425 patients who underwent oral endoscopic thyroid surgery and reported that none of these patients developed signs of infection after surgery. However, this approach involved the use of a large amount of antibiotics. 7 It is still unknown whether transoral thyroid surgery can be performed without antibiotics.
In the current era of increasing bacterial resistance, the necessity of perioperative antibiotic use needs further exploration to minimize the unnecessary use of antimicrobial drugs. Some studies have reported that the flora in the oral cavity are nonpathogenic bacteria, which theoretically do not cause local infections to increase. However, whether these flora can reproduce in the operative cavity still needs further verification.8,9 Our center has gradually reduced the use of antibiotics in patients and has routinely cultured the drainage fluid in the surgical cavity to understand the growth of bacteria in surgical wounds after transoral surgery. Therefore, this study aims to explore whether the use of antibiotics can be reduced after transoral endoscopic thyroidectomy vestibular approach (TOETVA), providing some reference for clinical practice.
Materials and Methods
Research Object
A retrospective study was conducted on patients with thyroid tumors who were diagnosed with surgical treatment at the Head and Neck Surgery Department of Tongren Hospital from 2022 to 2024. The inclusion criteria were stage T1 papillary thyroid carcinoma or unilateral benign nodules <4 cm with cosmetic needs and no other contraindications.
Surgical Techniques and Perioperative Management
In the experimental group, a transoral vestibular approach and a CO2 inflatable cavity-building method were used. The neck surgical area was disinfected with iodophor, and the oral cavity was rinsed with 1:10 diluted iodophor water, chlorhexidine, and normal saline before surgery. The control group underwent operations through the axillary, subclavian, and retroauricular approaches via a suspended cavity-building method. The surgical area was disinfected with iodophor before the operation. A drainage tube was placed in all patients with different approaches and was kept in place for 3 to 5 days postoperatively. When the drainage fluid volume decreased to 20 mL/24 h, the drain was removed, and the patient was discharged. Drainage fluid was collected from all patients for bacterial culture on the first day after surgery. The bacterial cultures included Gram-stained white blood cells, Gram-stained bacteria, common bacterial cultures, fungal cultures, and anaerobic bacterial cultures.
Among all patients who underwent transoral endoscopic thyroidectomy, antibiotics were routinely prescribed after surgery due to initial concerns about infection. However, as our skills and experience continued to improve, we have reduced postoperative antibiotic use, instead promptly recording patient’s condition after surgery. Antibiotics are now only used when evidence of local infection appears. This allows the division of patients who underwent oral-endoscopic thyroid surgery into two groups for comparison: the group that received antibiotics after surgery and the group that did not receive antibiotics after surgery.
Statistical Analysis
All the statistical methods used in this study were conducted using SPSS 20.0 (IBM, USA). For continuous numerical data, the mean ± standard deviation was used, and the differences between groups were analyzed using independent sample t tests. For noncontinuous variable data, a chi-square test was used for analysis. P < .05 was considered statistically significant.
Results
Basic Demographic Data Statistics
A total of 43 patients with clean incisions and 102 patients with clean-contaminated incisions who underwent transoral endoscopic thyroidectomy were included in the study. Among them, there were 9 males and 34 females with a mean age of 36.6 ± 9.6 years for clean incisions. Among those with clean-contaminated incisions, 17 were males and 85 females—with an overall average age of 35.3 ± 8.0 years. Among all clean-contaminated incisions, 62 patients were treated with antibiotics, mainly cephalosporins, after surgery. Only 7 patients were treated with either levofloxacin hydrochloride or Bactrim due to allergies to cephalosporins. There were 40 patients in the clean-contaminated group that did not require treatment with antibiotics.
Comparison of Postoperative Infection Rates
Among the patients with clean-contaminated incisions, 61 of the 62 patients who received antibiotics after surgery did not develop postoperative infections. One patient developed symptoms of infection, resulting in an infection rate of 1.6%. Among the 40 patients who did not receive antibiotics, the infection rate was 0%, with no statistically significant difference (χ2 = 0.652, P = .420). In addition, there was no postoperative infection in 43 patients with clean incisions, which were not significantly different from the 1% postoperative infection rate of clean-contaminated incisions (χ2 = 0.424, P = .515).
Comparison of Bacterial Culture Results Between the Two Groups of Clean-Contaminated Incisions
In the group that were administered antibiotics, 11 patients exhibited a significant amount of Gram-positive leukocytes, 10 patients exhibited a moderate amount of Gram-positive leukocytes, and 41 patients presented a small number of, occasional, or no visible leukocytes. Eight patients had G+ bacteria, 49 patients had no G+ or G− bacteria, and 5 patients had G− bacteria. Both anaerobic bacteria and fungal cultures were negative. The results of the standard culture were as follows: 48 cases were negative, and 14 cases were positive, including 1 case of Oslo Moraxella, 1 case of Acinetobacter baumannii and Acinetobacter lwoffii, 1 case of coagulase-negative Staphylococcus, 1 case of caput medusae Staphylococcus, 1 case of 10% human Staphylococcus and 90% O. moraxella, 1 case of grass green Streptococcus, 1 case of Stenotrophomonas maltophilia, 2 cases of S. mitis, 1 case of Streptococcus pneumoniae, 1 case of Staphylococcus epidermidis, 1 case of Staphylococcus aureus, 1 case of S. mitis, and 1 case of Streptococcus agalactiae.
In the group without antibiotic treatment, there were 3 patients with a large number of Gram-positive bacteria, 7 patients with a moderate number, and 30 patients with a small number of Gram-positive bacteria or no Gram-positive bacteria. Four patients were found to have G+ bacteria, 36 patients had no G+ or G− bacteria, and 0 patients had G− bacteria. Fungal culture was negative, anaerobic culture was negative in 39 patients, and Propionibacterium acnes was detected in 1 patient. The results of common culture were as follows: 26 cases were negative; 14 cases were positive, including 1 case of oral Streptococcus, 1 case of epidermal Staphylococcus, 1 case of fecal Enterococcus, 2 cases of human Staphylococcus, 1 case of human Staphylococcus, Propionibacterium, epidermal Staphylococcus, 1 case of oral Streptococcus, 1 case of combined pharynx Streptococcus and oral Streptococcus, 1 case of infection close to Corynebacterium, 1 case of infantile Streptococcus, 1 case of Staphylococcus aureus, Streptococcus mitis, S. pneumoniae, and 1 case of bacterial deficiency.
There was no significant difference in the number of Gram-stained white blood cells between the two groups, with a χ2 of 0.904 and P = .342. There was no significant difference in Gram-stained bacteria, with a χ2 of 2.106 and P = .147. The results of the remaining bacterial cultures showed no significant differences: the chi-square test for common bacteria was 1.883, with P = .170, and the positive rate for fungi was 0, indicating no need for statistical testing. The chi-square test for anaerobic bacteria yielded a value of 1.565, with P = .211, as shown in Table 1.
Comparison of the Bacterial Culture Results Between the Two TOETVA Groups.
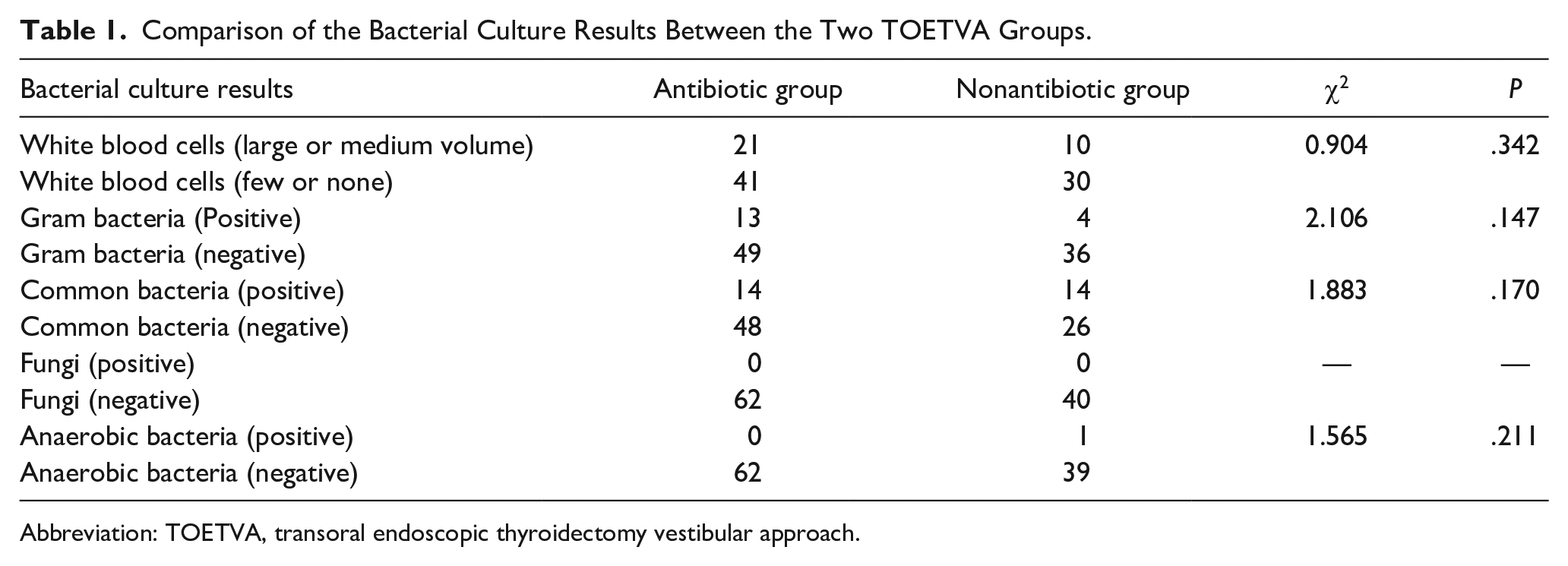
Abbreviation: TOETVA, transoral endoscopic thyroidectomy vestibular approach.
Comparison of Bacterial Culture Results between Clean and Clean-Contaminated Incisions
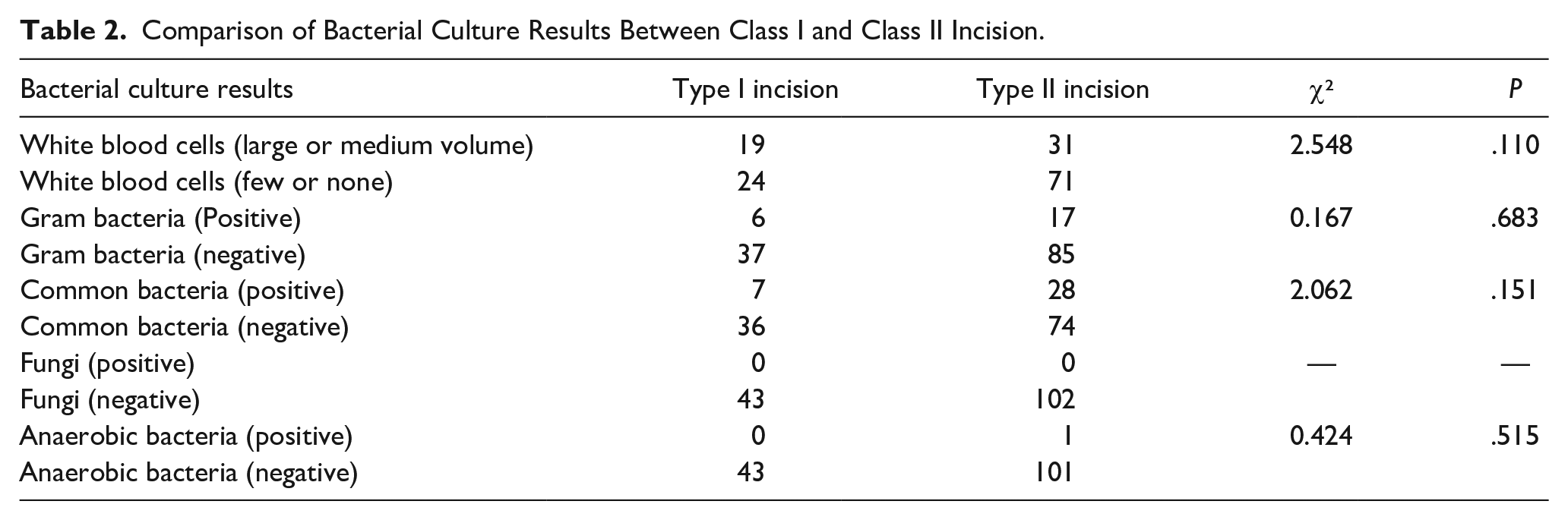
Comparison between the clean incision group and the clean-contaminated incision group revealed no significant difference in Gram-stained white blood cells, with a χ2 of 2.548 and P = .110. There was no significant difference in the bacterial culture rate between the Gram-stained bacteria comparison group II incision group and the clean incision group, with a χ2 of 0.167 and P = .683. There was no significant difference in the results of bacterial culture: common bacteria χ2 = 2.303, P = .129; the fungal positive rate was 0; no statistical test was needed; anaerobic bacteria χ2 = 0.424, P = 0.515; see Table 2.
Comparison of Bacterial Culture Results Between Class I and Class II Incision.
Discussion
Transoral endoscopic thyroidectomy is a surgery performed from the oral cavity, which contaminated with numerous bacteria, to the neck, which is considered to be a sterile area. If infection occurs, it may lead to the development of abscesses and systemic infections, as well as airway compression. This risk of infection is the main obstacle in performing transoral thyroidectomy. 10 Clinical evidence is sufficient to prove that the sublingual approach is more prone to complications such as infection, whereas the oral vestibular approach has been reported to have a lower infection rate. Therefore, surgery through the oral vestibule TOETVA is safer. 11
Surgical site infection (SSI) is another potential complication of TOETVA. It is important to avoid SSI because it can lead to additional complications and longer recovery times for patients: SSI can cause the incision site to become red, swollen, and soft and may lead to the discharge of pus or other fluids. SSI can also cause fever and chills and increase the risk of sepsis in patients. 6 Therefore, there is great interest in learning more about the factors that contribute to the development of SSIs and finding ways to prevent or reduce the risk of these infections. Recent studies on SSIs have explored several topics including the use of prophylactic antibiotics, wound dressings, and other care products, the management of blood glucose levels in diabetic patients, and the implementation of infection prevention programs during the perioperative period.12,13 Karakas et al. reported that TOETVA is a safe and effective surgical technique with a low complication rate and good cosmetic results. Their research also revealed that the use of preventive antibiotics and disinfection of the enoral mucosa before surgery may effectively reduce the risk of infection. 6
The overuse of antibiotics has caused significant harm, and doctors now realize the importance of reducing unnecessary antibiotic use. In thyroid surgery, there is a consensus that conventional clean incisions generally do not require the use of antibiotics. However, in recent years, the predominant surgical approach has changed from a clean-contaminated incision to a clean incision, with doctors still subconsciously worrying about the infection rate of this cosmetic procedure. According to classic literature and tutorials, sufficient antibiotics during the perioperative period are essential, and no increase in the infection rate has been reported after treatment. 7 However, scholars have continuously questioned the necessity of antibiotics, and even after the use of antibiotics has decreased, the infection rates have not increased. 14 One explanation may be that there may not be strong pathogenic bacteria in the oral cavity. Another explanation may be that the slight increase and decrease in white blood cells after surgery may enhance the body’s ability to fight infections, and 1 week after surgery, these elevated white blood cell levels returned to relatively normal levels.
However, further clarification is needed to determine whether the infection rate after oral thyroid surgery increases and whether it is caused by the oral microbiota entering the surgical cavity to increase the confidence of surgeons when antibiotics are removed. The results of this study revealed no significant differences in postoperative infection rates or bacterial culture results between clean and clean-contaminated incisions. There was no significant difference in the above indicators between the group that received antibiotics for clean-contaminated incisions and the group that did not use antibiotics. We obtained drainage material from the surgical cavity through postoperative drainage tubes for bacterial culture. Except for one patient with obvious tracheobronchitis complicated with pathogenic bacterial infection during the perioperative period, no obvious pathogenic bacteria were cultured and caused surgical cavity infection in other patients. In the later stage, we strictly followed the antibiotic use standards of open surgery and did not use antibiotics before or after surgery. We only administered prophylactic oral antibiotic treatment after the drainage tube was removed, and there were obvious local inflammatory reactions after discharge. All patients improved on their own, and there were no open drainage patients.
Therefore, we believe that adequate oral disinfection and physiological saline irrigation of the surgical cavity after surgical resection can effectively prevent the occurrence of pathogenic bacteria in the cavity. During the perioperative period, the vast majority of patients do not need antibiotics, and only patients with local inflammatory symptoms such as redness and swelling after drainage removal are treated with antibiotics, without affecting the overall infection rate. Notably, the findings of this study are applicable only to endoscopic thyroid surgery via the oral vestibular approach and are not applicable to surgery via the sublingual approach. The sublingual approach has a relatively high degree of trauma and as the incision is located at a low position, there may still be a risk of secretion infiltration after suturing due to inevitable damage to the oral barrier, resulting in a relatively high infection rate. 15 The currently more popular transoral vestibular surgery, owing to its incision located in a higher position of the lip mucosa, results in the formation of a closed wound after suturing, making the surgical site less vulnerable to contamination than other types of incisions in the oral cavity. If there is no obvious bacterial invasion during surgery, theoretically, it will not increase the infection rate of the surgery.
This study has certain limitations. First, the included data are from a single center and do not consider the impact of operator factors on postoperative infections. Second, this study is an observational study and not a formal randomized controlled clinical trial. The results are for reference only. In the future, in-depth randomized controlled trials should be conducted to further validate the conclusions.
Conclusion
In summary, this study explored the issue of postoperative antibiotic use in transoral vestibular endoscopic thyroid surgery and revealed that TOETVA surgery does not require the use of antibiotics unless there are special circumstances.
Footnotes
Acknowledgements
We wish to thank all the individuals who participated in this study.
Authors’ Contributions
Drafting the manuscript: Bingbing Wu, Xiao Chen, Junwei Huang. Acquisition of data: Bingbing Wu, Xiao Chen, Junwei Huang. Analysis of data: Bingbing Wu, Xiao Chen, Junwei Huang. Revising the manuscript for important intellectual content: Bingbing Wu, Xiao Chen, Junwei Huang. Conception and design of the study: Junwei Huang.
Data Availability Statement
The data that support the findings of this study are available from the corresponding author upon reasonable request.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethics Approval
All of the procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards.
Informed Consent
Informed consent was obtained from all individual participants and guardians included in the study.