
Abstract
Orbital apex syndrome (OAS) is a severe orbital condition caused by impairment of cranial nerves after inflammation or local compression. The report details an uncommon case of OAS caused by herpes zoster ophthalmicus (HZO) following endoscopic sinus surgery. A 52-year-old male exhibited symptoms of OAS in the postoperative phase; however, imaging examination and endoscopic evaluations failed to support that surgical damage and bacterial infection were the cause. The distinctive skin manifestations of herpes zoster around eye were the important clue for diagnosis. The patient was diagnosed with OAS caused by HZO and recovered after antiviral treatment for two weeks. During a one-month follow-up, the patient reported no eye-related sequelae. This case highlights the significance of early diagnosis and prompt intervention to achieve optimal clinical outcomes.
Introduction
Orbital apex syndrome (OAS) is a severe clinical syndrome caused by a variety of pathological changes in the orbital apex region. It is mainly characterized by damage of cranial nerves (CN), including optic nerve (CN II), oculomotor nerve (CN III), trochlear nerve (CN IV), abducens nerve (CN VI), and ophthalmic branch of trigeminal nerve (CN V1). 1 Infection (bacterial, fungal, and viral), trauma, vascular abnormalities including cavernous sinus thrombosis, endocrine disorders, tumor invasion, and congenital anomalies may contribute to the occurrence of OAS. These factors can lead to compression, inflammation, or ischemic damage to the neural and vascular structures in the orbital apex, causing serious clinical complications such as blindness, ocular motility disorders, and permanent neurological damage. 2 The progression of OAS is rapid, and early recognition and accurate diagnosis of OAS are critical to decrease high risk of disability.
We reported a case of OAS caused by herpes zoster ophthalmicus (HZO) after nasal endoscopic surgery. The operative regions during nasal endoscopic surgery are close to orbital structures, which lead to a potential risk of ocular complications after surgery. The onset of OAS in the reported patient was not caused by surgical injury. The subsequent occurrence of HZO with dermatological and neurological features was a vital clue for diagnosis. We emphasize the importance of recognizing HZO as a rare but significant cause of OAS, particularly in the postoperative phase, to ensure timely diagnosis and appropriate management. Prompt identification and early intervention are essential to decrease the risk of long-term complications. 1
Clinical Report
The patient, a 52-year-old male with no significant past medical history, was diagnosed with bilateral nasal inverted papilloma and underwent an extensive endoscopic sinus procedure, including tumor resection, ethmoidectomy, and open surgeries of the frontal, maxillary, and sphenoid sinuses. His nasal cavities were packed with absorbable material after surgery, with no signs of active bleeding noted in the nasal cavity and periorbital region. On the first postoperative day, the patient’s body temperature remained normal, and no evidence of periorbital congestion was observed. Vision and ocular motility were intact bilaterally. He was discharged on the fourth postoperative day without any complaints. On postoperative day 11, the patient underwent routine nasal packing removal, with the surgical cavity appearing normal. However, by postoperative day 12, the patient began to experience fatigue, along with swelling and pain localized to the right orbital region. Despite these symptoms, he did not seek medical attention at that time. By postoperative day 17, the patient’s condition had markedly deteriorated, presenting with persistent and severe right-sided headaches, facial numbness, scleral congestion, eyelid swelling, and diminished vision in the right eye, while the left eye remained unaffected (Figure 1a). Considering the clinical presentation, the patient was readmitted to the otolaryngology department with a suspected orbital infection as a complication of endoscopic sinus surgery.
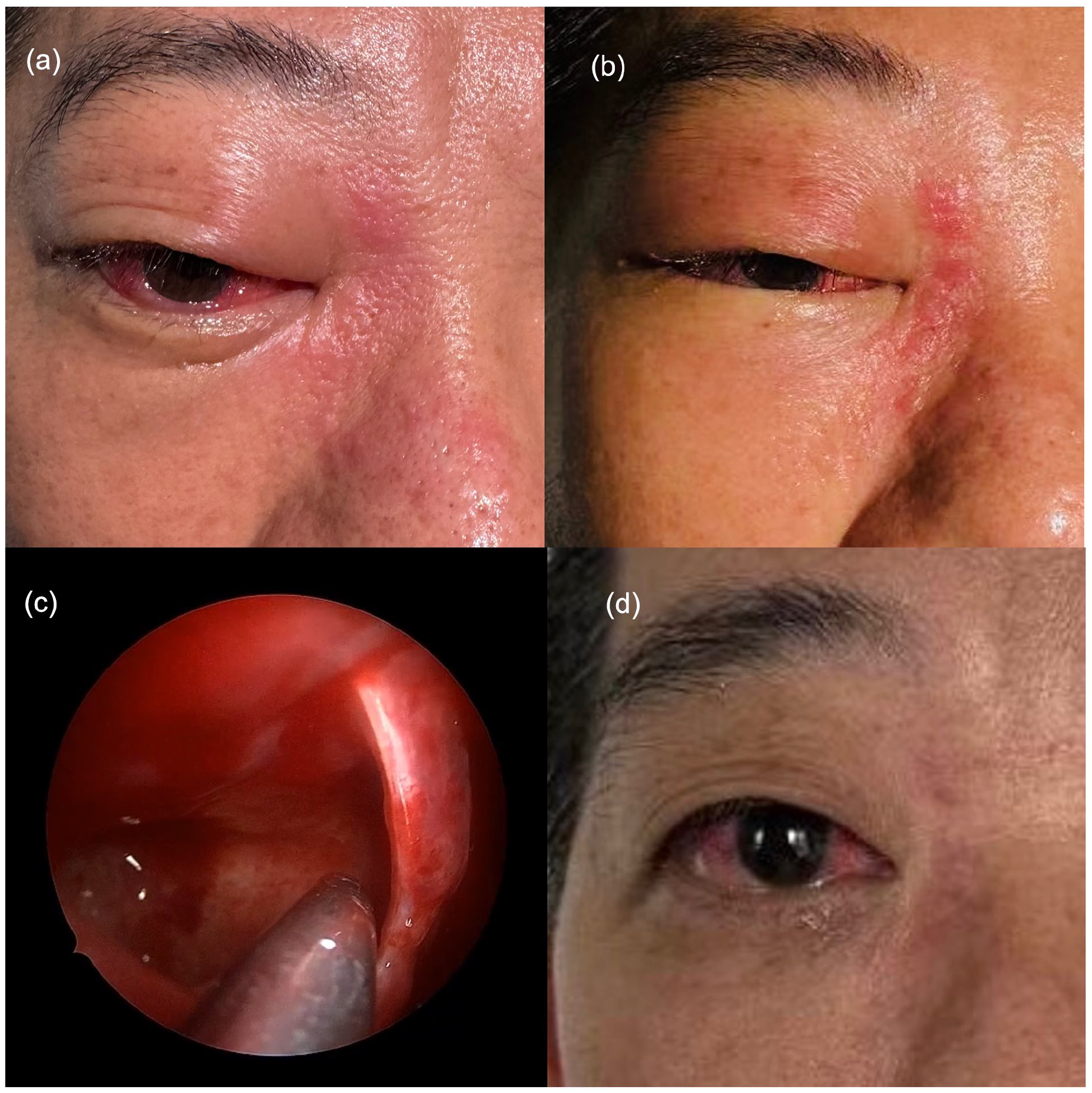
The patient had scleral congestion and mild ptosis in the right eye on admission (a). Two days after admission, ptosis was worse, and there were multiple clusters of erythema and band-like papuloherpes on the skin between nosal root and inner canthus (b); nasal endoscopy showed smooth sphenoid sinus mucosa with clear secretions and no bone destruction (c); before discharge, skin lesions and scleral congestion improved, and ptosis disappeared (d).
Upon admission, ophthalmic examination revealed considerable vision loss in the right eye, with visual acuity reduced to 0.15. Additionally, the patient presented with elevated intraocular pressure of 34 mmHg in the right eye, sluggish pupillary light reflexes, and restricted ocular motility. Following consultation with an ophthalmologist, his clinical signs were consistent with OAS, suspected to have been precipitated by ocular complications following endoscopic sinus surgery. Given the concern that the symptoms might be secondary to a postoperative orbital infection, intravenous meropenem was initiated at a dose of 2.0 g every 8 hours on the day of admission. Computed tomography (CT) imaging demonstrated that the optic nerve maintained a normal course and clear boundaries, with no abnormalities noted in the periorbital or orbital apex structures (Figure 2a and b). Contrast-enhanced magnetic resonance imaging revealed swelling of the right eyelid and maxillofacial soft tissues (Figure 2c), along with thickening of multiple right ocular muscles extending to the orbital apex region, which exhibited enhanced signals (Figure 2e). A suspicious ring-enhancing signal was observed near the orbital apex of the right optic nerve (Figure 2d). Magnetic resonance angiography of the cavernous sinus showed normal arterial anatomy, effectively excluding thrombosis as a contributing factor (Figure 2f). The imaging findings were consistent with those typically seen in orbital apex syndrome; however, they did not support ocular complications resulting from endoscopic sinus surgery. According to the patient’s report upon admission, he had not experienced fevers or chills since the onset of his illness, with his body temperature remaining below 37.1°C. Additionally, his complete blood count and C-reactive protein levels were within normal limits, findings that did not support a diagnosis of bacterial infection. Furthermore, his symptoms failed to show improvement despite treatment with intravenous antibiotics. A repeat endoscopic examination of the sinus cavity was conducted, revealing a small, nonpurulent discharge from the right sphenoid sinus. Subsequent bacterial and fungal cultures of this discharge were negative. After clearing the secretions, the mucous membrane of the lateral wall of the sphenoid sinus appeared smooth, further indicating an absence of infection following the endoscopic sinus surgery (Figure 1c). On the 19th postoperative day, physical examination revealed multiple clusters of erythematous and papular lesions on the skin between the nasal root and inner canthus, distributed in a band-like pattern (Figure 1b). Following consultations with dermatology and ophthalmology, these symptoms led to a diagnosis of HZO. Additionally, testing of the patient’s ocular secretions confirmed the presence of varicella-zoster virus DNA. We then initiated antiviral therapy, administering intravenous acyclovir and applying ganciclovir ophthalmic gel topically several times daily. Oral gabapentin was prescribed to alleviate the persistent neuropathic pain associated with herpes. Daily ophthalmic examinations were conducted to monitor changes in visual acuity and intraocular pressure throughout the course. Over the following week, the herpes lesions around the right eye gradually resolved, scleral congestion diminished, ptosis of the right upper eyelid improved, and ocular pain subsided. By the sixth day of antiviral treatment, both the visual acuity and intraocular pressure of the right eye had returned to pre-onset levels with normalized ocular motility (Figure 1d).
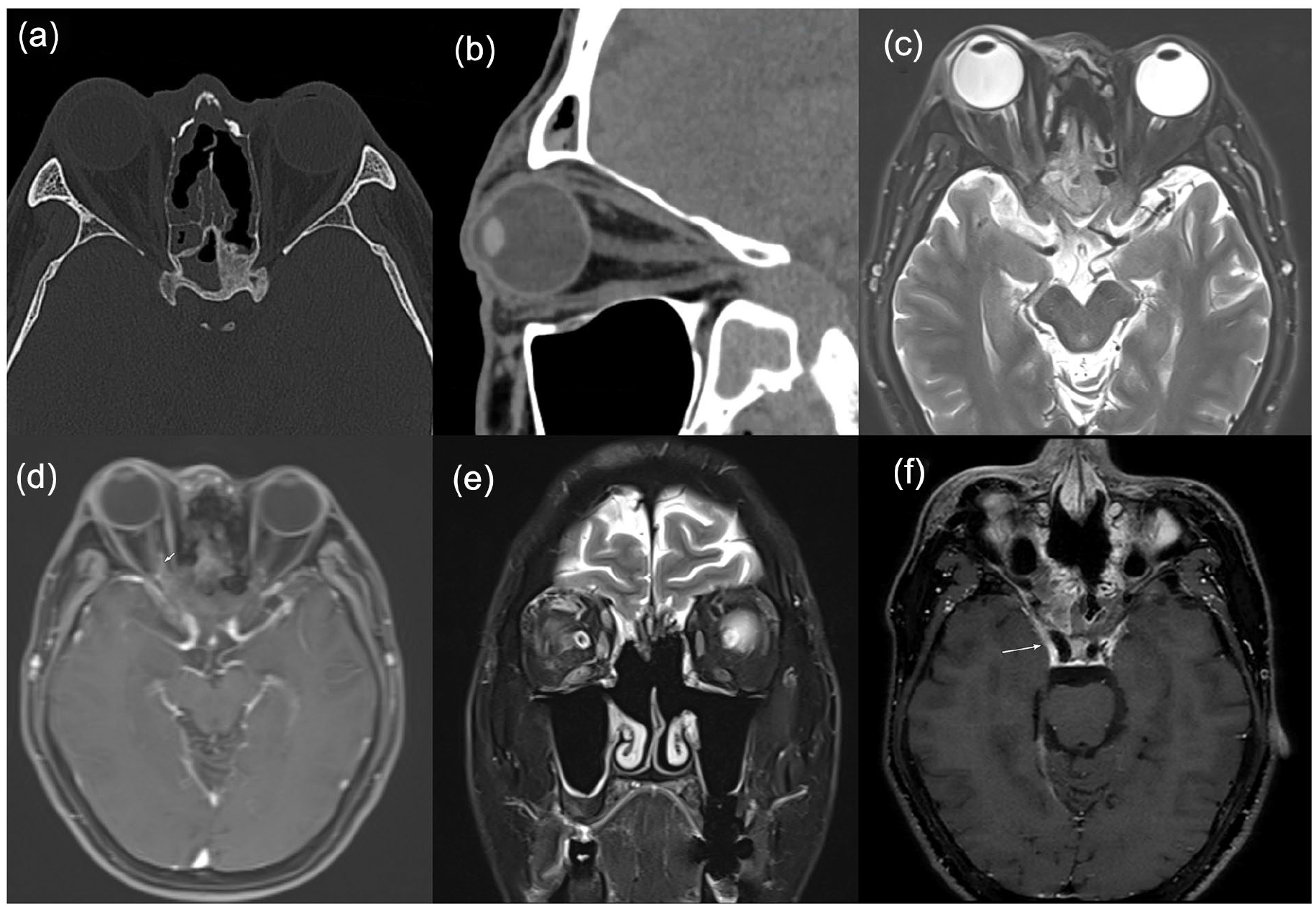
CT images showed postoperative changes in the paranasal sinuses with a normal optic nerve course, intact orbital apex, and no bone destruction.(a) Axial CT and (b) sagittal CT; the enhanced MRI scan showed right maxillofacial and eyelid swelling on T2WI (c), suspected optic nerve ring enhancement on axial contrast-enhanced T1WI (d, white arrow), extraocular muscle thickening on coronal T2WI (e), and no cavernous sinus thrombosis on MR angiography (f, white arrow). CT, computed tomography; MRI, magnetic resonance imaging; T1WI, T1-weighted image; T2WI, T2-weighted image.
Following antiviral therapy for two weeks, the symptoms associated with OAS gradually subsided. During a one-month follow-up, it was noted that his ocular lesions had resolved, with only mild postherpetic neuralgia remaining in the region of the original lesion.
Discussion
The orbital apex is a region in which many critical orbital structures converge and communicate with other important, periorbital spaces. CN II through VI, major orbital vessels, and all of the extraocular muscles excluding the inferior oblique sit in tight proximity within the apex (Figure 3). Pathology in this region can lead to significant impairments, including vision loss, ocular motility dysfunction, ptosis, and sensory disturbances, collectively defined to as OAS. 1
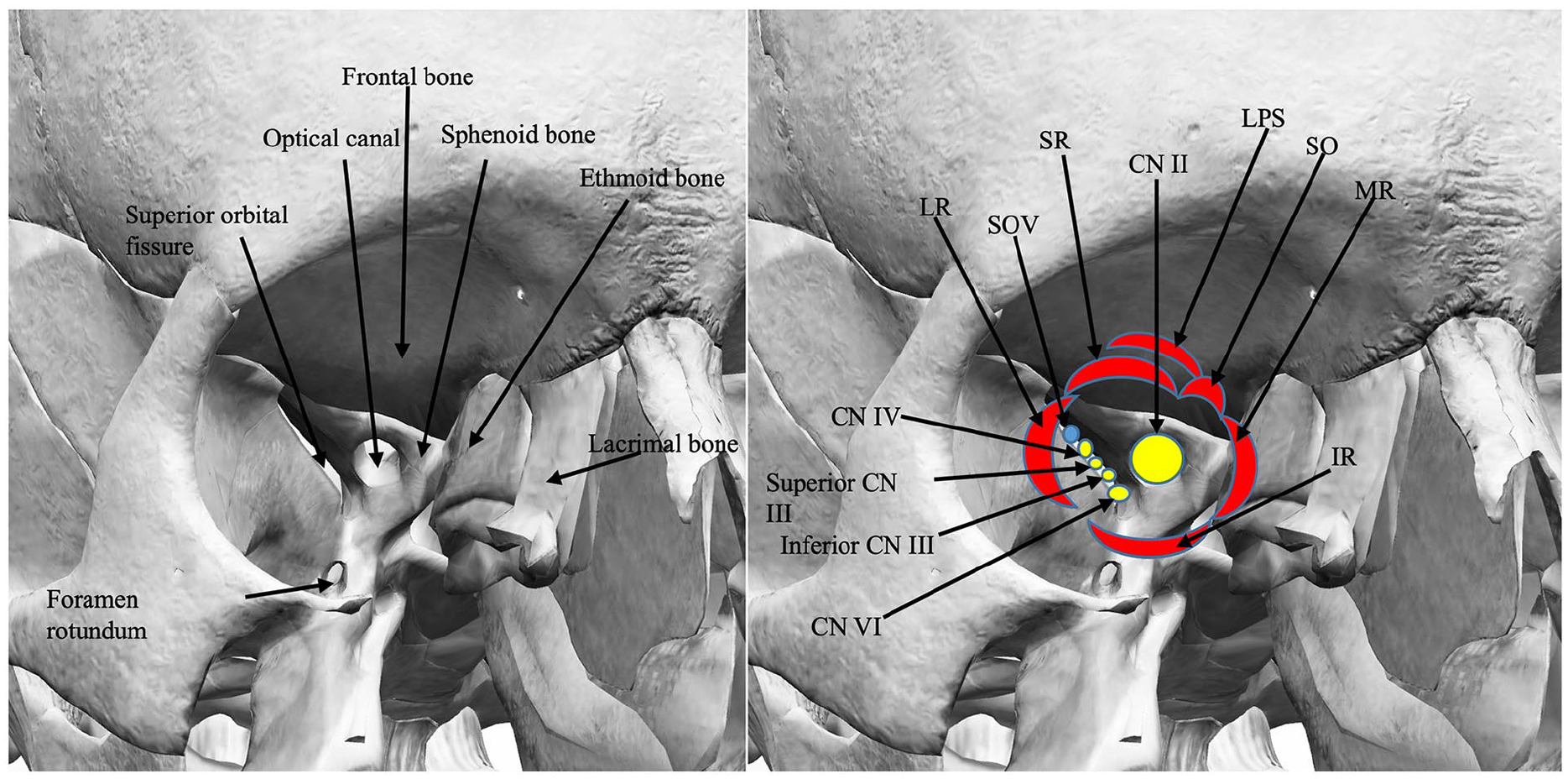
Anatomy of the right orbital apex, highlighting the extraocular muscle origins and the contents of the superior orbital fissure. LPS, levator muscle; SR, superior rectus; LR, lateral rectus; IR, inferior rectus; MR, medial rectus; SO, superior oblique; SOV, superior ophthalmic vein; CN II, optic nerve; Superior CN III, superior division of oculomotor nerve; Inferior CN III, inferior division of oculomotor nerve; CN IV, trochlear nerve; CN VI, abducens nerve.
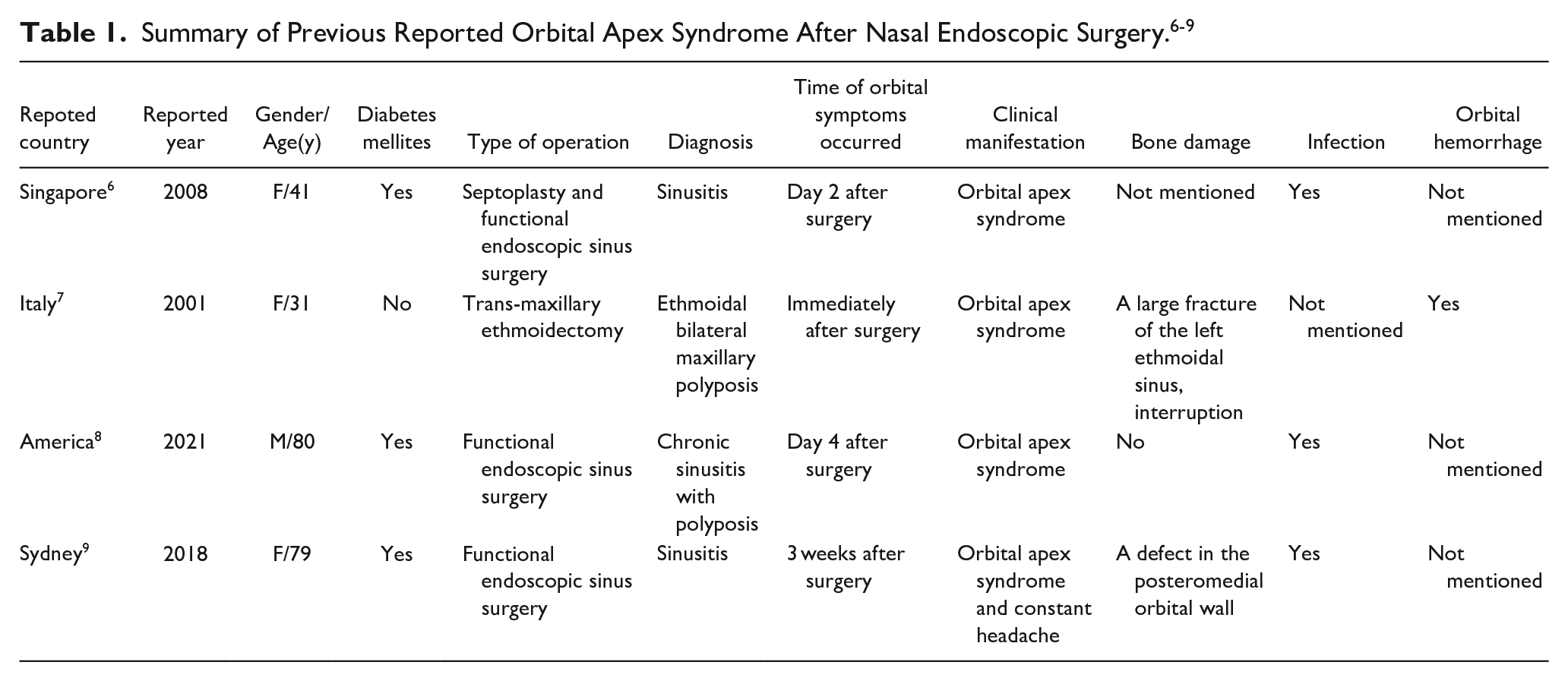
In this case, the symptoms of OAS were initially considered as potential ocular complications following nasal endoscopic surgery. Given the anatomical proximity of the nasal cavity and paranasal sinuses to the orbit, endoscopic sinus surgery can lead to direct or indirect damage to the orbital wall, CN II, extraocular muscles, blood vessels, and lacrimal passages. Improper handling during such procedures can also lead to orbital infections, which may subsequently cause severe ocular complications like orbital cellulitis or abscesses. 3 If the ocular complications extend to involve the superior orbital fissure, orbital apex, and adjacent areas, they can affect the CN III, IV, V, VI, and II. This involvement can result in OAS, characterized by restricted eye movement, ptosis, periorbital skin paresthesia, diplopia, and even blindness.4,5 However, case reports of OAS secondary to endoscopic sinus surgery are limited. After a systemic literature reviewing, we identified four related cases (Table 1).6-9 Among the reports, the causes of OAS included bone destruction in two cases (2/4), orbital hemorrhage in one case (1/4), and bacterial infection in three cases (3/4). Notably, most patients were elderly (2/4) and had underlying conditions such as diabetes mellitus (3/4), with all four cases presenting infectious sinusitis as the primary disease. This article reports a middle-aged patient in good health, with noninfectious primary diseases. Imaging examination, nasal endoscopy, and laboratory tests including pathogenic identifications were conducted to exclude bone injuries, nerve damage, and secondary bacterial infections that could have been caused by surgery. The distinctive dermatological manifestations of herpes zoster represented a crucial diagnostic clue in determining the underlying cause. In the differential diagnosis of OAS following endoscopic sinus surgery, it is imperative to acknowledge the significance of considering less frequent causes, such as viral infections.
HZO is a special manifestation of herpes zoster, which is mainly caused by reactivation of varicella-zoster virus (VZV). 10 VZV could be latent in the cranial ganglia of the dorsal root ganglion of the spinal nerve after primary infection, especially in the CN V1. Under the influence of certain predisposing factors, such as immune deficiency, advanced age, stress, and the postoperative state, the virus becomes activated and spreads along the nerve distribution areas, leading to localized inflammation and tissue damage. 11 In this reported case, the patient had undergone surgery, with the endoscopic surgical site being close to the orbital apex. While the exact mechanism of viral reactivation remains unclear, it is plausible that the surgical procedure may have contributed as a precipitating factor.12,13 The reactivation of the virus in the CN V1 may result in inflammation and damage to ocular structures. The main clinical manifestations include a characteristic rash on the forehead, eyelid and nasal root, eyelid erythema and edema, conjunctival hyperemia, increased intraocular pressure, and decreased vision. In addition, patients may experience acute neuralgia and nerve paralysis. 10
OAS secondary to HZO is a rare yet serious condition that can lead to visual loss, severe neurological dysfunction, and prolonged neuralgia. The potential mechanisms by which HZO may cause OAS include viral spread along the nerve to the orbital apex and surrounding tissues, an inflammatory response reaching the orbital apex region which triggered by the VZV, and the development of small-vessel occlusive vasculitis within the orbital apex area due to the viral infection. These processes can subsequently lead to damage of nerves and tissues.14,15 According to previous reports, OAS caused by HZO is easy to be misdiagnosed or missed due to its complex and diverse clinical manifestations and lack of specificity in the early phase. In some cases, the onset of ocular rash may be delayed, further complicating the diagnosis. 14 Therefore, the rare but potential cause such as HZO should be considered in the differential diagnosis of OAS.
Conclusion
It is the first case report of OAS secondary to HZO after endoscopic sinus surgery. When OAS occurs after nasal endoscopic surgery, and surgical trauma and postoperative secondary bacterial infection are excluded via imaging examination and endoscopic examination. HZO, a rare but potential cause, should be considered to reduce the risk of misdiagnosis and missed diagnosis. Early identification and active antiviral treatment are essential to prevent severe complications such as visual impairment and nerve paralysis.
Footnotes
Acknowledgements
None.
Author Contributions
Chen Peng: Writing—original draft, Date collection and Visualization; Zhimin Xing: Writing—review & editing, Validation; Yan Liu: Writing—review & editing; Congli Geng and Yidi Liu: Picture collection; All authors read and approved the final article.
Data Availability Statement
All data and materials generated or used during the study were included in the submitted article.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethics Approval
Ethical approval to report this case was obtained from the Ethics Review Committee of Peking University People’s Hospital.
Consent for Publication
Authors have obtained written informed consent from the patient for the publication of this case report.