
Abstract
Auricular mucormycosis is an exceptionally rare and aggressive fungal infection primarily affecting immunocompromised individuals, particularly those with poorly controlled diabetes. This report presents the case of a 54-year-old diabetic woman with isolated auricular mucormycosis and facial nerve palsy. The patient developed right auricular edema, necrosis, and severe pain, progressing over 10 days, with no history of trauma. Initial management included broad-spectrum antibiotics and intravenous liposomal amphotericin B, followed by surgical debridement and partial auricular resection. Despite extensive soft tissue involvement, imaging revealed no bony erosion or significant compression of the facial nerve. Facial nerve function gradually improved from House-Brackmann grade IV to grade II within 38 days. The patient’s condition stabilized after sequential surgical interventions and prolonged antifungal therapy, culminating in recovery by day 61. A comprehensive literature review identified 6 documented cases of auricular mucormycosis, all involving diabetic patients, with a mortality rate of 33.3%. Facial nerve paralysis, observed in 4 cases, often persisted despite infection resolution. This case underscores the importance of early diagnosis, aggressive antifungal therapy, surgical debridement, and meticulous management of underlying conditions to optimize outcomes in auricular mucormycosis, a condition with significant diagnostic and therapeutic challenges.
Introduction
Mucormycosis is a rare but aggressive fungal infection predominantly affecting individuals with poorly controlled diabetes mellitus and those who are severely immunocompromised, such as patients with hematological malignancies and solid organ transplant recipients. This disease is caused by various fungi classified as mucormycetes, with the genera Rhizopus, Mucor, and Rhizomucor being the most prevalent in human infections. 1 Notably, Rhizopus species possess the enzyme ketone reductase, enabling them to thrive in high-glucose, acidic environments. 2 The angioinvasive nature of these fungi leads to tissue infarction, a hallmark of the disease. Clinical manifestations vary based on the infected site, with rhino-orbital-cerebral and pulmonary infections being the most common, followed by cutaneous, gastrointestinal, and disseminated forms. Mucormycosis is characterized by infarction and necrosis of host tissues resulting from vascular invasion by hyphae, typically progressing rapidly, although indolent cases have been reported. Cutaneous mucormycosis often arises from traumatic inoculation of spores into the dermis, with common entry points including intravenous catheter sites, spider bites, and insulin injection sites. 1 It usually presents as a painful, indurated cellulitis that can rapidly evolve into tissue necrosis due to ischemic infarction. Mucormycosis of the external and middle ear is a rare entity. A review of the literature found very few cases of mucormycosis of the external ear extended to the temporal bone.1,2 Here we report a rare case of isolated auricular mucormycosis with facial nerve palsy without local trauma or injury with a comprehensive literature review.
Case Presentation
A 54-year-old woman 60 kg presented to the ENT clinic with right auricular edema and erythema that had gradually developed during the last 10 days with severe pain, bloody and purulent oozing, and necrosis, which indicated admission to the hospital. Clinical examination showed external auditory canal edema, dark necrosis, and posterior auricular groove effacement (Figure 1). Medical history involved 20-year of diabetes, 15 years of hypertension, and 1 year of anemia due to poor nutrition. In addition, a history of smoking for 30 years was noted. Labs showed elevated white blood cells = 13.2 and C-reactive protein = 361.45. Meropenem 1 g q12 hours has been initiated immediately to control the spread of the infection. On day 13, an ellipse of skin 12*21 mm with focal necrotic lesion submitted for microscopic examination revealed angioinvasive mucormycosis obligating intravenous amphotresine B liposomal (lower concentration 0.2 mg/ml) to be administered. A first superficial debridement to the necrotic tissues on day 15 followed by resection of a part of the upper auricle on day 19 to eradicate the disease (Figure 1). A grade IV House-Brackmann facial nerve paresis has been assigned on day 21. Computed tomography without contrast shows the absence of the skin and cartilage of the right upper auricle with edema extending into the cartilage portion of the external auditory canal and the right stylomastoid foramen. No bone erosion and no marked compression to the facial nerve are seen (Figure 2). On day 25, the culture of pus revealed pseudomonas that had been sensitive to colistine only, so the bacterial antibiotic was adjusted. Sequential debridements of the fibrous tissue occurred. The facial nerve followed a slow insidious course of recovery to reach a grade II by day 38. Labs improved gradually toward normal ranges. By day 46, all antibiotics were omitted except for intravenous amphotresine B liposomal which was adjusted to (0.3 mg/ml) until the wound healed from infection by day 61 and the patient was discharged.
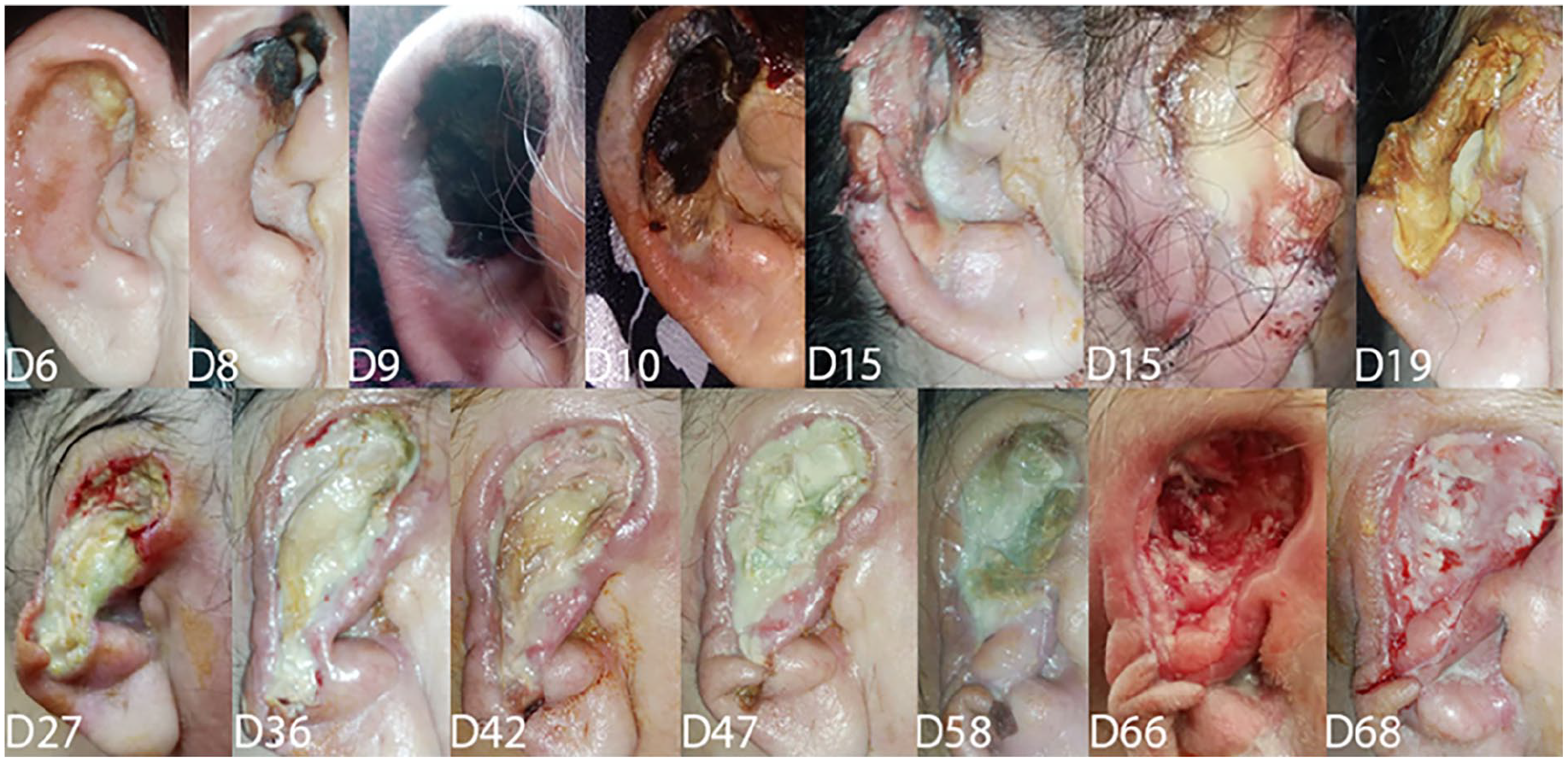
Clinical course of the disease.
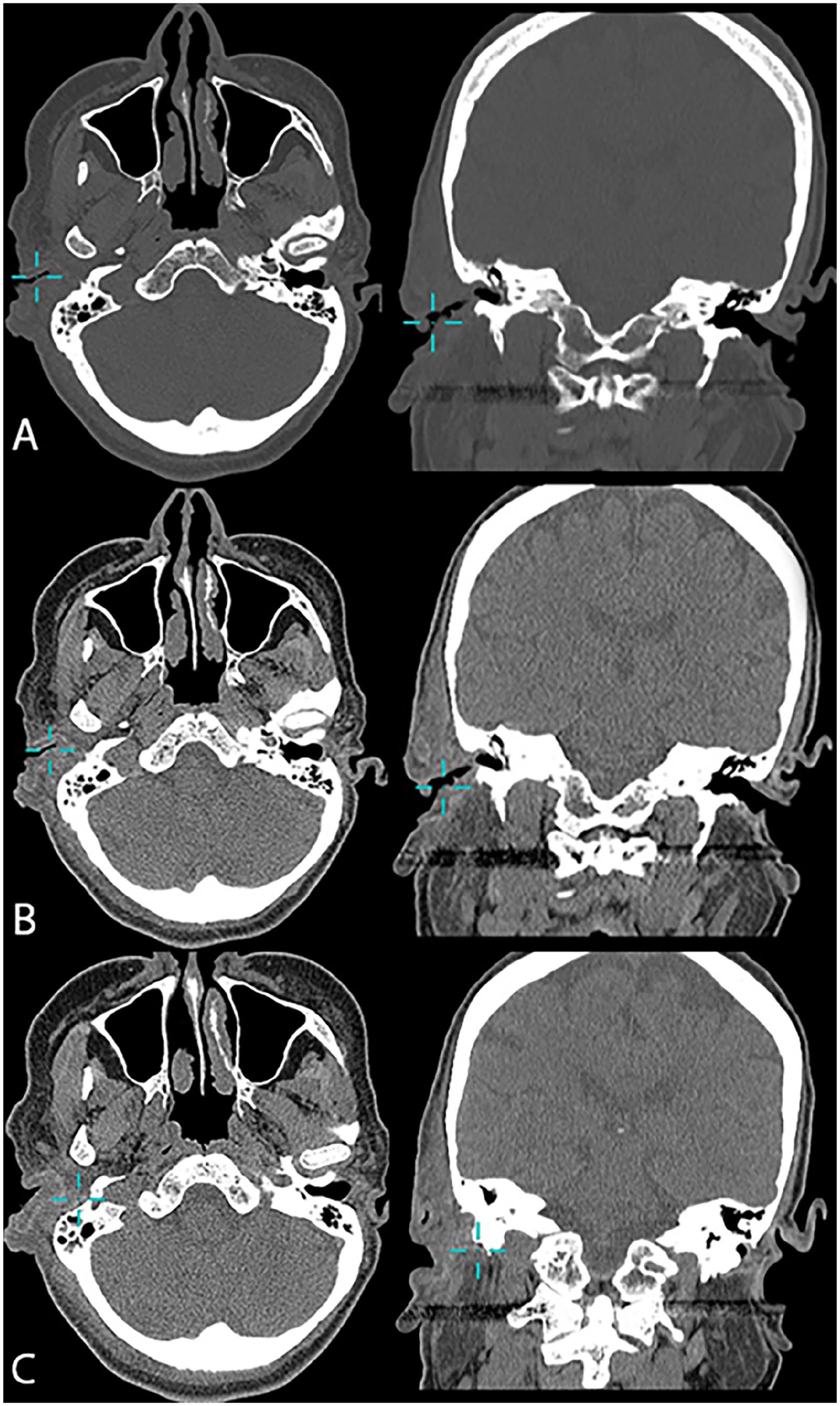
Computed tomography without contrast to the head, axial, and coronal planes shows (A) bone view, (B) and (C) soft tissue views tracing the extension of the edema toward the stylomastoid foramen.
Discussion
Mucormycosis is an uncommon fungal infection caused by filamentous fungi from the class Zycomycetes, specifically within the order Mucorales. In individuals with a healthy immune system, these fungi typically exhibit low pathogenicity. 3 However, they can become highly infectious in immunocompromised individuals, including those with diabetes, acidosis, immune deficiencies accompanied by neutropenia, severe malnutrition, or those undergoing corticosteroid or cytotoxic treatments. The rhino-orbito-cerebral form of the infection is the most commonly observed, accounting for approximately 40% of cases.3,4 Mucormycosis can also manifest in other anatomical regions, including the skin, lungs, gastrointestinal tract, and more widespread or unusual forms. When it affects the otologic region, several mechanisms have been proposed: fungal spores may travel from the sinonasal cavities to the middle ear via the Eustachian tube, they may enter through a perforated tympanic membrane, or they may directly invade the ear and mastoid through auricular mucormycosis.4,5 The management of auricular mucormycosis typically involves a multimodal approach, combining high-dose antifungal therapy (such as amphotericin B at 5-15 mg/kg/day), surgical debridement, and careful management of any underlying comorbid conditions. Surgical removal of necrotic tissue is essential, as it helps to reduce the fungal burden and enhances the efficacy of antifungal agents by improving their ability to penetrate the affected tissues. Given the infrequency of such cases, there is no established protocol regarding the optimal duration of antifungal treatment for auricular mucormycosis.6,7
Our literature review revealed 6 cases of auricular mucormycosis documented in the literature, including the case presented in this report. There were 4 females and 2 males, with 5 adults having an average age of 45.6 years, and 1 case in a child aged 1.5 years. All 6 cases had underlying immunocompromising conditions, primarily diabetes, which was present in all 6 cases. Auricular mucormycosis was complicated by facial nerve paralysis in 4 out of the 6 cases. In three of these, facial nerve paralysis persisted despite the resolution of the infection, while in the fourth case, the patient died on the seventh day of treatment. All cases were treated with intravenous amphotericin B and surgical debridement. As for the outcome, 4 cases fully recovered, while 2 patients died, representing a 33.3% mortality rate. One patient died on the second day of treatment, and the other on the seventh day. Although cutaneous mucormycosis is well recognized, its occurrence in the auricular site has not been widely acknowledged until recently. We observe that all recorded cases of auricular mucormycosis have been documented after the year 2000, which may correspond to the increasing incidence of mucormycosis in general, linked to the rise of immunocompromising diseases, primarily diabetes. Alternatively, this may be due to previous diagnostic and documentation limitations. We note that all the cases had chronic, exacerbated conditions, primarily diabetes, which aligns with the fact that mucormycosis is generally an opportunistic infection in immunocompromised individuals, particularly in diabetic patients. In addition to its known immunosuppressive effects, diabetes also impacts blood vessels, especially microvessels, which may predispose individuals to mucormycosis and vascular invasion. Facial nerve involvement in auricular mucormycosis has a poor prognosis, as the paralysis was persistent in all cases. Two patients died out of the 6, with a mortality rate of 33.33%. One of the deceased had multiple chronic, exacerbated conditions, and the other had diabetes complicated by ketoacidosis. This suggests that the patient’s poor overall condition and the presence of underlying, worsening chronic diseases are associated with a poor prognosis. This highlights the importance of improving the patient’s general condition and managing immunocompromised states in treatment, which is consistent with the general approach to successfully treating mucormycosis. Table 1 presents a summary of all cases of auricular mucormycosis documented in the literature.
Summary of All Cases of Auricular Mucormycosis Reported in the Literature.
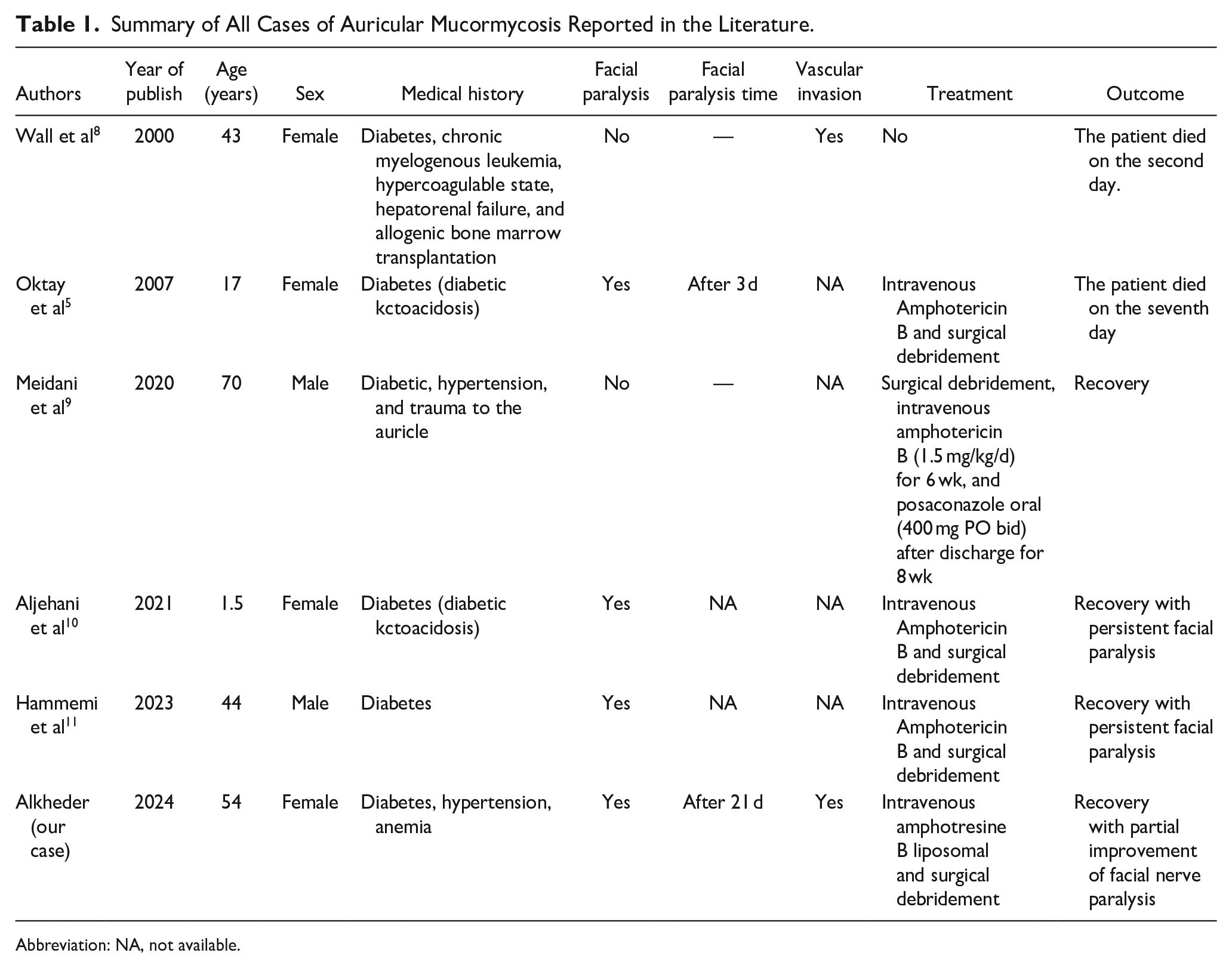
Abbreviation: NA, not available.
Mucormycosis is a severe fungal infection caused by molds belonging to the Mucor and Rhizopus genera. These fungi thrive in environments with decaying organic matter and often infect individuals with impaired immune systems. Auricular mucormycosis, while less common than cutaneous or rhino-orbital types, has been increasingly documented since the year 2000. The growing recognition of auricular mucormycosis parallels the general rise in mucormycosis cases due to the increase in diabetes and other immunocompromising conditions. The age range is noteworthy, with 5 adults and 1 child. The average age of the adult patients (45.6 years) is consistent with the age group that most frequently suffers from immunocompromising conditions like diabetes. The case of the 1.5-year-old child stands out as a rare and unique presentation of auricular mucormycosis, highlighting the potential vulnerability of younger immunocompromised individuals to this severe infection. One of the most significant findings of our literature review is that all 6 patients had underlying immunocompromising conditions, with diabetes being present in all cases. Diabetes, particularly when poorly controlled, creates a favorable environment for opportunistic infections like mucormycosis. The high glucose levels in the blood impair neutrophil function, thereby compromising the body’s defense mechanisms against fungal infections. Furthermore, diabetes leads to vascular changes, including microangiopathy, which may hinder effective tissue perfusion, impairing the ability to clear the infection and contributing to the invasion of blood vessels by the fungus. This correlation between diabetes and mucormycosis underscores the need for clinicians to remain vigilant when managing diabetic patients, particularly those with chronic or uncontrolled hyperglycemia. Although Mucor species can infect healthy individuals, the risk is disproportionately higher in immunocompromised patients, and diabetes serves as a significant risk factor in this regard. Facial nerve paralysis, which occurred in 4 out of the 6 cases, is a critical aspect of the clinical course of auricular mucormycosis. The involvement of the facial nerve is concerning because it is often associated with poor outcomes. In our literature review, it is noted that in 3 of the 4 cases with facial nerve involvement, paralysis persisted even after the infection resolved. This suggests that mucormycosis may cause significant, long-term damage to the facial nerve, possibly due to direct invasion of the nerve by the fungal elements or due to ischemic damage secondary to vascular invasion by the fungus. All patients in the reviewed cases were treated with intravenous amphotericin B, the first-line antifungal therapy for mucormycosis, and surgical debridement. Amphotericin B works by binding to ergosterol in the fungal cell membrane, creating pores that lead to fungal cell death. This treatment approach is standard for mucormycosis, given the aggressive nature of the infection and the difficulty in treating it with oral antifungals. However, it is important to note that the clinical response to amphotericin B can vary, and it can be associated with significant nephrotoxicity, which requires close monitoring during treatment. Surgical debridement is equally critical as it helps remove necrotic tissue and improves the efficacy of antifungal therapy. The mortality rate observed in our review is 33.3%, with 2 out of 6 patients dying during the course of their treatment. One patient died on the second day, and another on the seventh day of treatment. These outcomes are alarming and highlight the severity of auricular mucormycosis, particularly when compounded by comorbidities such as diabetes and diabetic ketoacidosis. The rapid progression of the disease in these patients further emphasizes the need for early diagnosis and prompt initiation of antifungal therapy. The mortality rate is consistent with broader trends in mucormycosis, where the overall mortality rate remains high, especially when the infection involves vital structures like the face and the central nervous system. The poor prognosis in these cases could be related to the late stage at which the infection was diagnosed or the overwhelming nature of the fungal invasion, which can lead to irreversible tissue damage and systemic infection. The presence of underlying chronic conditions, particularly diabetes, played a crucial role in determining the outcomes of the cases. Two of the patients who died had exacerbated, chronic conditions, including one who had diabetes complicated by ketoacidosis. This suggests that patients with poorly controlled diabetes or other immunocompromising conditions are more likely to experience rapid disease progression and poor outcomes, as their compromised immune systems cannot mount an effective response to the infection. The role of diabetes in mucormycosis is well documented, and it serves as a reminder of the importance of optimizing glycemic control in at-risk patients. Moreover, the case where 1 patient died of diabetic ketoacidosis suggests that hyperglycemic crises may predispose patients to more severe fungal infections, thus highlighting the critical need for managing both the infection and the underlying metabolic disorder simultaneously. The findings of this review reinforce the importance of early detection and aggressive management in cases of auricular mucormycosis. Clinicians should be aware of the risk of mucormycosis in diabetic patients with ear-related symptoms, particularly those who present with facial nerve paralysis. The rapid initiation of systemic antifungal therapy with amphotericin B, combined with timely surgical intervention, is essential for improving outcomes. Moreover, optimizing the patient’s general health and managing underlying immunocompromising conditions, especially diabetes, are crucial in improving survival rates and functional outcomes.
Conclusion
This case highlights the rarity and severity of auricular mucormycosis, a condition that poses significant diagnostic and therapeutic challenges due to its aggressive course and association with immunocompromised states, particularly diabetes. The patient’s successful recovery underscores the importance of a multidisciplinary approach involving early diagnosis, prompt initiation of systemic antifungal therapy, and meticulous surgical debridement. However, the case also emphasizes the potential for long-term complications, such as facial nerve paralysis, which may persist despite effective treatment of the infection. Given the high mortality rate and the devastating consequences of delayed intervention, clinicians should maintain a high index of suspicion for mucormycosis in diabetic patients presenting with rapidly progressive ear infections, especially when accompanied by necrosis or cranial nerve involvement. This report further reinforces the critical need for optimizing glycemic control and addressing other underlying immunosuppressive factors to improve outcomes in such cases.
Footnotes
Data Availability Statement
The data that support the findings of this study are available from the author or corresponding author upon reasonable request.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval
Our institution does not require ethical approval for reporting individual cases. Written informed consent was obtained from the patient for publication of this article.