
Abstract
Keywords
Introduction
Oral submucous fibrosis (OSMF) is a chronic, debilitating condition characterized by progressive fibrosis of the oral mucosa and submucosal tissues, often associated with the habitual use of areca nut and other irritants. This condition poses not only aesthetic and functional challenges but can also lead to significant health complications, including hearing impairment. The relationship between OSMF and auditory function has garnered increasing attention in recent years, given that the oral cavity and the ear share anatomical and physiological connections. Specifically, the Eustachian tube, which links the middle ear to the nasopharynx, plays a crucial role in maintaining middle ear pressure and is affected by conditions involving surrounding structures, such as OSMF.1,2 The extent of hearing impairment in patients with OSMF can vary widely and has been shown to correlate with the severity of the disease. Studies have indicated that changes in the structure and function of the Eustachian tube due to fibrosis may lead to Eustachian tube dysfunction (ETD), causing a chain reaction that affects middle ear function and results in auditory deficits.3-5 Understanding the mechanisms underlying these auditory changes is vital for clinicians to provide comprehensive care for OSMF patients, who may suffer from both oral and auditory complications.
Hearing Impairment in OSMF
The degree of OSMF and its possible effects on Eustachian tube function are the main factors influencing the multifactorial nature of hearing impairment in these patients. Numerous studies have been conducted on the relationship between OSMF and auditory deficiencies, and the results show a complex interaction between the disease’s course and hearing efficiency. Studies have demonstrated that individuals frequently have a reduction in hearing efficiency as OSMF advances through different clinical grades. The clinical grading of OSMF and hearing impairment levels were found to be significantly correlated in a study by Shah and Lunagariya, 1 highlighting the importance of early diagnosis and treatment of both disorders. Similarly, individuals with more advanced stages of OSMF showed more noticeable hearing impairments, as noted by Srivastava et al, 6 indicating a direct correlation between the degree of oral fibrosis and auditory function. These results highlight the need for routine evaluations of the patient’s hearing in individuals with OSMF, since prompt management could prevent additional loss of hearing.
Impact of ETD
The pathological modifications to the oral cavity and its surrounding tissues cause changes to the structural integrity and functionality of the Eustachian tube, which can cause ETD. The Eustachian tube is essential for maintaining the proper balance of air pressure in the middle ear, and its blockage or malfunction can have a domino effect on the health of the auditory system. Research has indicated that alterations in the soft tissue encircling the Eustachian tube may result in compromised middle ear ventilation and drainage, hence generating an environment with negative pressure. This malfunction has the potential to impede auditory transduction, which in turn can result in conductive hearing loss (CHL). This connection was further clarified by Devi et al, who discovered a significant prevalence of hearing impairments in OSMF patients and connected these impairments to the clinical and histological severity of the illness. 3 Rathod et al found trace element levels in OSMF patients and linked these to hearing loss, which complicated the picture of what influences auditory deficiencies in this group. 4 Based on available data, the best patient therapy may need a multidisciplinary strategy that addresses both the oral and auditory elements of OSMF.
Audiological Assessment and Management Strategies
Comprehensive audiological examinations are necessary to identify hearing impairment in patients with OSMF. Regular audiometric examinations, such as tympanometry and pure-tone audiometry (PTA), are crucial for identifying the presence and severity of hearing loss and for assisting medical practitioners in developing customized treatment regimens. Swain and Das underlined the significance of these evaluations, emphasizing that prompt treatments to enhance auditory outcomes might be made possible by early detection of hearing impairment. 7 Treatment plans for individuals with hearing loss caused by OSMF may involve medications like steroids or nasal decongestants that try to treat ETD. To improve hearing and restore middle ear function in more severe cases, surgical treatments such as myringotomy or tympanostomy tube installation may be necessary. Incorporating ENT doctors into the care of patients with OSMF can offer important insights into the challenges associated with managing both oral and auditory problems.
ETD and Its Effects on Hearing
Numerous research that has investigated the relationship between oral and auditory health have shown that ETD is a common side effect of OSMF. A disruption in the Eustachian tube’s function can result in a variety of auditory difficulties, such as pain, a fullness sensation, and reduced hearing. The Eustachian tube is an essential channel for equalizing air pressure in the middle ear. Siddiqui et al’s research found that people with OSMF often had undetected ETD, which emphasizes the importance of careful audiometric evaluations in this patient population. 8 Additionally, a variety of ETD symptoms, such as pressure in the ears and ear pain, are frequently reported by patients with OSMF, which can adversely affect their quality of life, quite significantly. Chandran and Aswath’s tympanometric studies provide additional evidence that patients with OSMF frequently have altered tympanometric patterns, which are suggestive of middle ear dysfunction. 5 These results highlight how crucial it is to take auditory impairment into account while managing OSMF overall because doing so can enhance patient outcomes.
Implications of ETD in OSMF
The relationship between Eustachian tube function and OSMF can have significant effects on how patients are managed. According to Rathod et al, patients with OSMF may experience chronic middle ear issues because of reduced Eustachian tube function. This means that treating OSMF requires a multidisciplinary strategy that considers both the oral condition and its systemic implications. 4 To guarantee that patients receive comprehensive care, this comprehensive management method may involve coordination between audiologists, otolaryngologists, and oral health specialists. It is possible that underlying inflammatory processes that impact the Eustachian tube and oral cavity are related to the link between OSMF and ETD. The localized inflammation caused by the fibrosis characteristic of OSMF may exacerbate the symptoms of ETD. By allowing doctors to customize interventions to address oral and auditory difficulties, these processes can eventually improve patient outcomes.
Auditory Impairment in OSMF: Pathophysiology and Management
Finding and treating hearing deficits in individuals with OSMF requires routine auditory evaluations, particularly considering the high incidence of ETD linked to the illness. By enabling the early identification of auditory deficiencies, instruments such as tympanometry and PTA enable focused treatments such as nasal decongestants, balloon dilatation of the Eustachian tube, or other treatments meant to restore normal auditory tube function.3,5 When the underlying pathophysiology of OSMF is examined, it becomes clear how fibrotic alterations in the oral mucosa might impact nearby structures, such as the tissues and muscles that support the Eustachian tube. ETD and hearing impairment could result from this disturbance. Neurovascular variables, vascular alterations, and inflammatory pathways may intensify this dysfunction and lead to CHL.1,2 Patients with OSMF may experience additional complications with their auditory health due to secondary processes, such as infections or autoimmune reactions. 4 Raising patient awareness about the auditory complications of OSMF can result in earlier diagnosis and intervention, ultimately improving their quality of life. The complicated effects of OSMF on auditory health must be managed with regular audiometric examinations and patient education. 7
The purpose of this systematic review was to examine the relationship between auditory dysfunction and OSMF, with a particular emphasis on ETD and hearing loss in OSMF patients. Examining the pathophysiological pathways is the goal, along with the effects of inflammation, fibrotic changes. The study assessed the effectiveness of diagnostic instruments like tympanometry and PTA in early identification of hearing impairment. It also investigated potential therapies for auditory impairments, such as nasal decongestants and balloon dilatation of the Eustachian tube. The objective of the study was to enhance awareness, early diagnosis, and management of auditory problems in OSMF patients and secondary variables such as infections and vascular abnormalities.
Methodology
Research Question
The primary research question guiding this systematic review was: “Is there a significant association between hearing impairment and OSMF, and what are the potential mechanisms behind this association?”
Time Frame of the Study
2015 to 2024 (10 years).
PICOS Framework
Population (P): Patients diagnosed with OSMF, which can potentially extend to structures related to hearing.
Intervention (I): The core investigation centered on hearing impairment, including the assessment of changes in hearing efficiency, the functionality of the Eustachian tube, and any alterations in middle ear function.
Comparison (C): A comparison was made between different groups, including patients without OSMF and those with varying grades of the condition.
Outcomes (O): The primary outcomes studied were the presence and degree of hearing loss, abnormalities in middle ear function, and dysfunction of the Eustachian tube.
Study Design (S): The review included a variety of study designs such as clinical studies, cross-sectional analyses, and case–control studies.
Search Strategy
Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) criteria were followed in this systematic review to guarantee an exhaustive and open procedure. A comprehensive search plan was created to find pertinent material across a range of databases, including Google Scholar, PubMed, Embase, Scopus, Web of Science, and the Cochrane Library. To find clinical trials and gray literature, other specialist databases were examined, including ClinicalTrials.gov and MedlinePlus. Free-text keywords and Medical Subject Headings (MeSH) terms were used to do the search. By using the Boolean operators AND, OR, and NOT to narrow down the search, studies about hearing impairment and OSMF may be found. The search phrases and keywords used comprised “oral submucous fibrosis,” “hearing loss,” “hearing impairment,” “Eustachian tube dysfunction,” “middle ear function,” “tympanometry,” “auditory efficiency,” “trace elements in OSMF,” “hearing evaluation in OSMF,” “conductive hearing loss,” “fibrosis-related hearing deficits,” “audiological assessment,” “otological manifestations in OSMF,” “nasopharyngeal involvement in OSMF,” along with “ETD in fibrotic conditions.” Boolean operators were used to combine terms in the following ways to ensure comprehensive coverage: (“trace elements” OR “fibrosis”); (“Eustachian tube dysfunction” OR “ETD”) AND (“middle ear function” OR “auditory efficiency”); (“oral submucous fibrosis” OR “OSMF”) AND (“hearing loss” OR “hearing impairment”). The databases were searched for articles published between 2000 and 2024. Filters were applied to include studies in English and those involving human subjects. Additionally, the reference lists of all the included articles were screened manually to identify any further studies that may be relevant, ensuring a thorough capture of the literature.
Selection Criteria
Studies involving human subjects diagnosed with OSMF, including clinical studies, case–control studies, and observational studies that specifically measured middle ear function, Eustachian tube function, or hearing efficiency in OSMF patients, met the inclusion criteria for this systematic review. Only research that was published between 2015 and 2024 in peer-reviewed publications was considered. For inclusion in the review, studies were required to be published in English. Moreover, only investigations involving adult populations aged 18 years and older were included to ensure demographic homogeneity. Additionally, studies were required to classify the severity of OSMF using standardized grading systems, such as the Khanna and Andrade classification, 9 to facilitate consistent comparisons across findings. Studies using animal models, case reports, editorials, and letters to the editor were all excluded because they lacked the strong evidence required for a systematic review. Research without unambiguous evaluations of hearing impairment or quantifiable results pertaining to auditory function were likewise disregarded. Moreover, articles written in languages other than English were excluded from consideration for inclusion.
Data Extraction, Synthesis, and Quality Assessment
From a total of 1137 screened articles, 18 met the inclusion criteria for this review (Figure 1). Data extraction was independently performed by 4 reviewers (C.K., A.D., K.K., A.B.), focusing on study characteristics, population demographics, hearing evaluation methods, and outcomes related to hearing impairment in OSMF patients. Discrepancies were resolved through discussion or consultation with a fourth reviewer. Both narrative and quantitative approaches were employed to synthesize findings. Quality assessment utilized the Cochrane Risk of Bias Tool for randomized controlled trials and the Newcastle–Ottawa Scale (NOS) for non-randomized studies, grading studies based on selection criteria, comparability, and outcome metrics. A detailed table documented individual NOS scores, emphasizing adjustments for confounding factors such as age, gender, and lifestyle habits (eg, smoking, alcohol use). Studies with lower comparability scores due to insufficient control of confounders were flagged and their implications discussed. K.K. handled quality assessment and dispute resolution, C.K. led data synthesis, and A.D. and A.B. ensured data accuracy.
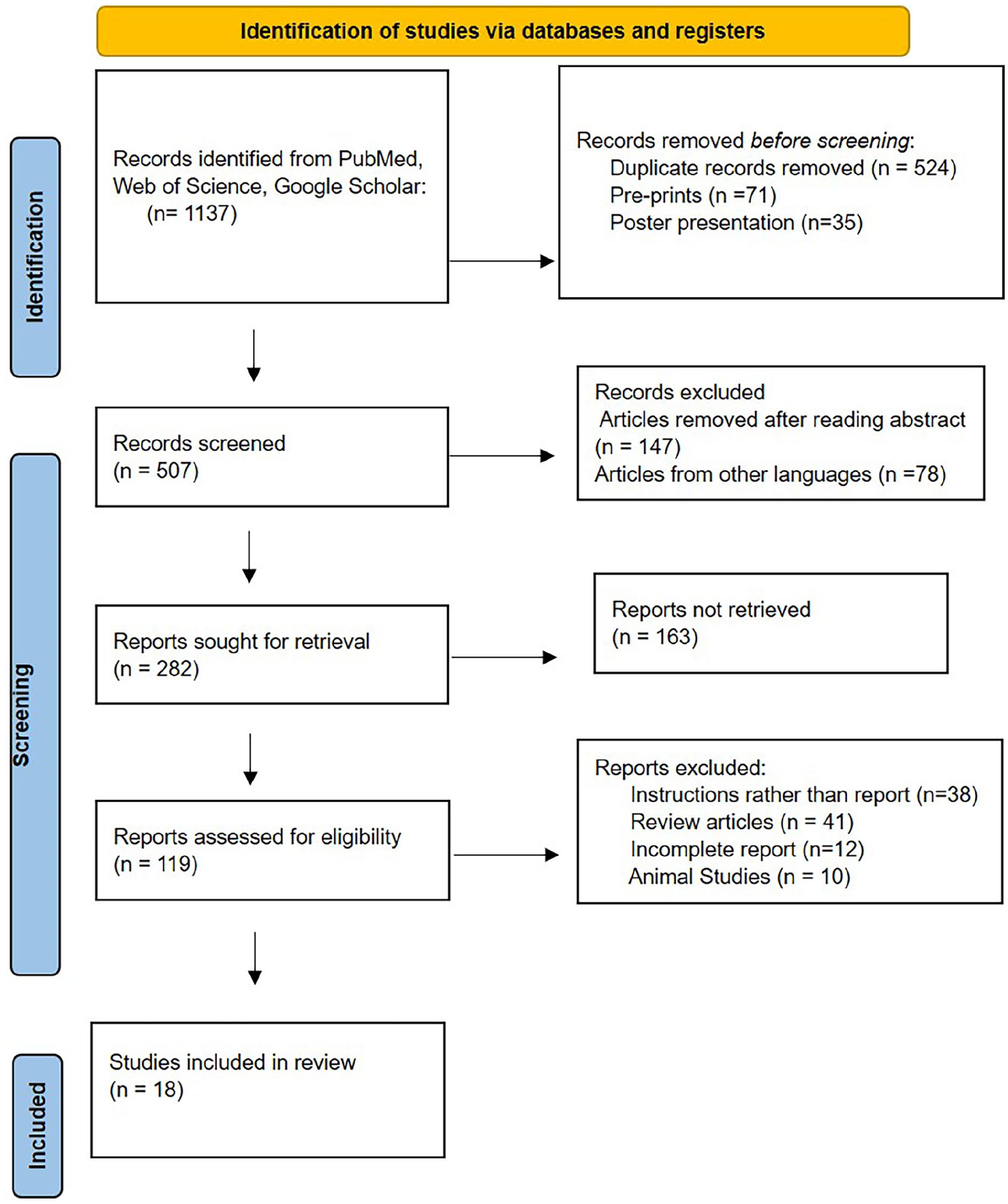
PRISMA flowchart for the review.
Risk of Bias Assessment
Every study that was part of the review had its risk of bias carefully evaluated. Selection bias, performance bias, detection bias, attrition bias, and reporting bias were among the criteria used in the assessment. The Cochrane Risk of Bias Tool was utilized for randomized trials, and the NOS was used for non-randomized research to assess each study. The risk of bias in studies was rated as low, moderate, or high. Sensitivity analyses were incorporated into the bias mitigation process to eliminate high-bias studies from pooled results to improve reproducibility. Reevaluating flagged research using more stringent NOS criteria was done in addition to employing a consensus approach to resolve disputes. While K.C., C.S., and A.D. studied reporting and performance biases, K.K. and A.B. evaluated selection and detection biases. Bias rating disagreements were settled by a consensus or a discussion.
Results
This study did not conduct a meta-analysis because of the substantial heterogeneity seen in the included trials. The total impact size of the link between OSMF and hearing impairment could not be quantitatively analyzed due to variations in methods, diagnostic instruments, participant selection criteria, and outcome measures amongst research. Thus, instead of combining data into a single statistical model, a systematic review was carried out to highlight important patterns and connections and summarize the results from the numerous investigations.
Prevalence and Correlation Between OSMF Severity and Hearing Loss
Studies examining the association between hearing impairment and OSMF severity are compiled in Table 1. Hearing loss was repeatedly found to be significantly correlated with the severity of OSMF, with patient-reported hearing problems ranging from 27.69% to 76.7%. Shah and Lunagariya 1 discovered that 30% of people had hearing loss, but Devi et al 3 and Jha et al 10 revealed that 44% and 46% of their respective cohorts had hearing impairment. According to Chandran and Aswath 5 and Harkare et al, 11 ETD was frequently found to be a contributing factor to these auditory abnormalities. Studies primarily employed PTA and tympanometry as audiological assessment methods. Singh et al 2 and Srivastava et al 6 stressed the importance of early detection and management of hearing impairment in OSMF patients to improve clinical outcomes.
Characteristics of Included Studies.
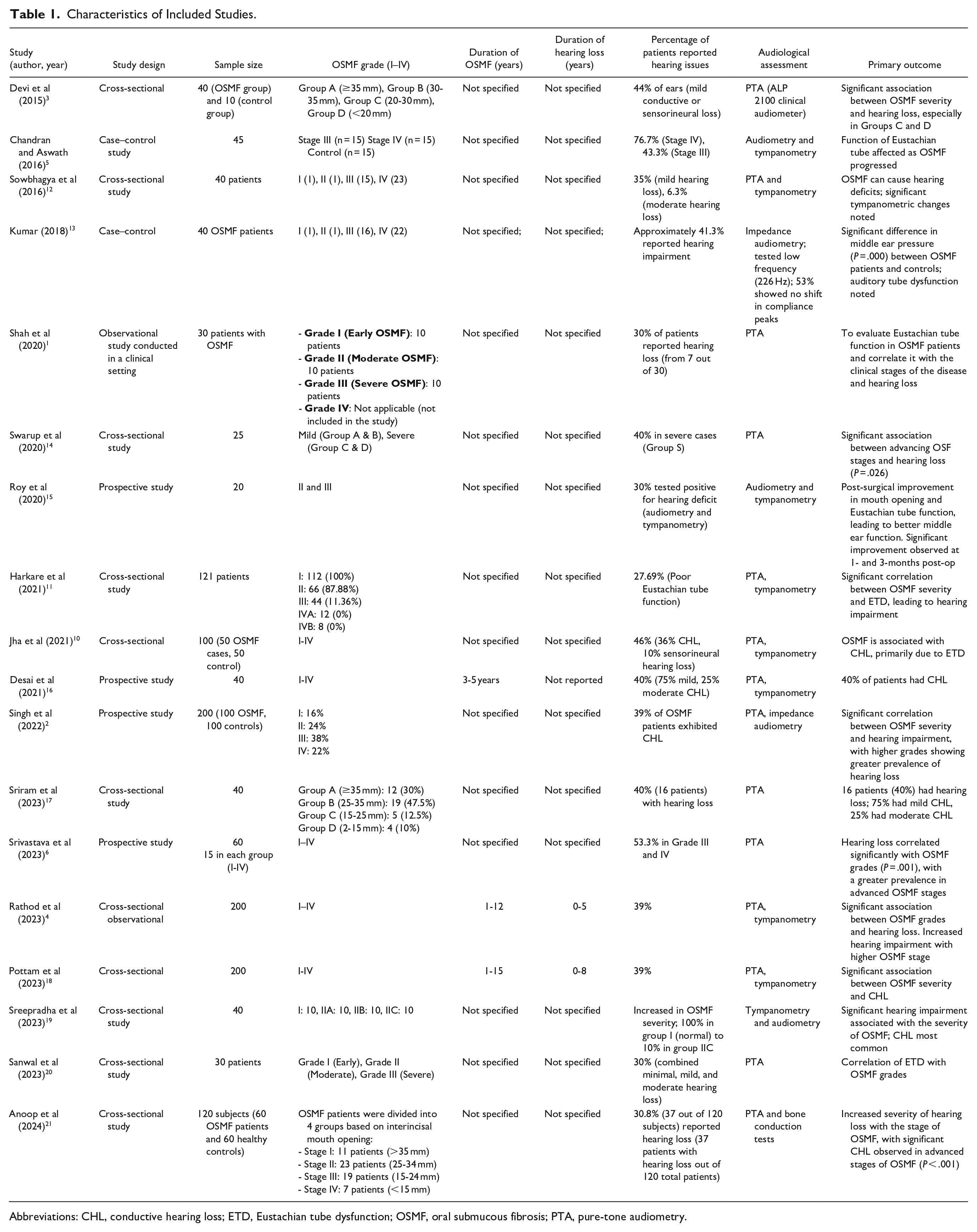
Abbreviations: CHL, conductive hearing loss; ETD, Eustachian tube dysfunction; OSMF, oral submucous fibrosis; PTA, pure-tone audiometry.
Symptoms and Audiological Findings
The symptoms of OSMF and how they relate to hearing loss are listed in Table 2. Burning feelings, limited mouth opening, and trouble swallowing were common complaints. The most common kind of hearing loss was found to be conductive. According to Devi et al, 3 44% of ears had hearing loss, but Chandran and Aswath 5 found that patients with Stage IV OSMF had a greater rate of hearing loss (76.7%). Harkare et al 11 and Kumar 13 both found a strong correlation between OSMF severity and ETD, indicating that higher levels of auditory impairment may be associated with more severe OSMF.
OSMF Symptoms and Audiological Findings.
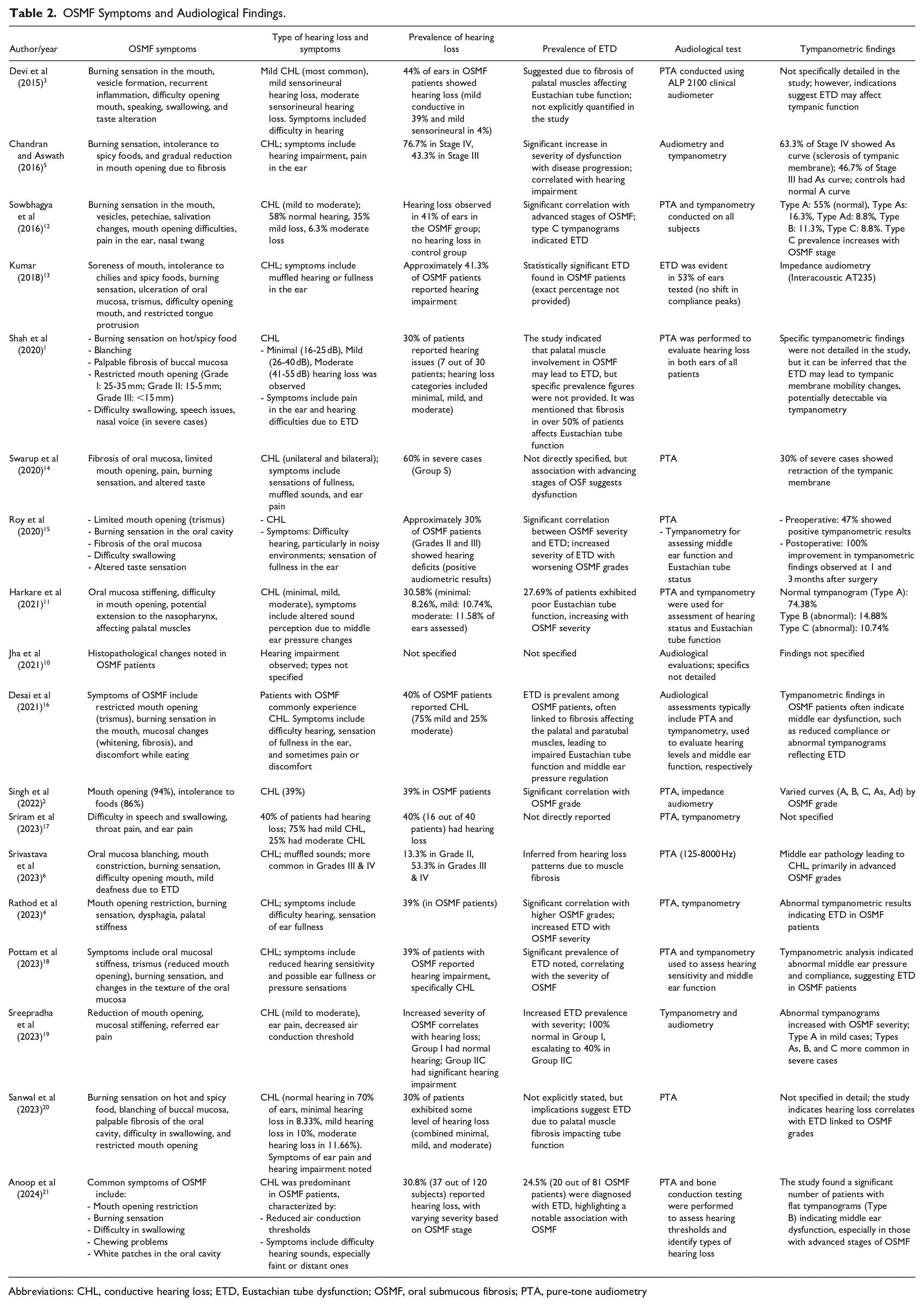
Abbreviations: CHL, conductive hearing loss; ETD, Eustachian tube dysfunction; OSMF, oral submucous fibrosis; PTA, pure-tone audiometry
Hearing Evaluation Methods
A description of the hearing evaluation techniques applied in each study is given in Table 3. The most widely used diagnostic method was PTA, which evaluated frequencies between 250 and 8000 Hz. According to Devi et al, 3 39% of patients had mild conductive hearing loss, and there were strong correlations between the severity of OSMF and hearing impairment. Chandran and Aswath 5 reported a high prevalence of conductive hearing loss and impaired Eustachian tube function, especially in advanced OSMF stages such as Stage IV, where tympanometric findings indicated sclerotic tympanic membranes. Kumar 13 used impedance audiometry to identify poor Eustachian tube function in 53% of ears. Atypical tympanometric findings were also observed in other research, such as Roy et al 15 and Harkare et al, 11 which linked them to the severity of OSMF and different levels of conductive hearing loss. According to tympanometric data, which showed ETD, 75% of the participants in the study by Desai et al 16 had mild conductive hearing loss. Recent research by Sreepradha et al 19 and Anoop et al 21 highlighted the significance of assessing middle ear mechanics and found that flat tympanograms, a sign of middle ear dysfunction, were quite common.
Methods of Hearing Evaluation in OSMF Studies.
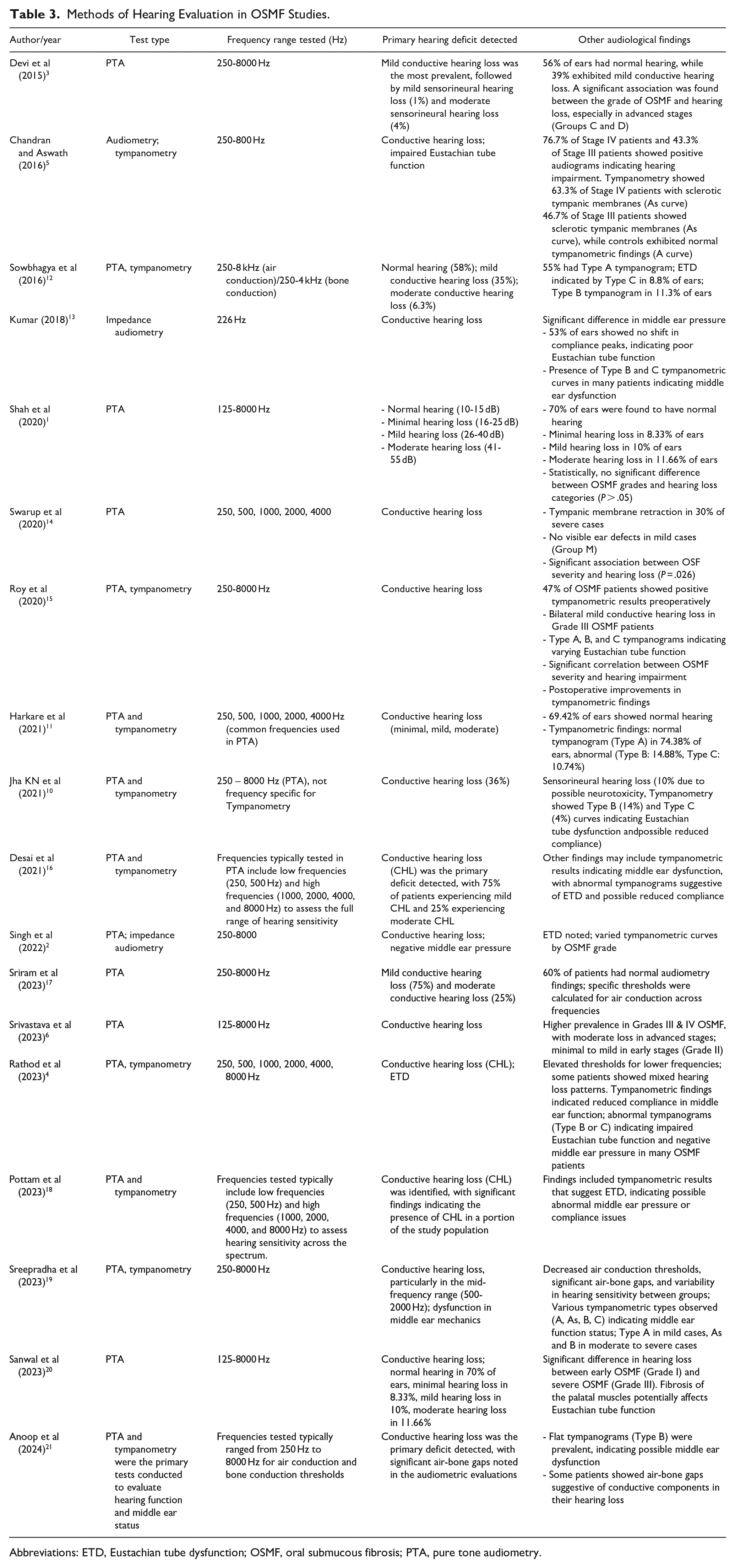
Abbreviations: ETD, Eustachian tube dysfunction; OSMF, oral submucous fibrosis; PTA, pure tone audiometry.
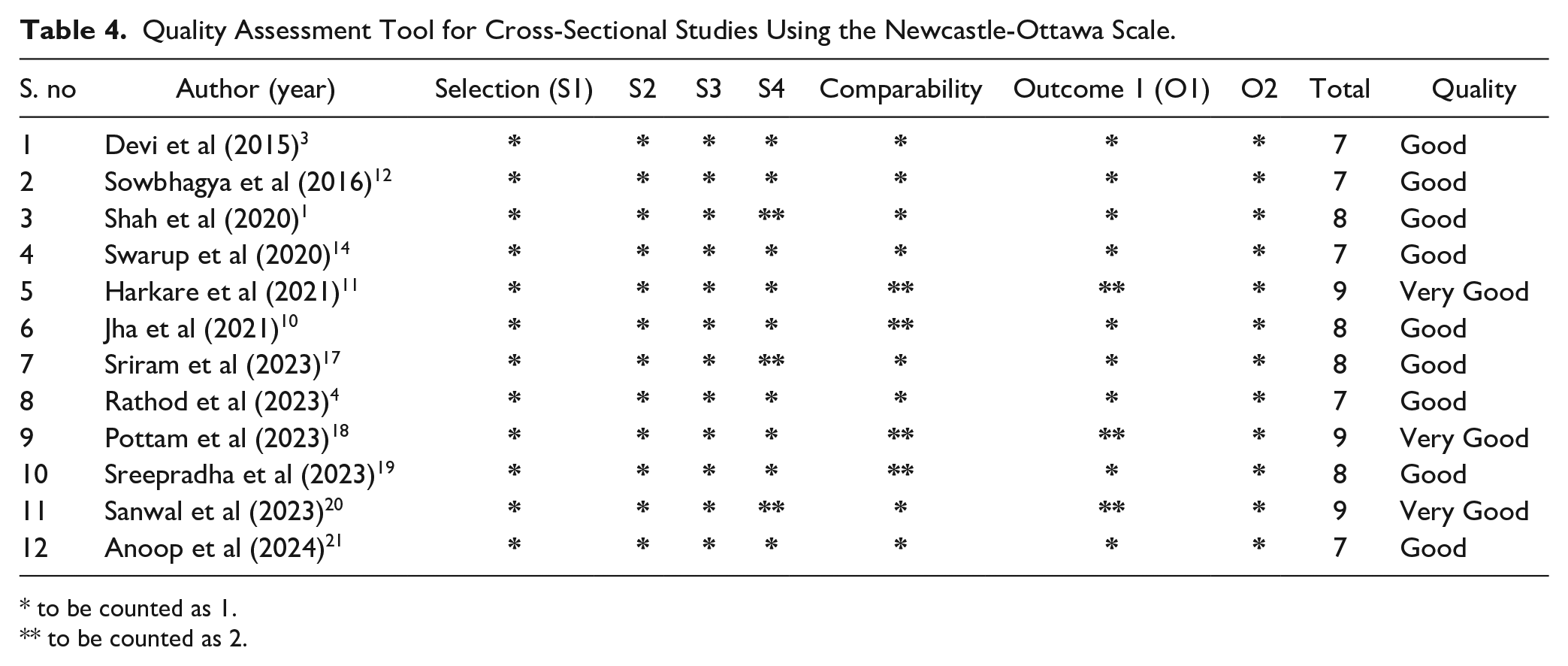
Quality Assessment of Cross-Sectional Studies
The NOS is used in Table 4 to assess the methodological quality of cross-sectional research on hearing loss in OSMF patients. A “Good” rating was given to most investigations, indicating sound methodological practices. With a score of 9, Harkare et al 11 received a “Very Good” grade, indicating robust results, comparability, and selection criteria that point to trustworthy conclusions on conductive hearing loss and tympanometric data. Pottam et al 18 also received a score of 9, highlighting the importance of comprehensive assessments of middle ear function and hearing loss. Sanwal et al 20 showed a substantial correlation between hearing impairment and OSMF severity, with a score of 9. These findings underscore the importance of rigorous study design in understanding the audiological implications of OSMF.
Quality Assessment Tool for Cross-Sectional Studies Using the Newcastle-Ottawa Scale.
to be counted as 1.
to be counted as 2.
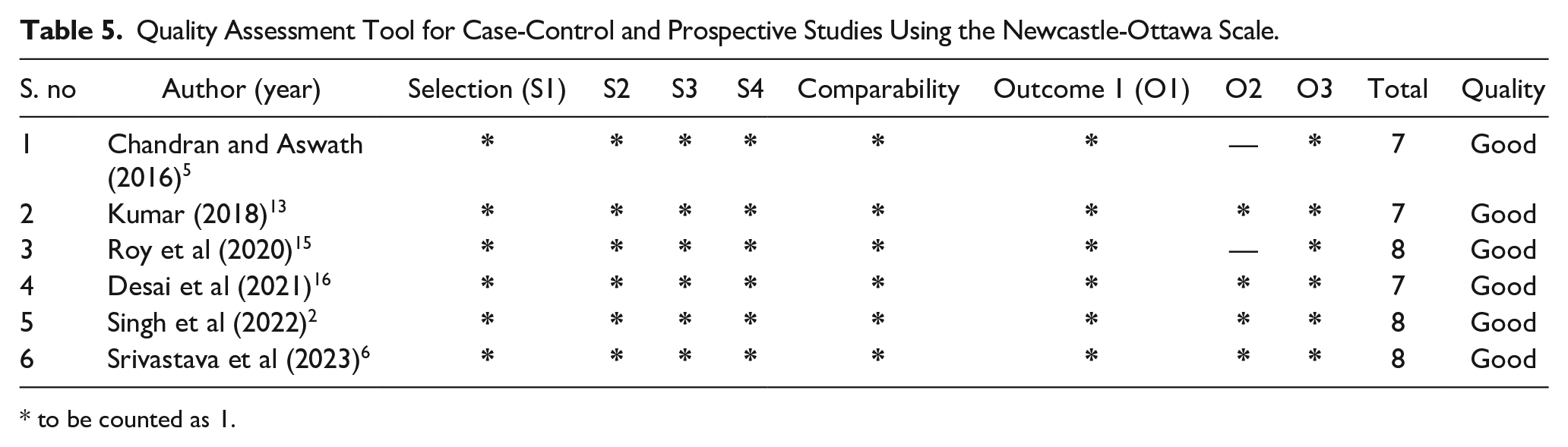
Quality Assessment of Case–Control and Prospective Studies
Table 5 evaluates case–control and prospective studies on hearing loss in OSMF patients. All studies received a “Good” rating, indicating robust methodologies. Notably, Roy et al, 15 Singh et al, 2 and Srivastava et al 6 scored 8, reflecting strong selection, comparability, and outcome measures. These studies provide valuable insights into the prevalence and types of hearing loss associated with OSMF. However, studies such as Chandran and Aswath 5 , Kumar, 13 and Desai et al, 16 with scores of 7, suggested that there is potential for methodological improvements.
Quality Assessment Tool for Case-Control and Prospective Studies Using the Newcastle-Ottawa Scale.
to be counted as 1.
Bias Analysis
Figures 2 and 3 illustrate the bias analysis of the included studies. The majority of studies showed proper data collection procedures, and the risk of bias was generally minimal, particularly with regard to confounding (D1) and exposure assessment (D2). Significant differences in participant selection (D3) were noted, though, with certain studies showing higher risks because of non-representative sample selection. The most biased treatments were found to be post-exposure interventions (D4), indicating that hearing results may have been impacted by therapies administered after an OSMF diagnosis. Concerns were also raised by several studies about missing data (D5), which would make the conclusions less compelling overall. Numerous investigations showed a minimal risk of outcome measurement (D6) despite these problems, suggesting accurate evaluations of hearing impairment. Selective reporting (D7) was still a problem in several trials, though. Overall, the body of evidence regarding the audiological effects of OSMF needs to be strengthened by addressing issues with participant selection, missing data, and post-exposure interventions, even though many studies corrected for exposure measurement and confounding variables. Future research should think about performing a subgroup analysis depending on OSMF severity (mild, moderate, or severe) to determine whether hearing impairment is more noticeable in advanced instances, given the variation in results among studies. Factors including age, length of OSMF, and chewing tobacco use should also be considered in subgroup analysis. Furthermore, utilizing I2 statistics to address statistical heterogeneity and considering the possible influence of various diagnostic techniques may offer important insights into the causes of the findings’ variability.
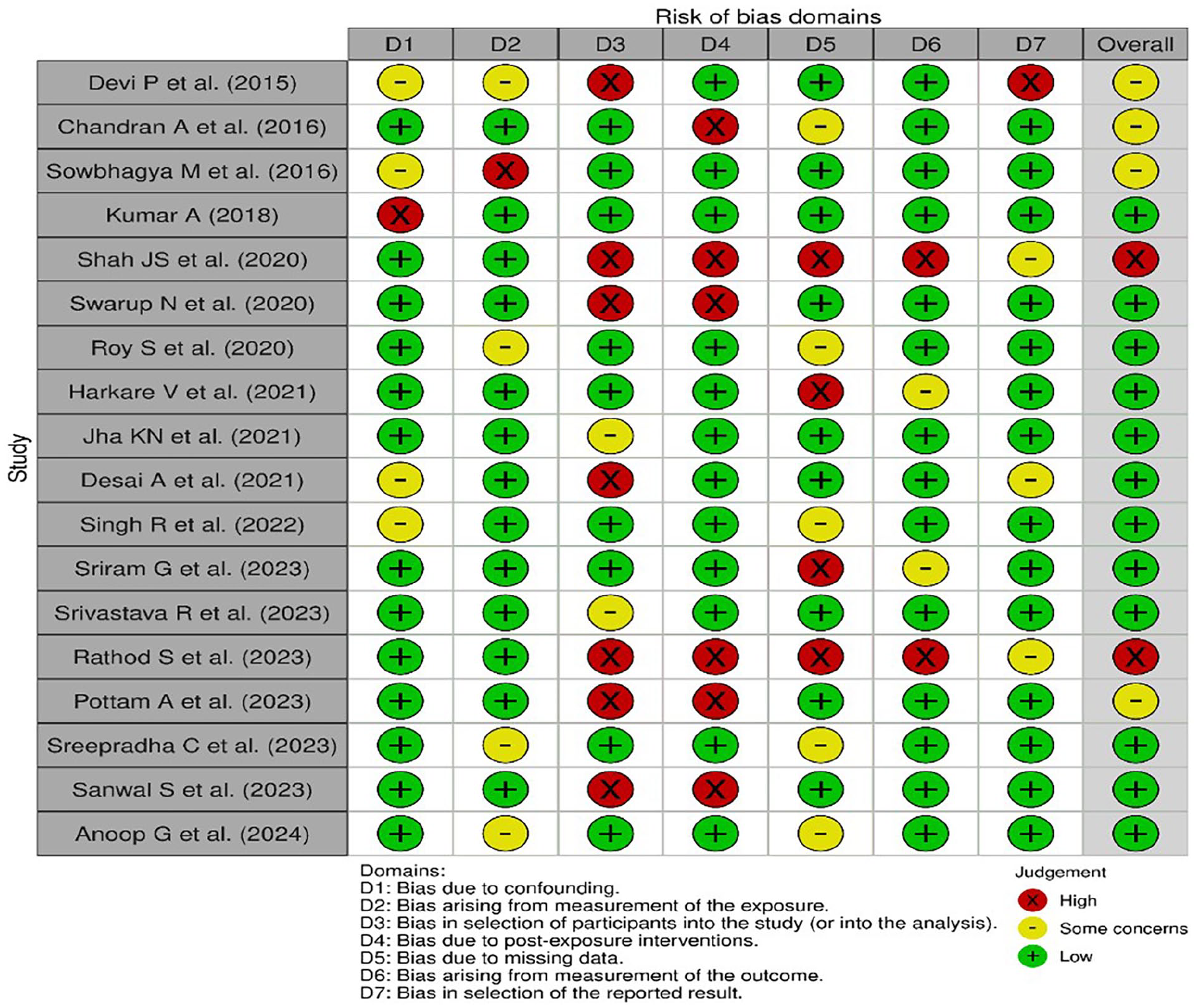
Individual risk of bias assessment using ROBINS – E Tool.
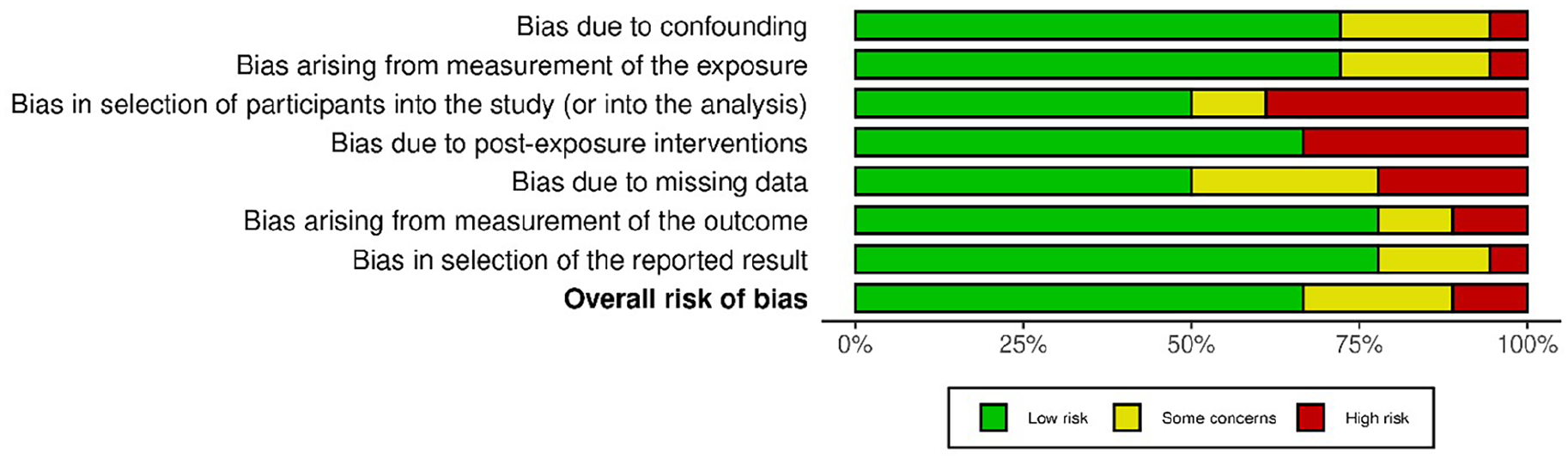
Overall risk of bias assessment using ROBINS – E Tool.
Discussion
OSMF is becoming more well acknowledged as a complicated disorder that presents serious health risks, especially in areas where areca nut intake is common. Even though earlier research has linked OSMF to several issues, such as dysphagia and oral cancer, the precise connection between OSMF and hearing loss is still unknown. There is a significant lacuna in the literature about the pathophysiological processes and magnitude of the association between OSMF and auditory impairment, even in the face of accumulating evidence that suggests this association may exist. By combining the results of several research that investigated hearing loss in patients with OSMF, this systematic review seeks to address these gaps in literature. It is critical to comprehend this relationship because hearing loss can significantly damage a patient’s quality of life and make managing OSMF more difficult. Two reasons justify concentrating on this topic: first, it highlights the potential audiological effects of an already challenging condition; second, it encourages the application of interdisciplinary approaches in OSMF treatment. Healthcare professionals can improve early detection and intervention, which will eventually improve patient outcomes, by including audiological tests into the routine care of patients with OSMF.
The inflammatory processes linked to OSMF may give rise to ETD, a mechanism for hearing impairment in patients with OSMF. Prolonged inflammation can cause fibrosis, which impairs the anatomy of the middle ear and the Eustachian tube’s ability to function. There is a correlation between the high prevalence of conductive hearing loss observed in advanced OSMF and the alteration of middle ear mechanics caused by inflammation. Siddiqui et al discovered this strong correlation between ETD and hearing loss, pointing out that fibrosis and inflammation can block the Eustachian tube, affecting pressure equalization that is essential for proper auditory function. 8 Similarly, a tympanometric investigation by Chandran and Aswath revealed that individuals with OSMF had impaired Eustachian tube function because of fibrotic alterations in the oral cavity. 5 The meta-analysis by Rathod et al highlighted the patients’ increased risk of developing ETD by indicating that the affected auditory structures may be impacted by fibrotic alterations that go beyond the mouth mucosa. 22 The correlation between auditory abnormalities and the clinical and histological severity of OSMF was confirmed by Singh et al, 2 demonstrating that fibrosis has a substantial effect on middle ear function and hearing. 2 The complex link between OSMF, ETD, and hearing impairment is shown by these data taken together, highlighting the significance of assessing auditory function in OSMF patients for efficient therapeutic management.
Considerable information on the hearing capacities of patients with OSMF has been gleaned from studies employing audiological diagnostic techniques. PTA is the method of assessment that is used the most frequently among these approaches. However, to gain a more comprehensive understanding of auditory function in OSMF patients, it is essential to include additional methods such as tympanometry and acoustic reflex tests. In addition to evaluating middle ear function, tympanometry can be used to diagnose disorders including ETD, which is frequently linked to OSMF. 8 Acoustic reflex testing further evaluates the auditory pathway and can indicate the status of the stapedius muscle in response to loud sounds, providing additional useful information about the integrity of the auditory system. 5
It is noteworthy that combining these complimentary assessments improves the evaluation of the connection between auditory abnormalities and OSMF severity. Healthcare providers can more precisely determine the degree of hearing impairment which is often underdiagnosed and undertreated in this population by using a comprehensive approach to audiological assessment. 4 These comprehensive evaluations are crucial for tailoring effective intervention strategies and ensuring that patients receive the appropriate therapy for their auditory needs.
The relationship between the degree of hearing loss and the duration as well as the severity of OSMF is a significant finding that needs more research. Research has shown a substantial correlation between the duration of OSMF and the degree of hearing loss, suggesting that patients with a longer history of the disorder typically have more severe auditory impairments.6,23 The discovery emphasizes the vital necessity of prompt diagnosis and treatment of OSMF to reduce the likelihood of hearing impairment. Regular audiological monitoring is crucial since OSMF being a chronic condition is frequently characterized by a progressive deterioration of symptoms. Early detection of hearing problems can be facilitated by such surveillance, enabling prompt interventions. 24
Moreover, as OSMF progresses, the associated degree of hearing impairment tends to escalate, reinforcing the necessity for proactive management strategies. 24 Additionally, preoperative evaluations often reveal significant hearing loss in OSMF patients, which can be exacerbated without appropriate treatment. 25 Overall, the interplay between OSMF duration, severity, and hearing loss calls for heightened awareness and regular auditory assessments to ensure optimal patient outcomes.
Recent research has focused a great deal of emphasis on the function of areca nut in the pathophysiology of OSMF and its possible connection to hearing impairment. Consuming areca nuts is linked to several systemic side effects, such as potential ototoxicity, which could impair auditory function. Long-term areca nut usage may cause systemic alterations that affect hearing function, possibly through inflammatory pathways, according to research by Gupta et al. 26 This research highlights the critical need for public health initiatives targeted at lowering its usage and raises serious concerns about the wider effects of lifestyle decisions, such as the use of areca nuts, on the health of the hearing in OSMF patients.
Hearing impairment may also be indirectly caused by psychosocial issues associated with living with OSMF, in addition to ETD. Psychological discomfort is common in patients with chronic diseases, and it can increase awareness of sensory abnormalities, including hearing loss. According to research by Chaudhary, 27 psychological assistance may be essential for improving overall health outcomes, including auditory function, as it underlines the psychosocial burden experienced by OSMF patients. Both the physical and psychological components of OSMF have a substantial impact on the overall quality of life (QoL) of those who have the condition. OSMF causes pain, trouble swallowing, and limited mouth opening, all of which can make it harder to go about everyday tasks. In addition to these physical limits, patients may also face social and emotional difficulties, such as low self-esteem, diminished social relationships, and shame. Furthermore, because OSMF is chronic, there is frequently ongoing concern about the possibility of getting oral cancer. The QoL of OSMF patients must be handled holistically, combining medical and psychosocial support to enhance general well-being.9,28
It is critical to address mental health in addition to physical health because doing so could greatly improve the QoL of patients affected by OSMF. For this reason, comprehensive care plans that combine psychological and medicinal therapies are necessary to maintain auditory function and optimize health outcomes in this population. The audiological profile of patients with OSMF may be complicated by the coexistence of systemic and oral diseases. Studies show that people with OSMF are more likely to have comorbid conditions such as diabetes and hypertension, which have both been linked to hearing loss.2,38,29 Thus, to properly manage these comorbidities and comprehend their combined impact on hearing function, a multidisciplinary strategy involving dentists, audiologists, and general healthcare practitioners is necessary.
There are still numerous shortcomings in the research that have been done on OSMF and hearing impairment, despite the expanding volume of literature. Small sample sizes are a common characteristic of research, which limits how broadly the results may be applied. Direct comparisons between studies are further complicated by differences in patient demographics, audiological evaluation techniques, and study designs. Future research should prioritize larger, multicenter trials employing standardized assessment protocols to yield more robust data regarding the prevalence and mechanisms of hearing loss in OSMF patients.23,30,31 It will be essential to close these gaps to create complete management plans that improve patient outcomes. In the end, better therapy, and a higher standard of living for those impacted by OSMF will result from a full grasp of the interactions between the disorder, its comorbidities, and hearing loss.
Strengths and Limitations
The literature on OSMF and hearing impairment is thoroughly synthesized in this systematic review, which also highlights important relationships and important processes. This review’s strength is its thorough methodology, methodical approach, and inclusion of a variety of articles, all of which improve the validity of the findings. However, several restrictions need to be solved. The findings’ generalizability may be impacted by the small sample numbers, inconsistent diagnostic tool use, and possible publication bias of many of the included studies. The results could have been affected by confounding factors like alcohol use, smoking, and nutritional deficits, whose effects were not always taken into consideration. To give more trustworthy evidence about the effect of OSMF on hearing health, future research should concentrate on bigger, multicenter trials using established procedures and take longitudinal outcomes into account.
Conclusion
This review highlights a significant association between OSMF and hearing impairment, including both conductive and sensorineural hearing loss. The hearing issues are likely due to fibrotic changes affecting the middle ear and Eustachian tube. Despite some methodological challenges, such as participant selection bias, inconsistent therapies, and missing data, the studies consistently link OSMF with hearing loss, indicating that the fibrosis involved may impact not only the oral cavity but also auditory structures, affecting hearing.
Future research should focus on several key areas. Longitudinal studies are essential to determine whether early intervention, including medical or surgical treatments, can reduce hearing loss over time and establish a clearer causal relationship between OSMF and hearing impairment. Additionally, while conductive hearing loss has been well-studied, more research is needed on sensorineural hearing loss in OSMF patients, particularly to explore potential systemic effects or damage to the inner ear and auditory nerve. Larger, multicenter trials with consistent audiological evaluations and standardized diagnostic criteria are crucial for reducing biases and improving the quality of the evidence. These efforts will help develop better clinical care plans for OSMF patients.
Key Findings
A significant association between the severity of OSMF and conductive hearing loss.
ETD as a likely mechanism for hearing loss in OSMF.
Sensorineural hearing loss observed in some OSMF patients, possibly due to systemic effects or comorbidities.
Based on these findings, routine audiological screening, particularly for severe OSMF patients or those with a history of areca nut use, is recommended. Early detection can improve outcomes by enabling timely interventions.
Footnotes
Acknowledgements
None.
Data Availability Statement
No patient data were used in the study; hence, there is no data availability statement furnished.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Ethical Statement
Ethical approval was not required.
Patient Consent
Not applicable.
Trial Registration Number and Date
Not applicable.
Grant Number
Not applicable.