
Abstract
Pituitary macroadenomas are benign neoplasms that can cause a range of symptoms due to a mass effect on surrounding structures. This case report describes a 51-year-old male presenting with progressive bilateral hearing impairment and significant deterioration in speech discrimination over several years. Examination revealed normal tympanic membranes and no neurological deficits, while pure tone audiometry indicated mild to moderate sensorineural hearing loss. Magnetic resonance imaging identified a 6 × 5.5 × 7 cm pituitary macroadenoma extending into the suprasellar region and invading the sphenoid and right cavernous sinuses. The patient underwent a two-stage surgical intervention followed by gamma knife surgery. Postoperative follow-up showed mild deterioration in hearing with unmeasurable speech discrimination scores. This case underscores the importance of considering pituitary macroadenomas in the differential diagnosis of unexplained hearing loss and highlights the role of comprehensive audiological and imaging evaluations in achieving accurate diagnosis and optimal management.
Introduction
The pituitary gland, approximately the size of a pea, is located in a small bony cavity (sella turcica) at the base of the brain. Pituitary adenomas are benign neoplasms originating from the cells of the pituitary gland. Although these tumors are common, their actual prevalence is not well known, as most are asymptomatic. Autopsy studies have found pituitary adenomas in up to 27% of patients. 1 While many pituitary tumors may remain asymptomatic with slowly developing, insidious, nonspecific complaints, thus delaying accurate diagnosis, some pituitary tumors cause prominent symptoms. Headaches and visual disturbances are the most frequent mass effect symptoms, but hearing impairment, particularly deterioration in speech discrimination, can also be the only symptom.2,3
Case Report
A 51-year-old otherwise healthy male presented to our ENT department with complaints of progressive bilateral hearing impairment that had developed over several years and had worsened in the past 2 weeks. He had previously noticed some hearing loss but had not sought evaluation.
On examination, the patient showed bilateral normal tympanic membranes and no neurological deficits. Pure tone audiometry revealed mild to moderate sensorineural hearing loss with air conduction thresholds of 34 dB in the right ear and 43 dB in the left ear. Speech discrimination scores were 68% in the right ear and 8% in the left ear (Figure 1A).
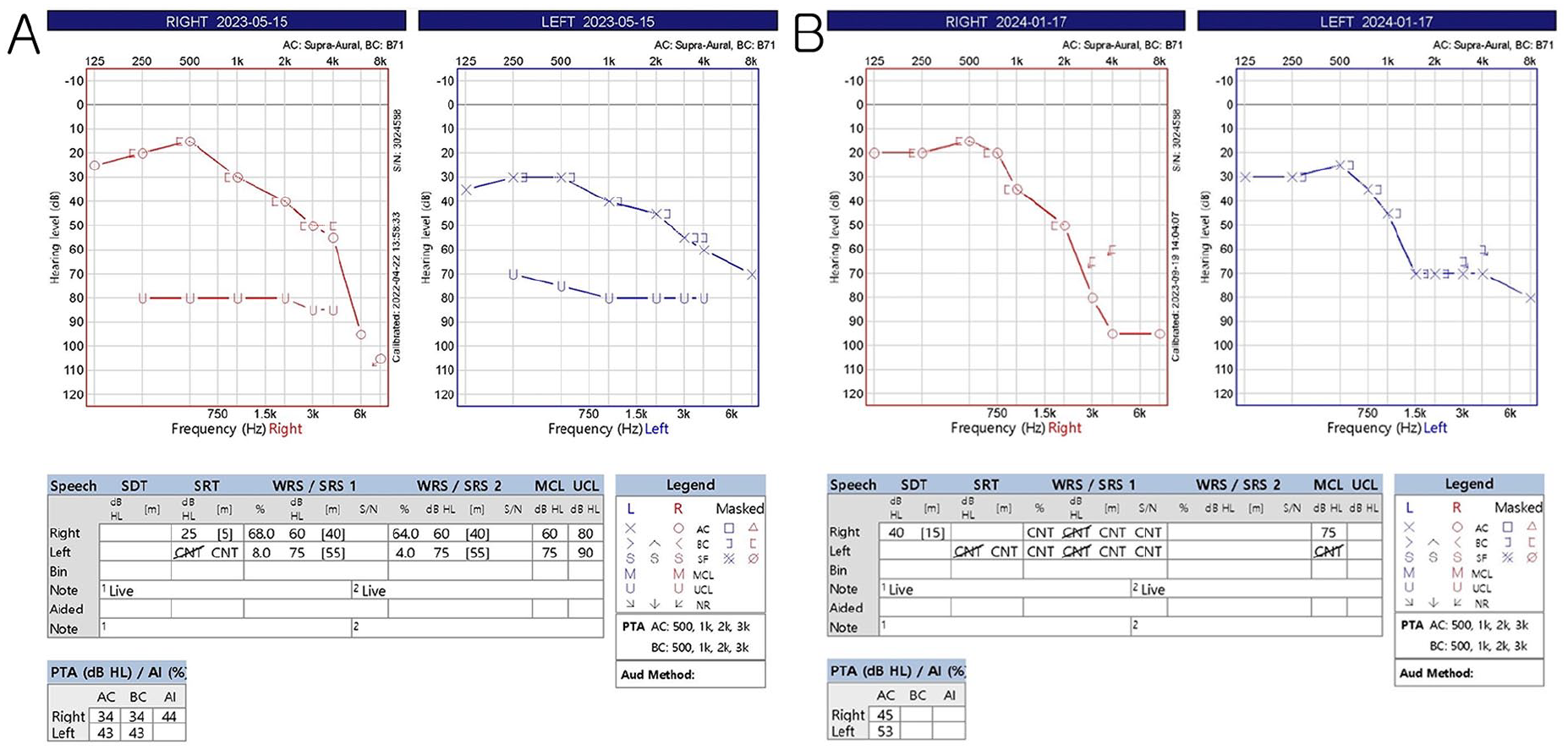
Initial pure tone audiometry and speech discrimination scores (A) and pure tone audiometry and speech discrimination scores after treatment (B).
Magnetic resonance imaging (MRI) was performed, revealing a 6 × 5.5 × 7 cm pituitary macroadenoma extending into the suprasellar region with invasion into the sphenoid sinus and right cavernous sinus (Figure 2).
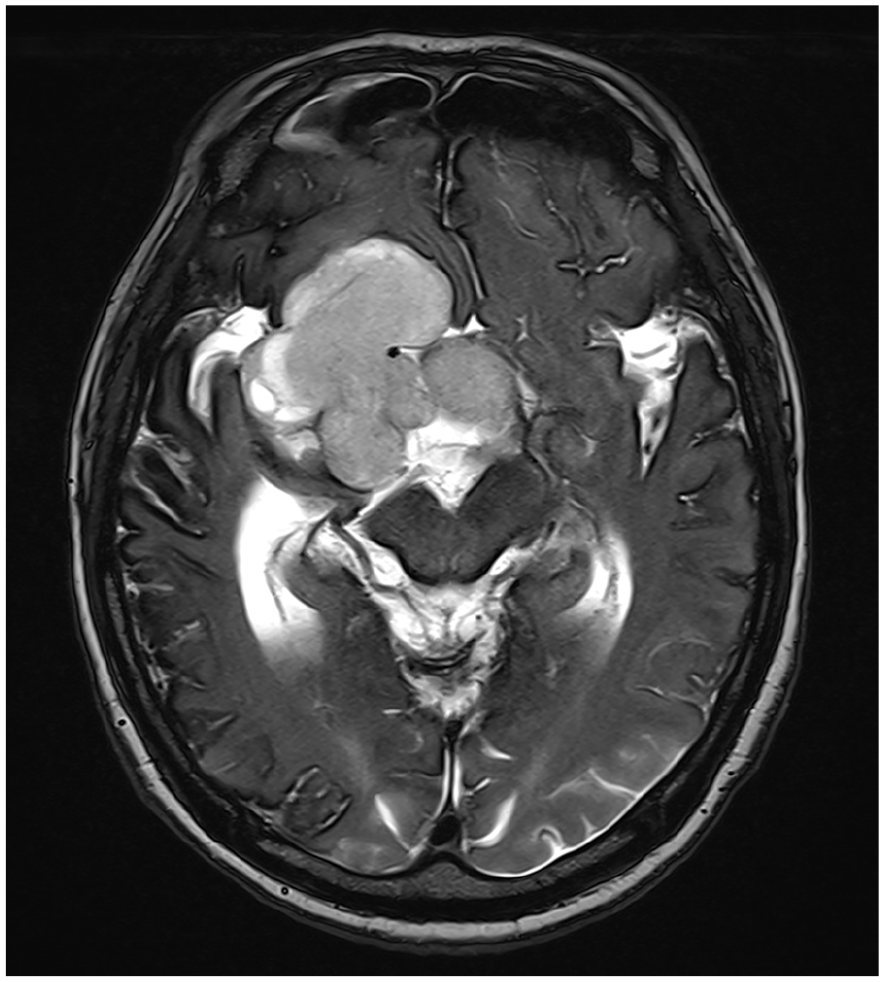
T2-weighted magnetic resonance imaging (MRI) revealed a large, homogeneous, enhancing mass filling the sella turcica, with invasion into the sphenoid sinus and right cavernous sinus, and extension into the suprasellar region, further extending to the right Sylvian fissure and frontotemporal fossa.
In consultation with the neurosurgery department, the patient underwent a 2-stage surgical approach: an endonasal transsphenoidal approach (TSA) followed by craniotomy for tumor mass removal. A follow-up MRI showed a decrease in tumor size in the suprasellar area but no interval changes in the right cavernous sinus and infratentorial fossa. Six months after the initial surgery, the patient underwent additional gamma knife surgery.
Seven months post-surgery, a follow-up hearing test showed a mild deterioration in sensorineural hearing loss of about 10 dB, with air conduction thresholds of 45 dB in the right ear and 53 dB in the left ear. Speech discrimination scores were not measurable on either side (Figure 2B).
Discussion
Pituitary macroadenomas are significant due to their potential to cause symptoms through a mass effect on surrounding structures, such as the optic chiasm, cavernous sinuses, and cranial nerves. This case illustrates an atypical presentation of pituitary macroadenoma with primary symptoms of hearing loss and poor speech discrimination, emphasizing the need for thorough evaluation in patients with unexplained auditory deficits.
The deterioration in speech discrimination in this patient suggests a retrocochlear pathology, which can be associated with various intracranial lesions, including pituitary adenomas. The lack of typical neurological or visual symptoms in this case highlights the complexity and variability in the presentation of pituitary adenomas, necessitating a high index of suspicion in atypical cases. 4
MRI remains the gold standard for diagnosing intracranial pathologies, including those presenting with auditory symptoms. 5 However, its use as an initial diagnostic tool in patients with hearing loss and no other neurological symptoms can be challenging due to cost, accessibility, and the relatively lower index of suspicion for intracranial pathology in such cases. Nevertheless, this case underscores the importance of considering MRI in patients with unexplained hearing loss, especially when there is significant deterioration in speech discrimination. 6
The treatment approach for pituitary macroadenomas often involves surgical resection, particularly in cases with significant mass effects or symptomatic presentation. The endonasal TSA is a commonly used surgical technique due to its minimally invasive nature and effectiveness in accessing the pituitary region. 7 However, complete resection can be challenging, especially when the tumor extends into areas such as the cavernous sinus. Adjuvant therapies, such as gamma knife surgery, play a crucial role in managing residual tumors and preventing recurrence. 8
Conclusion
This case highlights the unusual presentation of sensorineural hearing loss associated with a pituitary macroadenoma. While pituitary macroadenomas are rare and typically identified incidentally during imaging for other symptoms such as headache or visual disturbances, this case underscores the importance of thorough evaluation in patients with unexplained sensorineural hearing loss, particularly when significant speech discrimination deficits are present. In the modern diagnostic era, imaging, particularly MRI, is the standard of care and is crucial in identifying rare intracranial pathologies like macroadenomas that may underlie auditory symptoms. Multidisciplinary collaboration is essential for optimal management, involving otologists, radiologists, and neurosurgeons to achieve the best possible patient outcomes.
Footnotes
Acknowledgements
This study was supported by a fund from the Biomedical Research Institute at Jeonbuk National University Hospital.
Author Contributions
Conceptualization: C.D.Y. Data curation: S.C.P., H.T.K., and S.L. Investigation: H.T.K. and S.L. Writing-original draft: S.C.P., H.T.K., and C.D.Y. Writing-review & editing: all authors.
Data Availability Statement
The datasets used and/or analyzed during the current study are available from the corresponding author upon reasonable request.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethics Approval
This study was approved by the Institutional Review Board of Jeonbuk National University Hospital, Korea (approval number: 2022-02-023). Informed written consent was obtained from the patient for publication of this case report and accompanying images.