
Abstract

Significance Statement
We report the first documented case of an obstructing nasal mass as a manifestation of Crohn’s disease in the sinonasal cavity. Nasal involvement in Crohn’s disease is exceedingly rare, with only 5 suspected cases previously reported. While extraintestinal manifestations of inflammatory bowel disease affect 25% to 40% of patients, they typically involve the joints, skin, mouth, and eyes. Nasal involvement is particularly uncommon and may present as nasal congestion, epistaxis.
Case Presentation
A 17-year-old male with a one-year history of Crohn’s disease was admitted to the pediatric emergency department after sustaining a minor nasal injury during routine sports activity, followed by epistaxis. The patient reported chronic nasal obstruction, which had worsened since the injury, accompanied by localized pain. At the time, he was asymptomatic from a gastrointestinal perspective and had been undergoing treatment with Infliximab (400 mg every 4 weeks) and azathioprine (50 mg daily). He was also scheduled for a routine follow-up colonoscopy.
On examination, the patient’s vital signs were stable, and there were no signs of facial tenderness or nasal discharge. Rhinoscopy revealed a non-tender granulated mass causing right-sided nasal obstruction, with no evidence of septal hematoma or other traumatic abnormalities (Figure 1). A computed tomography (CT) scan confirmed a soft tissue mass occluding the right nasal cavity (Figure 2).
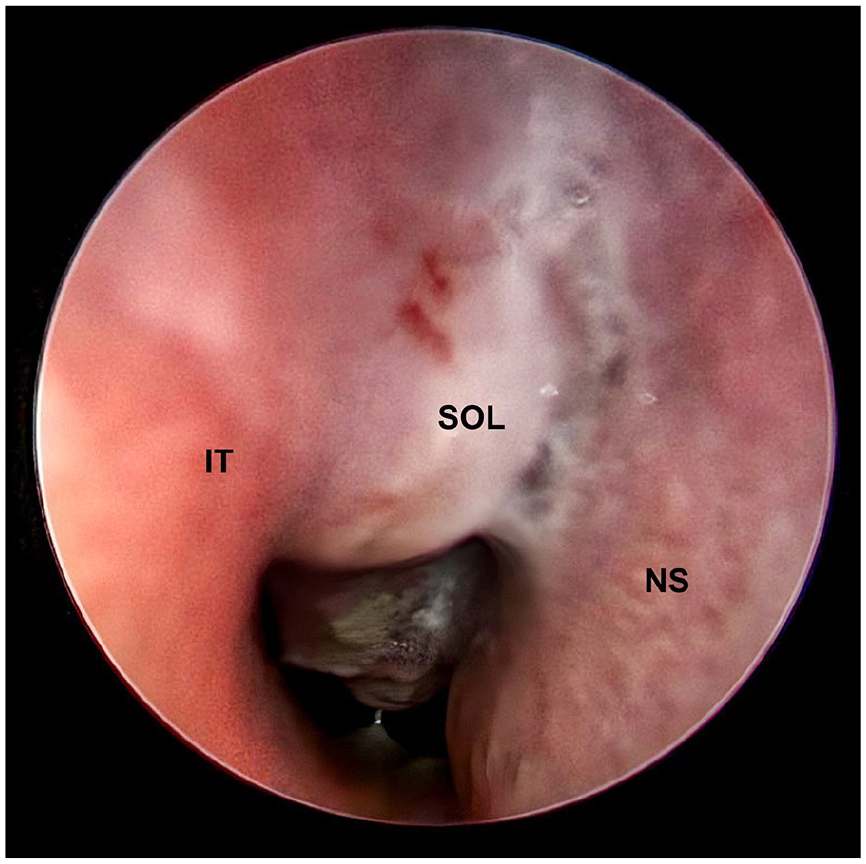
Endoscopic view of the right nasal cavity showing a space-occupying lesion (SOL) located between the inferior turbinate (IT) and the nasal septum (NS).
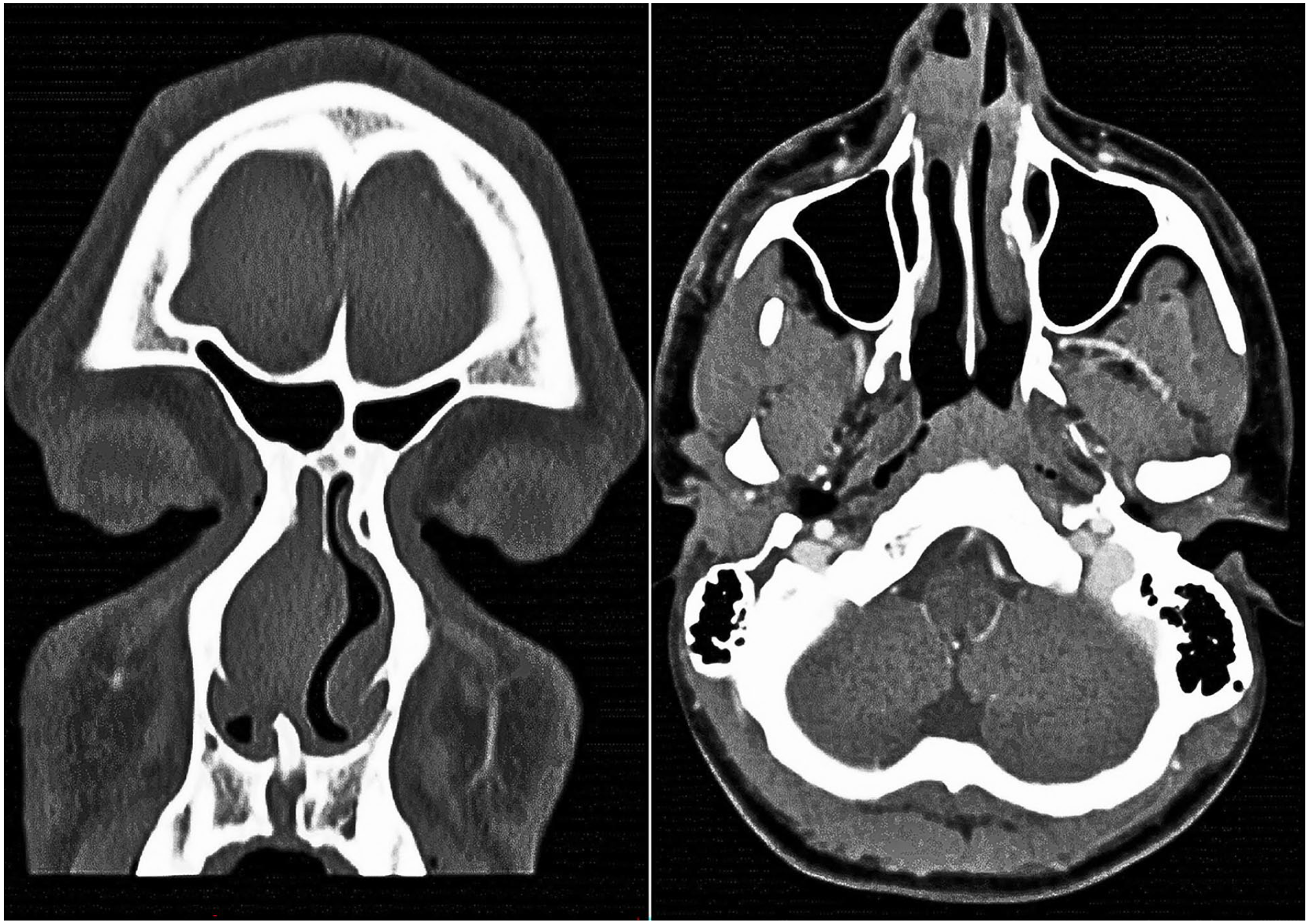
CT scan showing a soft tissue mass obstructing the right nasal cavity.
The patient was referred for surgical excision, during which a 3 cm cauliflower-like mass was removed from the right nasal septum, extending from the posterior region to the anterior part of the middle concha. The mass was excised along with the overlying mucosa while preserving the septal cartilage. Notably, the left nasal cavity was unaffected.
Histopathological analysis of the excised mass revealed extensive non-caseating granulomatous inflammation with multiple giant cells, T cells, and CD30+ cells, consistent with Crohn’s disease affecting the sinonasal cavity (Figure 3). A concurrent colonoscopy showed normal results, with only focally-active colitis in the transverse colon, indicating quiescent inflammatory bowel disease (IBD). Following the nasal biopsy result, the patient’s infliximab dose was increased from 400 mg every 4 weeks to 600 mg every 5 weeks.
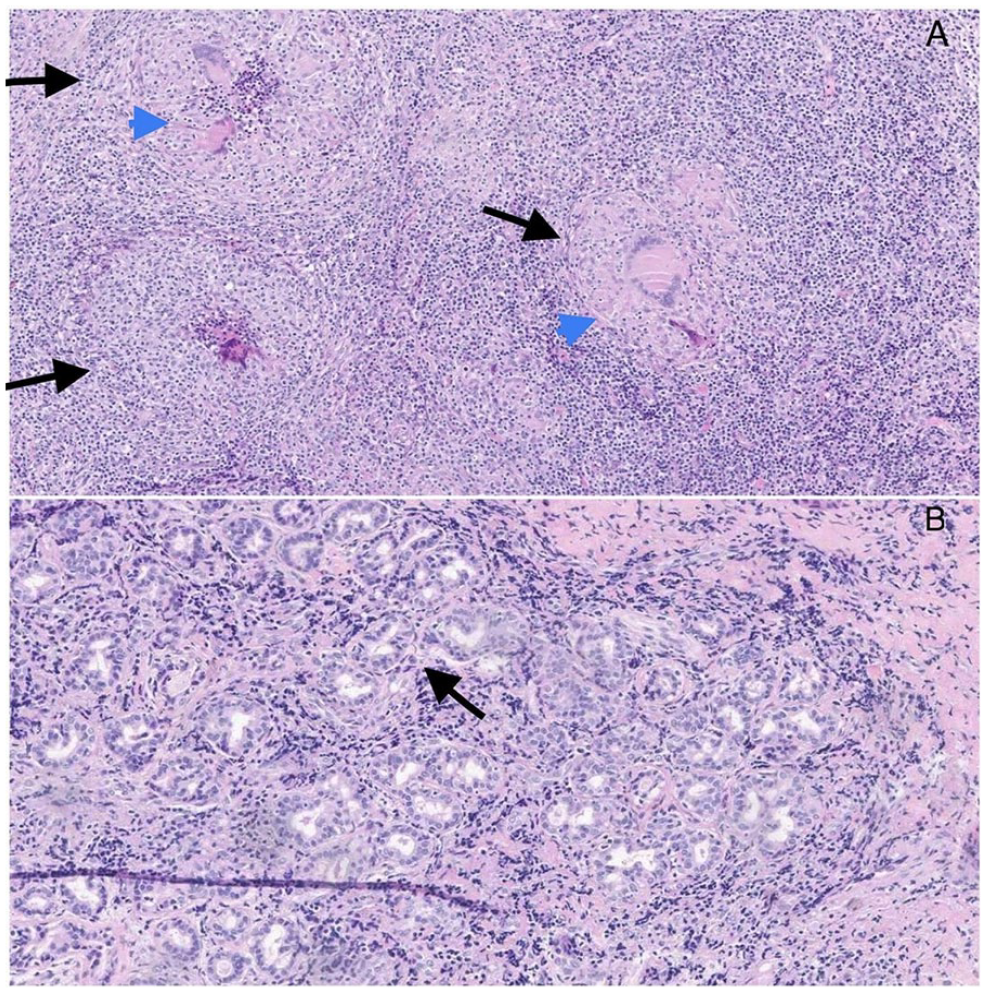
Histopathological examination of the sinonasal mucosa. (A) Multiple granulomas (indicated by arrows) with multinucleated giant cells (indicated by arrowheads). (B) Lymphocytes infiltrating the glands (indicated by arrow).
The patient was also treated postoperatively with topical saline irrigations, steroids, and ointments. Although he experienced some persistent nasal obstruction in the months following surgery, his sense of smell was preserved, and he had no further episodes of epistaxis or nasal pain.
Three months post-surgery, the patient presented with a non-tender lesion on the hard and soft palate, and a biopsy showed dense chronic inflammation without granulomas (Figure 4).

Transoral view showing a lesion on the hard palate, confirmed as compatible with Crohn’s disease based on tissue diagnosis.
Ten months after surgery, physical examination and a follow-up CT scan of the sinuses revealed no abnormal findings in the nasal cavity, and the patient’s most recent colonoscopy was normal.
Discussion
IBD, including Crohn’s disease, is a chronic condition of the gastrointestinal tract with a complex pathogenesis influenced by genetic and environmental factors. 1 Extraintestinal manifestations of IBD are common, but sinonasal involvement is rarely seen. To date, only 5 cases of suspected nasal Crohn’s disease have been documented in the English literature, each with different clinical presentations and treatments, which have ranged from topical and systemic steroids to surgical interventions and leukocytapheresis. To the best of our knowledge, this case is the first to describe an obstructing nasal mass as a manifestation of Crohn’s disease.
The exact mechanisms driving extraintestinal manifestations in IBD are still unclear. One leading hypothesis suggests that, in genetically-predisposed individuals, antigens from a compromised bowel barrier may activate the systemic immune system, leading to inflammation beyond the gastrointestinal tract. While many extraintestinal manifestations resolve with better bowel inflammation control, some, such as nasal involvement, may persist independently of bowel disease activity.2-6
Effective management of extraintestinal manifestations requires a careful consideration of both the severity of IBD and the potential impact on the patient’s quality of life.7,8 In this case, biopsy was essential in confirming the diagnosis of Crohn’s disease in the nasal cavity, differentiating it from other granulomatous conditions such as Wegener’s granulomatosis, sarcoidosis, tuberculosis, or sinonasal lymphoma. Histopathological findings, including granulomas and perivascular inflammation, are key diagnostic features, although granulomas may not always be present. 9
This case highlights the importance of considering sinonasal Crohn’s disease in patients with chronic IBD who present with nasal symptoms, such as obstruction or bleeding. Early recognition and intervention are crucial for improving patient outcomes and quality of life. This rare presentation highlights the need for a multidisciplinary approach in managing extraintestinal manifestations of Crohn’s disease, particularly in cases involving unusual anatomical sites such as the sinonasal cavity.
Footnotes
Author Contributions
T.Z.: conceptualization, literature review, and manuscript writing. S.H.: manuscript review and editing. I.V.: literature review. E.M.: data provision and pathology description. D.S.S.: gastroenterological assessment, manuscript review, and editing. G.A.: maxillofacial surgical assessment, manuscript review, and editing. R.H.: manuscript review. D.G.: manuscript supervisor.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Informed Consent
A written informed consent form was obtained from the patient’s legal guardian.