
Abstract
Introduction
Preauricular sinus is a congenital disease that was first described by Heusinger in 1865. Although it typically manifests as a pit near the anterior limb of the ascending helix, it has been reported near the posterior surface of the helical crus, cymba concha, ear lobule, and postauricular area. 1 Surgical treatment is recommended in cases of repeated preauricular sinus infection. However, consensus regarding the removal of a portion of the ascending helix cartilage during preauricular sinus surgery is lacking. Incomplete removal of sinus epithelial cells increases the risk of recurrence. The recurrence rate ranges from 0% to 42% with an average of 2.2%. A thorough understanding of the histopathological characteristics, particularly the relationship between the epithelial tract and perichondrium, may improve surgical decisions. Therefore, we retrospectively analyzed the histopathological characteristics of initial and recurrent cases in our medical group. Because most preauricular sinuses occur in the anterior region of the ascending helix, this study only included sinuses at this location.
Methods
This retrospective, single-center study was approved by the ethics committee of Wuhan Union Hospital. Written informed consent for the publication of anonymized information was obtained from the legally-authorized representatives of all patients.
Patients who underwent primary or revision preauricular sinus surgery at Wuhan Union Hospital between October 2020 and October 2021 were included. Primary surgeries were performed by the same surgeon, whereas revision surgeries were performed by different surgeons at the same institute with similar surgical procedures.
All patients underwent surgery under general or local anesthesia, depending on their age and pain tolerance. A spindle-shaped incision was made around the sinus opening, and methylene blue was injected into the sinus using a probe. Subsequently, en bloc excision of the sinus with the surrounding tissue was performed medial to the temporalis fascia and posterior to the ascending helix. Any branches discovered intraoperatively were tracked and completely resected. The sinus and its branches were dissected from the attached portion of the ascending helix cartilage or perichondrium. After achieving hemostasis, the wound was closed using interrupted sutures without any dead space (Figure 1). In revision cases, subcutaneous necrotic tissue was removed leaving the overlying skin intact. The infected skin recovered after the infection was controlled (Figure 2).
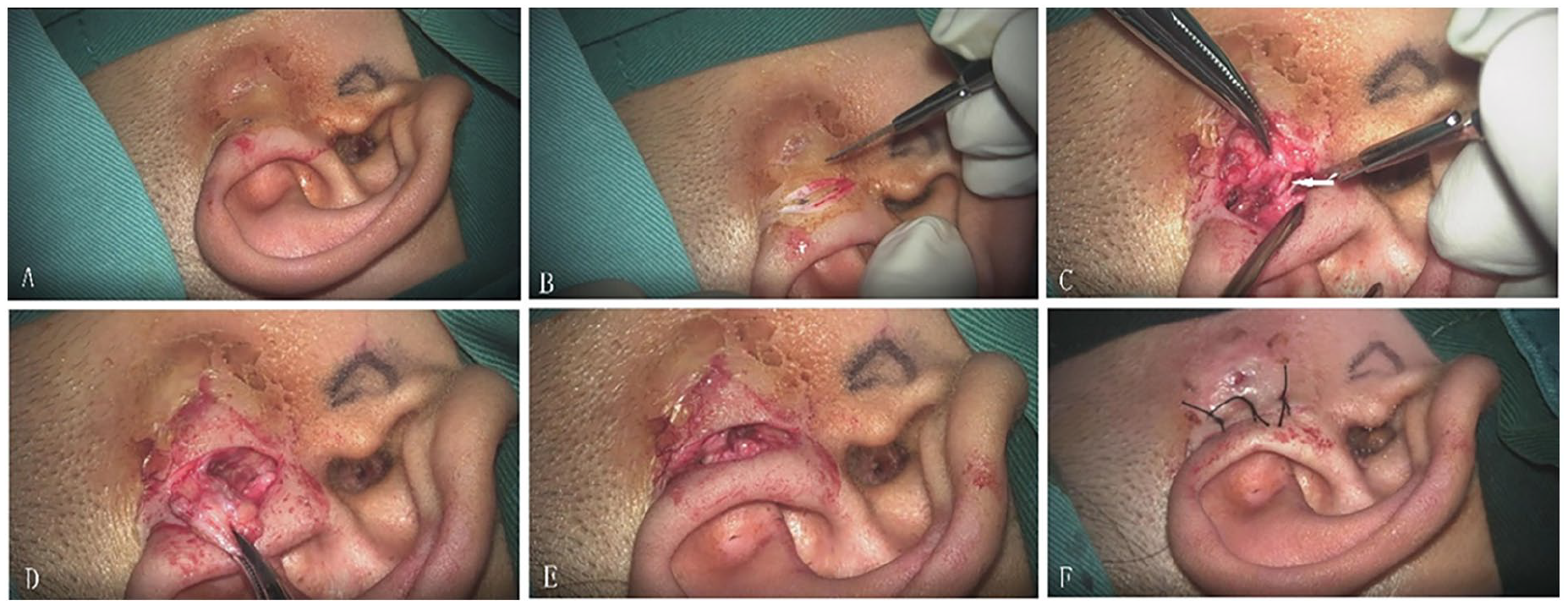
Surgery procedures. The white arrow indicates the cartilage of the ascending helix.
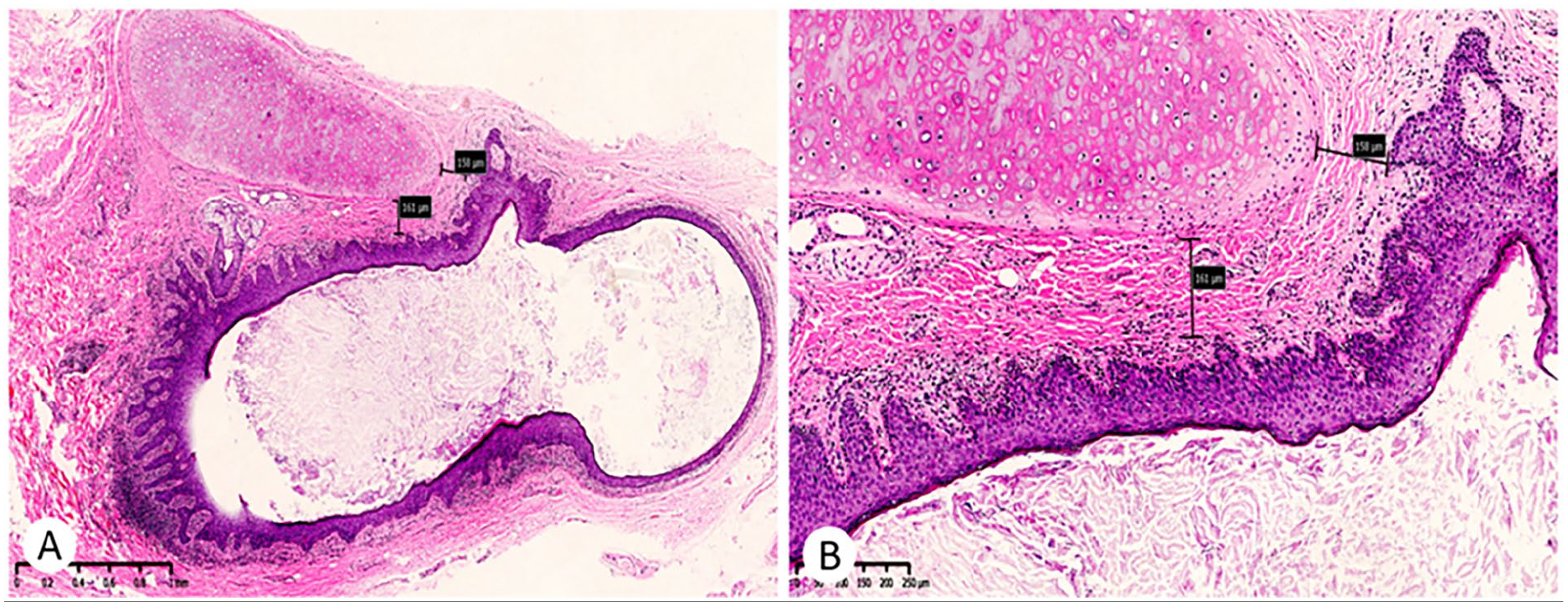
Pathological findings in the primary cases. (A) The sinus tract lined by thick squamous epithelium and a cartilage fragment adjacent to the sinus tract. Mild-moderate lymphocyte infiltration was detected in the sinus tract. (B) The closest distance between the squamous tract and the excised auricular cartilage was 0.16 mm. (A) and (B) Hematoxylin-eosin. (A) magnification ×30 and (B) magnification ×100.
The excised tissue was stained using hematoxylin and eosin, and pathological features, including the shortest distance between the squamous tract and excised auricular cartilage; maximum diameter of the sinus tract; and the presence of infection, cysts, granulation tissue, and multinucleated giant cells were evaluated (Figures 3 and 4).
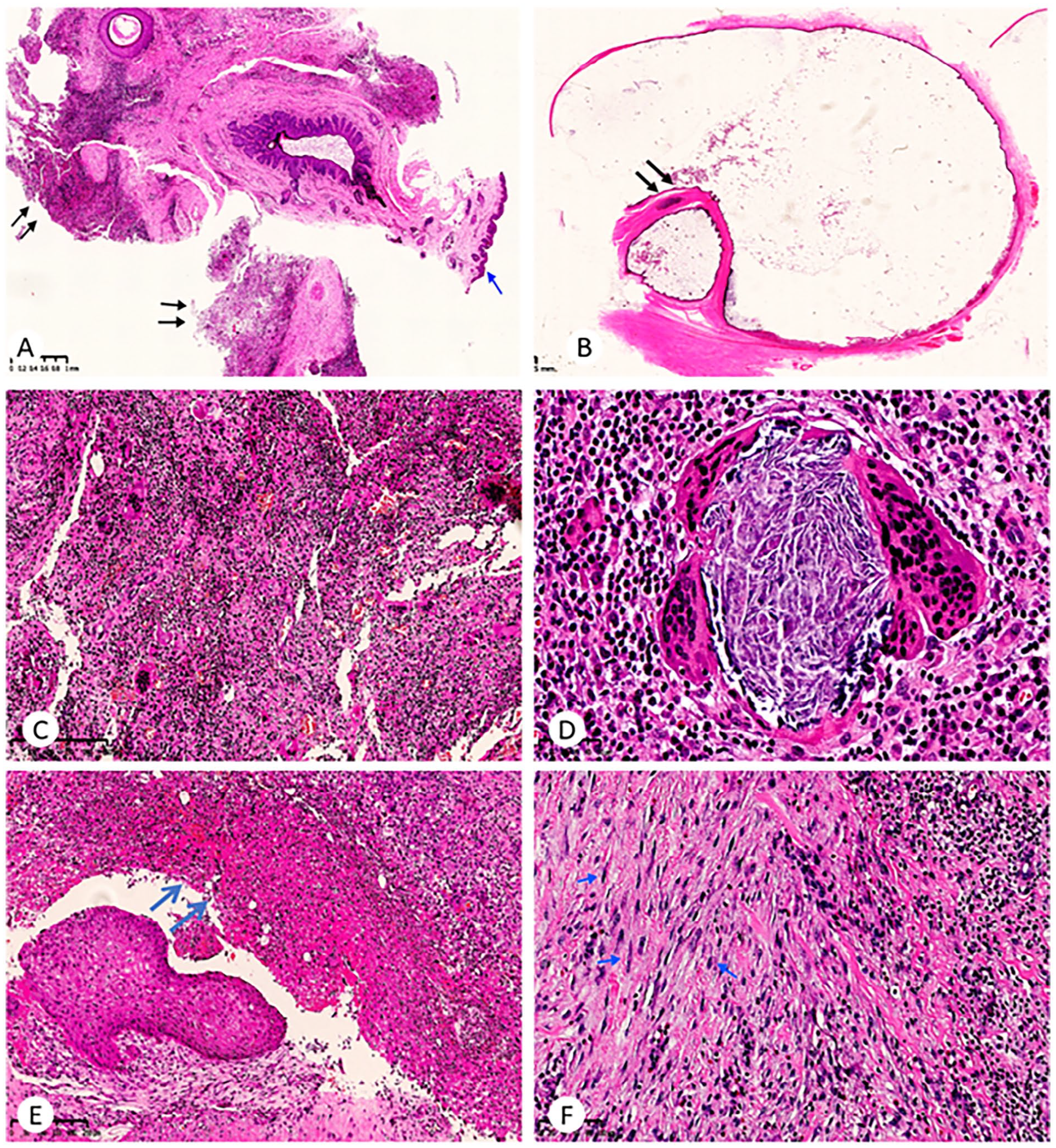
Significant secondary response was observed in the recurrent specimens. (A) On the surface, normal skin can be seen (blue arrow), and a large number of lymphocyte infiltration, granulation tissue proliferation, and multinucleated giant cell reactions could be seen adjacent to the sinus tract (black arrow). (B) A dilated cyst lined by thin squamous epithelium and a cartilage fragment adjacent to the sinus tract (arrow). (C) Granulation tissue and multinucleated giant cell reaction. (D) Acellular keratin was surrounded by foreign body-type giant cells. (E) Necrosis on the surface of granulation tissue (arrow). (F) Myofibroblastic proliferation (arrow). Hematoxylin-eosin. (A) magnification ×20, (B) magnification ×4, (C) magnification ×120, (D) magnification ×400, (E) magnification ×100, and (F) magnification ×200.
A follow-up picture of a recurrent case 2 years after surgery.
All patients were followed up for at least 1 year, and no recurrence was observed.
Results
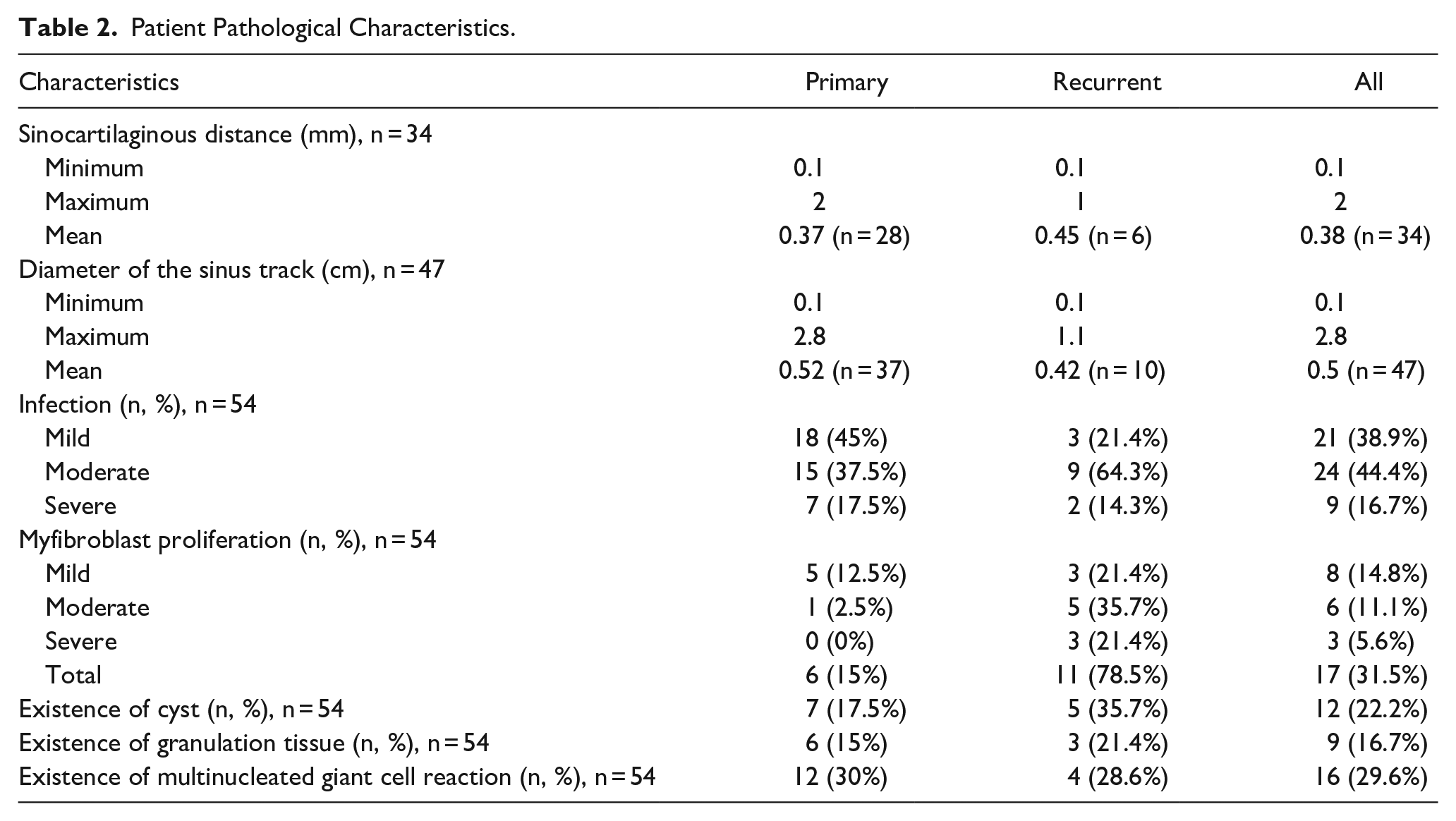
A total of 54 patients [25 male, 29 female; age, 1-58 years (mean, 21 years)] underwent preauricular sinus surgery during the study period. Of these, 40 and 14 underwent primary and revision surgery, respectively (Table 1). Among patients undergoing primary surgery, the shortest distance between the squamous tract and excised auricular cartilage could be determined in 28 cases, and it ranged from 0.1 mm to 2 mm (mean, 0.37 mm). Among patients undergoing recurrent surgery, the distance could be determined in 6 cases, and it ranged from 0.1 mm to 1 mm (mean, 0.45 mm). The mean distance in overall cohort was 0.38 mm.
Patient Characteristics (n = 54).
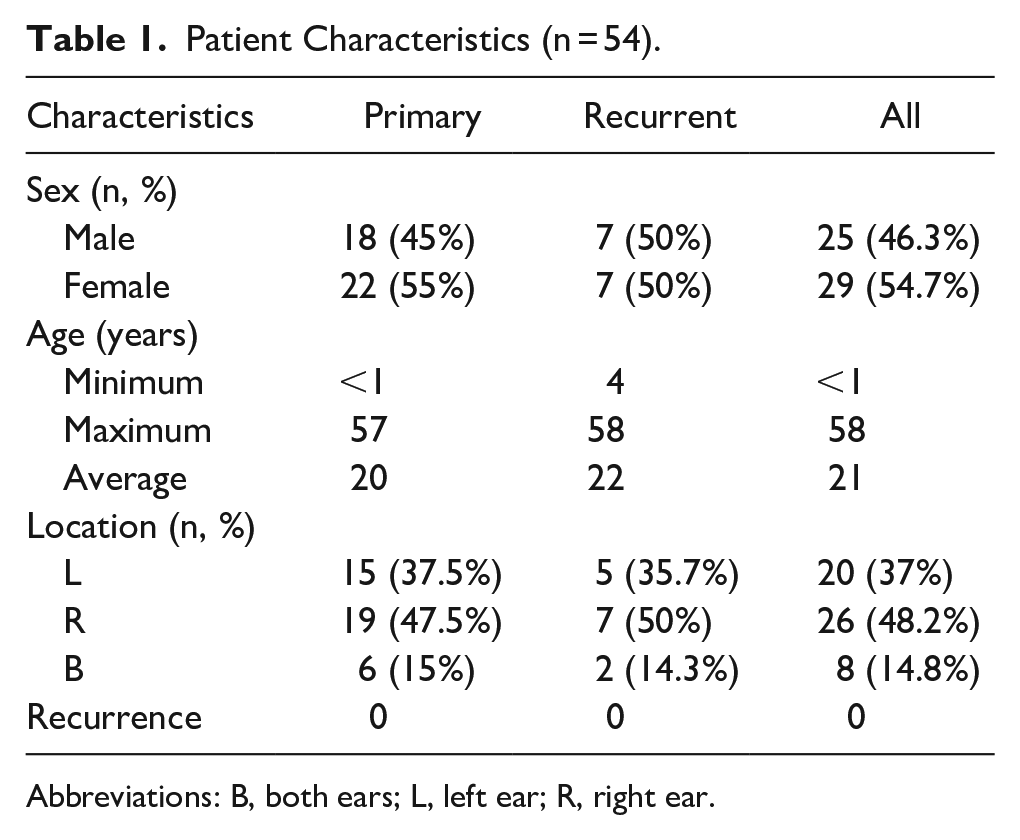
Abbreviations: B, both ears; L, left ear; R, right ear.
The maximum diameter of the sinus track could be determined in 37 and 10 cases in primary and recurrent groups, respectively. The maximum diameter in the 2 groups was 0.52 cm (0.1-2.8 cm) and 0.42 cm (0.1-1.1 cm), respectively. The mean diameter in the overall cohort was 0.5 cm.
The frequency of mild, moderate, and severe infections in primary and recurrent groups was 45%, 37.5%, and 17.5% and 21.4%, 64.3%, and 14.3%, respectively. Myofibroblast proliferation was more frequent in the recurrent group than in the primary group. Myofibroblast proliferation was observed in 6 (15%), 11 (78.5%), and 17 (31.5%) cases in the primary, recurrent, and overall groups, respectively. Cysts were observed in 12 patients, 7 (17.5%), and 5 (35.7%) were primary and recurrent cases, respectively. Granulation tissue was observed in 6 (15%), 3 (21.4%), and 9 (16.7%) cases in the primary, recurrent, and overall groups, respectively. Multinucleated giant cells were observed in 12 (30%), 4 (28.6%), and 16 (29.6%) cases in the primary, recurrent, and overall groups, respectively (Table 2).
Patient Pathological Characteristics.
Discussion
Preauricular sinus is a common congenital ear condition characterized by a small hole or pit in front of the ear. It can occur as an isolated anomaly or as a part of inherited conditions, such as Melnik-Fraser (Branchiootorenal), Beckwith-Wiedemann, and Lachiewicz-Sibley syndromes. 2 The incidence of preauricular sinus varies across different ethnic groups and regions. In Caucasian populations, the incidence is approximately 0.1% to 0.9%, 3 whereas in African and East Asian populations, it is approximately 4% and 10%, respectively. 4 Furthermore, the incidence in South Korea and Japan is 1.91% 5 and 2.6%, respectively. This condition is likely caused by incomplete fusion of the 6 auditory hillocks. 6
Surgical treatment is recommended for cases of preauricular sinus with recurrent infections. Various surgical approaches have been described in the literature, with reported recurrence rates ranging from 0% to 42% (mean, 2.2%).7-9 The primary cause of recurrence is incomplete removal of the sinus, and other potential causes include previous excision, use of a probe to delineate the sinus, and operation under local anesthesia. 10 Therefore, infection control prior to surgery, meticulous dissection, good communication with the patient if local anesthesia is used, and complete removal of all epithelial tissue associated with the sinus are crucial for preventing recurrence.
Prasad et al. reported that the supra-auricular approach, which involves removing a small portion of the auricular perichondrium, resulted in a lower recurrence rate of 5% than of 42% for simple sinectomy. 8 Lam et al also reported a similar findings. 7 The distal part of the sinus is often close to the ascending helix cartilage and perichondrium, and complete removal of this part during surgery is the most challenging aspect and key to reducing recurrence rates. Dunham et al reported that the average distance between the squamous tract and excised auricular cartilage (sinocartilaginous distance) was 0.472 mm, suggesting that routine removal of a small portion of auricular cartilage with the sinus tract may yield a more thorough excision and help prevent recurrence. 11 In this study, the average distance between the squamous tract and excised auricular cartilage was 0.38 mm with no significant difference between the primary and recurrent groups. Moreover, a residual squamous sinus tract was observed in 71% of the recurrent cases, suggesting that incomplete excision rather than a relatively-small sinocartilaginous distance causes recurrence. In addition, the frequency of mild and severe infections was significantly higher in recurrent cases than in primary cases. Furthermore, reactive myofibroblast proliferation, which is a secondary postoperative reaction, was observed in most recurrent cases (78.5%). Reactive myofibroblast proliferation may increase the surgical difficulty in recurrent cases, leading to incomplete resection and multiple relapses. In addition, the incidence of cysts, granulation tissue, and giant cell reactions was significantly higher in recurrent cases. This indicates that in recurrent cases, more complex pathological features might have led to incomplete excision in previous surgeries.
In this study, the average distance between the squamous tract and the auricular cartilage was 0.38 mm, with some cases having a distance as small as 0.1 mm. This suggests that complete removal of the squamous tract from the cartilage can be challenging, particularly in cases of inflammation. Moreover, inflammation was more severe in recurrent cases than in primary cases. Therefore, we recommend removal of a small portion of the ascending helix cartilage during surgery to prevent recurrence. Alternatively, the squamous tract should be carefully dissected from the attached cartilage to ensure complete sinus excision. Our study is a single-center study with small sample size and short follow-up. Further studies including multicenter prospective studies, case-control studies, and studies with larger sample sizes and longer follow-up would provide more reliable data for surgical decisions.
Footnotes
Author Contributions
X.W. and H.C. design this research. G.X. analyze the pathological data. Q.H. write this paper.
Consent for Publication
Written informed consent for the publication of anonymized information was obtained from the legally-authorized representatives of all patients.
Data Availability Statement
The datasets used and/or analyzed during the current study are available from the corresponding author (
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Statement
Ethics approval for this case series was obtained from the ethics committee of Wuhan Union Hospital.