
Abstract
Preauricular sinuses are relatively common congenital anomalies of the soft tissues of the ear. By strict definition, when they connect 2 separate spaces, they are referred to as a preauricular fistula. This clinical entity was first described by Heusinger in 1864. Most preauricular sinuses have a small opening located anterior to the root of the helix. In rare cases, they are found posterior to the tragus, near the crus of the helix, and the ear lobule. The latter is the variant type preauricular sinus, also referred to as the “postauricular sinus,” as the sinus tract opens posterior to the auricle. Recurrent infections or persistent discharge may require surgical excision which is ideally performed at a time when there is no inflammation. There are a variety of techniques for excision. Regardless of the surgical approach taken, it is of critical importance to remove the subcutaneous sac completely. We present a very rare case involving the co-occurrence of a preauricular sinus and postauricular sinus in a 33-year-old woman. We report this case with a review of the literature.
Introduction
Congenital preauricular sinus was first described by Heusinger in 1864. It arises from the incomplete fusion and displacement of the sixth hillock which is derived from the first and second branchial arches during embryogenesis. 1 In many cases, there are no symptoms, and no treatment is required. However, surgical intervention becomes necessary when there is recurrent infections or persistent discharge through the sinus. 2
While preauricular sinuses are typically located in the anterior superior part of the ear, they can exist in various areas around the ear. These include the helical crus, posterosuperior aspect of the auricle, preauricular region, retroauricular area, and the area inferior to the external ear structures. Preauricular sinuses can be categorized into 2 types based on their position relative to a line connecting the tragus and the posterior margin of the ascending limb of helix. The first type is referred to as the classical type, in which the opening of the sinus is anterior to this line. The second is the variant type or “postauricular sinus,” which opens posteriorly to the line mentioned above. 3 The variant type is less common than the classical type and is characterized by the direction of the sinus opening toward the posterior aspect, leading to recurrent infections and abscess formation in the retroauricular area.1,4
We present an exceptionally rare occurrence of both classical and variant types of preauricular sinuses in a 33-year-old female patient, and we present this case along with a review of the literature.
Case
A 33-year-old female patient visited the otolaryngology department with complaints of pain and swelling around the right ear that had persisted for a week. She denied hearing loss, tinnitus, vertigo, or other otologic symptoms, and there were no underlying medical conditions. However, she had a history of intermittent ear pain and swelling in the same area for several years. On examination, acute inflammation with swelling and tenderness was observed in the right ear and the surrounding preauricular region (Figure 1A). Acute infections of the ear such as acute auricular perichondritis and relapsing polychondritis were considered and intravenous antibiotic therapy was initiated. A temporal bone computed tomography scan revealed inflammatory changes in the right ear with soft tissue edema and an abscess in the anterior superior preauricular region (Figure 2A and B). Incision and drainage were performed, followed by a 2 week course of intravenous antibiotic therapy, resulting in improvement. The Numeric Rating Scale for ear pain decreased from 8 points at admission to 2 points at discharge. During the recovery period, drainage of fluid from the preauricular sinus, which was not previously observed, was identified. Two openings were identified, one in the crus of helix and the other at the anterior aspect of the root of the helix (Figure 1B and C). Before discharge, the diagnosis of right preauricular sinus was made.
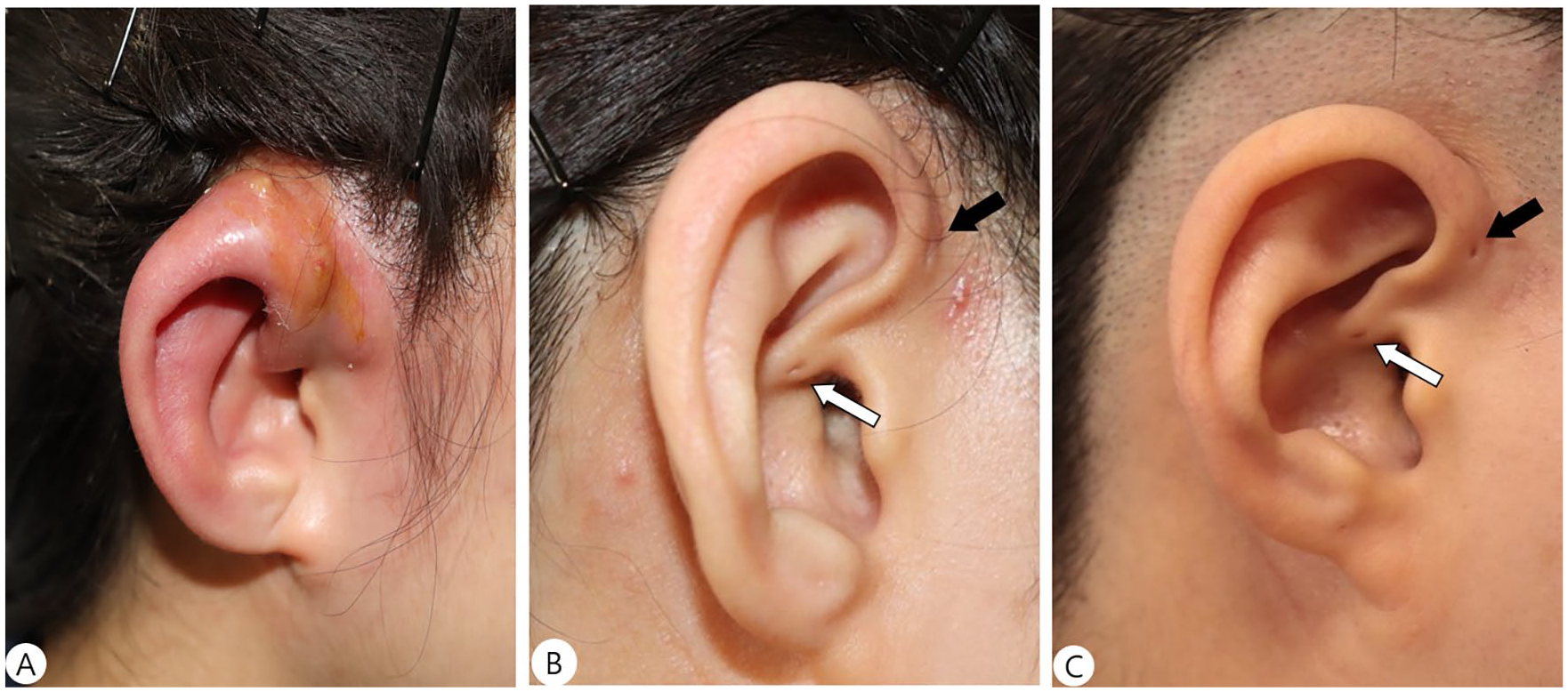
Pictures of the patient’s right ear. (A) Shows edema and swelling of the right auricle with abscess formation. Right auricle before discharge after inflammation resolved (B) and right auricle before surgery (C). Gross photograph of the patient shows 2 auricular pits on right ear. One on the crus of helix (white arrow) and the other on anterior area of root of helix (black arrow).
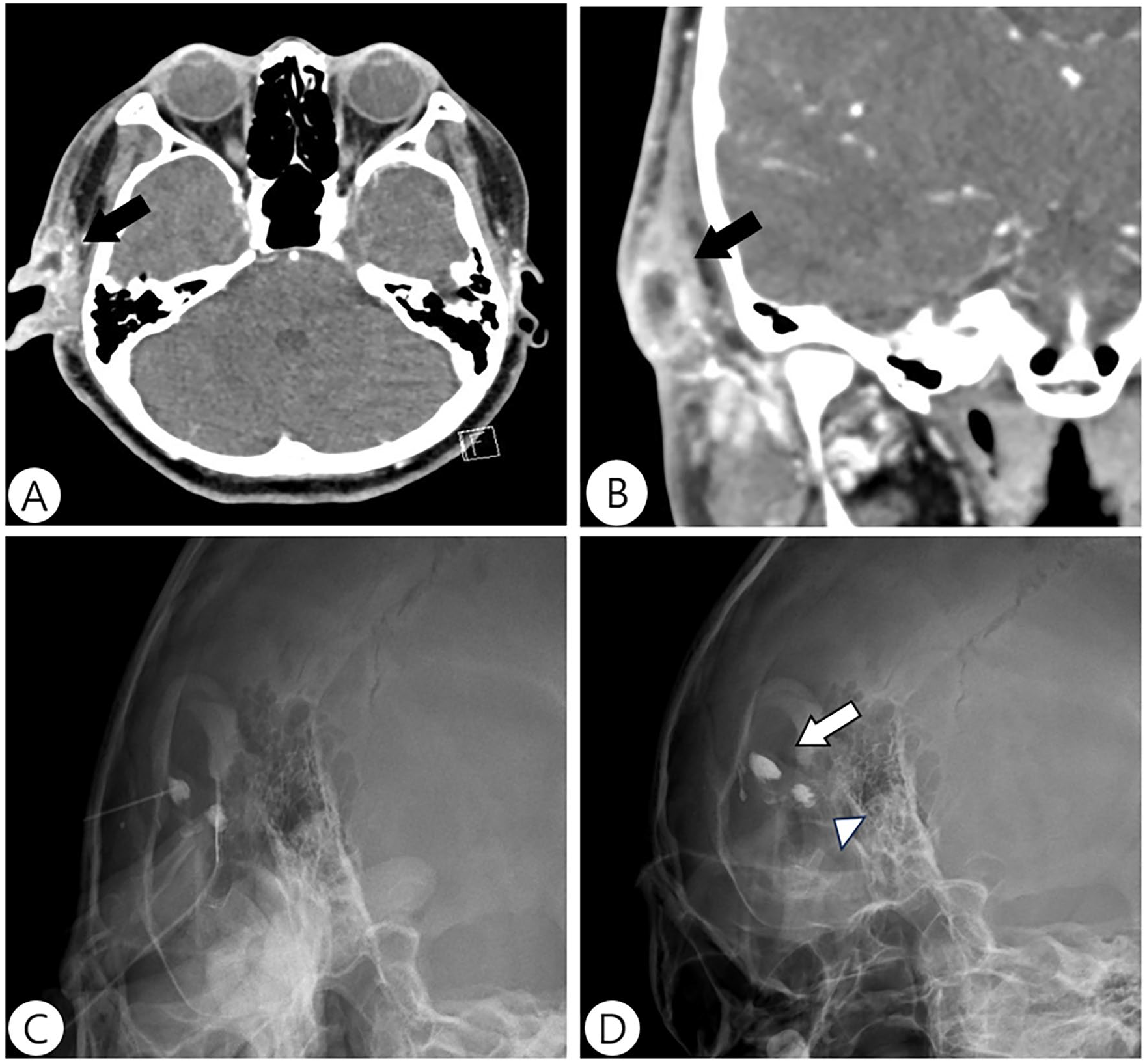
Preoperative imaging. Axial contrast-enhanced temporal bone CT (A) and coronal contrast-enhanced temporal bone CT (B) shows anterosuperior dominant diffuse swelling with abscess in the right auricle and periauricular area (black arrows). Sinusography is performed by injecting iopamidol into the preauricular and postauricular openings through a syringe (C). (D) Shows 0.5 cm × 0.8 cm sinus (white arrowhead) and 0.4 cm × 1.1 cm sinus (white arrow) in right ear. CT, computed tomography.
Surgery was performed 6 months later under general anesthesia, after complete control of the acute inflammation. Preoperative sinusography was performed to evaluate the direction, length, and size of the sinuses. The sinus with the opening in the crus of helix was 0.5 cm × 0.8 cm, and the sinus with the opening at the anterior aspect of the root of helix was 0.4 cm × 1.1 cm (Figure 2C and D). Methylene blue dye was injected into the openings to facilitate visualization during surgery. Surgical excision included complete removal of both sinuses, involving the total margin of the fistular openings. A probe was gently inserted into the fistula at the anterior of the root of helix and advanced to check the direction and width of the lumen until it was dissected up to the periosteum. Finally, the total fistular lumen along with the adjacent auricular cartilage and granulomatous tissue was completely removed. The variant type preauricular sinus at the crux of helix pierced through the cartilage into the posterior ear. The posterior portion of the fistula was adhered to the cartilage, so adjacent cartilage was also removed with the preauricular sinus (Figure 3A and B). Primary closure was performed with drain tube insertion, and pressure dressing was applied. The patient was discharged without complications on the seventh day postsurgery (Figure 3C and D). Histopathological examination revealed a well-encapsulated subcutaneous cyst lined by hyperkeratinized stratified squamous epithelium, with surrounding inflammatory granulation tissue, consistent with a preauricular sinus. At the 12 month follow-up, there was no evidence of recurrence or indications of complications from surgery.
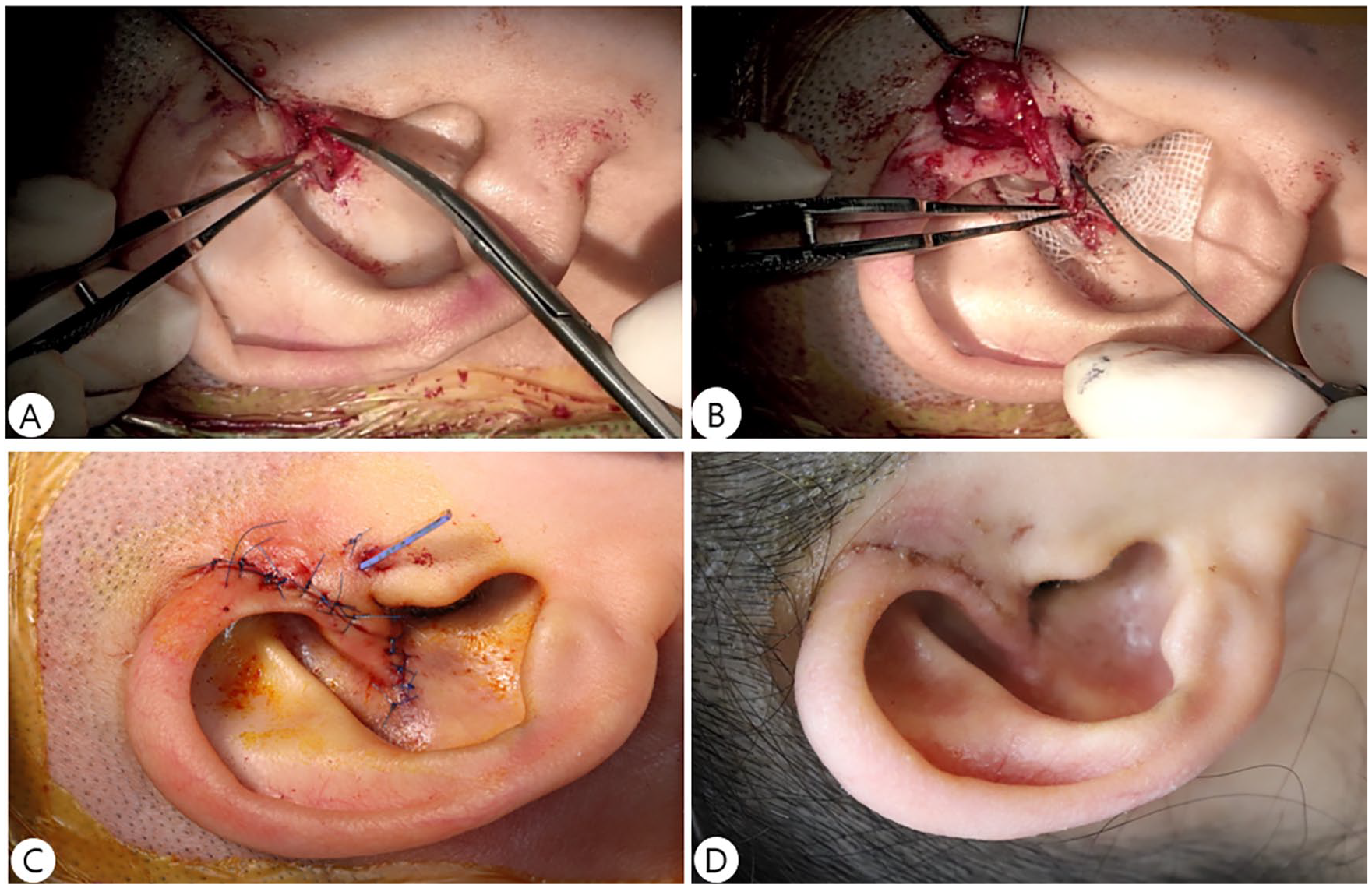
Surgical procedures and postoperative photos. (A) Shows the cartilage surrounding the sinus tract should be excised together to ensure complete removal. (B) Shows sinus tract being dissected by classical sinectomy. (C) Shows right auricle immediately after surgery with primary suture and drainage tube inserted. Right auricle with stitches removed at 7 days postoperatively (D).
Written informed consent was obtained from the patients involved in this study. This report is written in compliance with the Declaration of Helsinki.
Discussion
The preauricular sinus can occur sporadically or hereditarily. In the case of hereditary occurrence, it manifests as an incomplete autosomal dominant genetic expression with various phenotypic presentations. 5 The preauricular sinus is formed by the 6 preauricular hillocks originating from the first and second branchial arches around the sixth week of gestation. Congenital preauricular sinuses are known to occur when these hillocks fail to fuse completely or migrate inadequately during embryonic development.1,6 Incidence ranges from 0.1% to 9% in the United States, showing no significant difference in gender, but varies according to race, with reported rates in Asia and parts of Africa ranging from approximately 4.0% to 10%. 4
The classification of preauricular sinuses is based on their position relative to a line connecting the tragus and the posterior margin of the ascending limb of helix. The classical type opens anterior to this line, and the variant type, also known as “postauricular sinus,” opens posterior to this line. 3 The classical type’s opening faces the anterior part of the external auditory canal, while the variant type may face either the posterior-central or posterior-inferior aspect of the canal. 3 Furthermore, variant type sinuses can be classified into 3 subtypes based on the opening’s location: type 1 in the middle of the crus helix, type 2 superior to the crus helix, and type 3 at the cymba concha. 3 Overall, the incidence rate of postauricular sinuses is low.1,4 However, the simultaneous occurrence of both classical and variant types on one side, as observed in this case, is extremely rare. Our patient had a combination of the classical type and variant type 1, with the fistula opening found in the middle of the crus of helix, as well as a posterior fistular tract.
Clinical manifestations of congenital preauricular sinus are mostly asymptomatic, but occasional symptoms such as swelling, abscess formation, tenderness, and discharge may occur due to inflammation of the subcutaneous cyst caused by desquamation or infection. In such cases, appropriate antibiotic treatment is required, along with incision and drainage in case of abscess formation. 5 The classical type primarily presents with abscesses and discharge around the preauricular region, while the variant type shows inflammation around the auricle or retroauricular region. 1 Surgical excision is recommended during inflammation-free periods, for cases with recurrent infections or persistent discharge. 6 However, complete removal is challenging due to the branching pattern of the sinus.5,7 This results in a relatively high recurrence rate, especially in the variant type with intricate pathways and dense surrounding tissue. 4 Therefore, preoperative sinusography, delineating the sinus with injection of methylene blue, and blunt probing during surgical excision can aid in complete removal.2,4 Surgical techniques are simple sinus excision and the supra-auricular approach where the incision is extended posteriorly and superiorly in the temporal direction. 5 Variant type sinuses are generally removed using a bidirectional approach, which accesses the anterior and posterior auricle simultaneously.3,4 In this case, the classical type preauricular sinus was removed with the classical sinectomy approach by making an elliptical incision at the margin of the sinus oriface and dissecting along the sinus tract. The variant type postauricular sinus was relatively narrow, necessitating concurrent removal of part of the cartilage surrounding the sinus tract. Removal of the helical crus cartilage can result in auricular deformity, so we minimized extent of the dissection in this area.
Conclusion
The authors performed successful surgical excision of the preauricular and postauricular sinuses simultaneously in an ear, while achieving good results without recurrence, complications, or ear deformities. Unlike the more common typical preauricular sinus, the rarer variant type must be differentiated with symptomatic lymphadenitis, epidermal cysts, sebaceous cysts, and branchial cleft anomalies around the retroauricular area.4,5 Accurate diagnosis and total surgical removal may be challenging due to the diverse locations of the sinus openings and trajectories of their tracts. In addition, careful consideration of surgical methods is essential, considering the branching pattern of the sinuses, especially in cases with recurrent infections and adhesions to surrounding tissues.
Footnotes
Acknowledgements
Not applicable.
Data Availability
Data sharing not applicable to this article as no datasets were generated or analyzed during the current study.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Statement
All procedures performed in this study involving human participants were in accordance with the ethical standards of the institutional review board. Our institution does not require ethical approval for reporting individual cases or case series.
Informed Consent/Patient Consent
Informed consent was obtained from the patient for the publication of this case report.
Trial Registration Number/Date
Not applicable.
Grant Number
Not applicable.