
Abstract
Keywords
Introduction
Obstructive sleep apnea-hypopnea syndrome (OSAHS) is a highly prevalent breathing disorder in sleep and is associated with various diseases, such as dyslipidemia, sudden cardiac death, hypertension, and diabetes.1-3 Treatment strategies for OSAHS patients need comprehensive approaches. Continuous positive pressure ventilation (CPAP) is accepted as the first choice for OSAHS patients, but patients with upper airway anatomical abnormalities need more surgical intervention. 4
Modified uvulopalatopharyngoplasty (mUPPP) has been proven to be a useful option for the treatment of OSAHS. 5 But mUPPP alone addresses only velopharyngeal airway collapse and is suboptimal in the treatment of moderate to severe OSAHS which is widely accepted as a multilevel airway disease. 6 The frequent multilevel diseases including oropharyngeal and nasal obstruction. 7 Nasal obstruction is mainly caused by either nasal or septal deformities, as well as mucosal disease associated with inferior turbinate hypertrophy which is considered the most common cause of nasal obstruction. 8 Surgical reduction of the inferior turbinate is warranted to relieve the nasal obstruction caused by hypertrophied inferior turbinates. Radiofrequency coblation inferior turbinoplasty can effectively increase the nasal airway passage and avoid complications of conventional turbinectomy such as bleeding, crusting, and excessive pain. 9 Due to the risk of airways in OSAHS operations, radiofrequency coblation inferior turbinoplasty is more suitable for OSAHS patients with nasal obstruction caused by inferior turbinate hypertrophy. For OSAHS patients who have inferior turbinate hypertrophy and oropharyngeal obstruction, the authors’ experience has been that mUPPP with radiofrequency coblation inferior turbinoplasty is more effective than standalone mUPPP. Given a lack of direct comparisons between mUPPP with radiofrequency coblation inferior turbinoplasty and standalone mUPPP, the aim of this study was to evaluate the surgical outcomes and potential complications between these 2 methods and determine whether mUPPP with radiofrequency coblation inferior turbinoplasty offers more advantages in OSAHS patients.
Materials and Methods
Study Design
A retrospective analysis of 79 OSAHS patients with inferior turbinate hypertrophy and oropharyngeal obstruction who underwent surgical treatment was performed. All patients (age >18) were consecutively selected from the Department of Otolaryngology and Head and Neck Surgery at the Qingdao Municipal Hospital during a 2.3-year period (January 2020–April 2022). According to the different surgical methods, patients were divided into 2 groups (Group A and Group B). Group A included 36 patients treated with standalone mUPPP. Group B included 43 patients treated with mUPPP and bilateral radiofrequency coblation inferior turbinoplasty. This study was approved by the local ethics committee of the Qingdao Municipal Hospital (2024-LW-071) and was carried out according to the Declaration of Helsinki of the World Medical Association. All procedures in this study abide by the standards of the institutional and national ethics committee. Written informed consents were obtained from all the participants for their anonymized information to be published in this article.
Patient Inclusion Criteria
(1) Patients were diagnosed with moderate or severe OSAHS according to polysomnography (PSG). (2) Patients with nasal and oropharyngeal obstruction were selected based on flexible nasopharyngolaryngoscopy (a comprehensive examination of the nasal cavity, nasopharynx, oropharynx, and larynx). All patients with nasal obstruction were caused by bilateral inferior turbinate hypertrophy, excluding other diseases such as nasal deformity, nasal septum deviation, or nasal cavity occupation. (3) Patients who had failed CPAP treatment. (4) Patients with no history of surgery in the nasal or oropharyngeal cavity. (5) Patients who gave their consent to participate in this study.
Surgical Methods
The surgical methods included 2 parts: mUPPP and bilateral radiofrequency coblation inferior turbinoplasty. All surgical procedures were performed by the same senior surgeons.
Modified uvulopalatopharyngoplasty
First, the tonsils were removed. Then 2 inverted “V”-shaped incisions were made on both sides of the soft palate. Redundant adipose tissues around the levator palatini and tensor palatini were excised (the intact uvularis were preserved). The palatoglossal arch and the palatopharyngeal arch were sutured to stabilize and enlarge the oropharyngeal cavity space. The dorsal and ventral edges of the preserved mucosal membrane of the uvula were closed with interrupted sutures. Corticosteroids such as dexamethasone or methylprednisolone were administered during surgery and a brief course of corticosteroids was needed in the initial stages of the postoperative period.
Bilateral radiofrequency coblation inferior turbinoplasty
This operation was performed by using the Coblator II surgical system and a fine-tipped wand set at power level 4. Before the operation, a vasoconstrictor (1/1000 adrenaline) was used to contract the bilateral nasal mucosa. The tip of the wand was introduced into the anterior part of the bilateral inferior turbinates to create a horizontal channel from anterior to posterior. The wand was advanced along the length of the turbinate submucosally. Depending on the bulk of the turbinate, these steps could be repeated by creating an additional channel. After surgery, we applied smaller volume fillers to pack the anterior segment of the patient’s nasal cavity to control bleeding in the anterior head of the inferior turbinate, and all the nasal packing materials were removed in 24 hours (Figure 1).
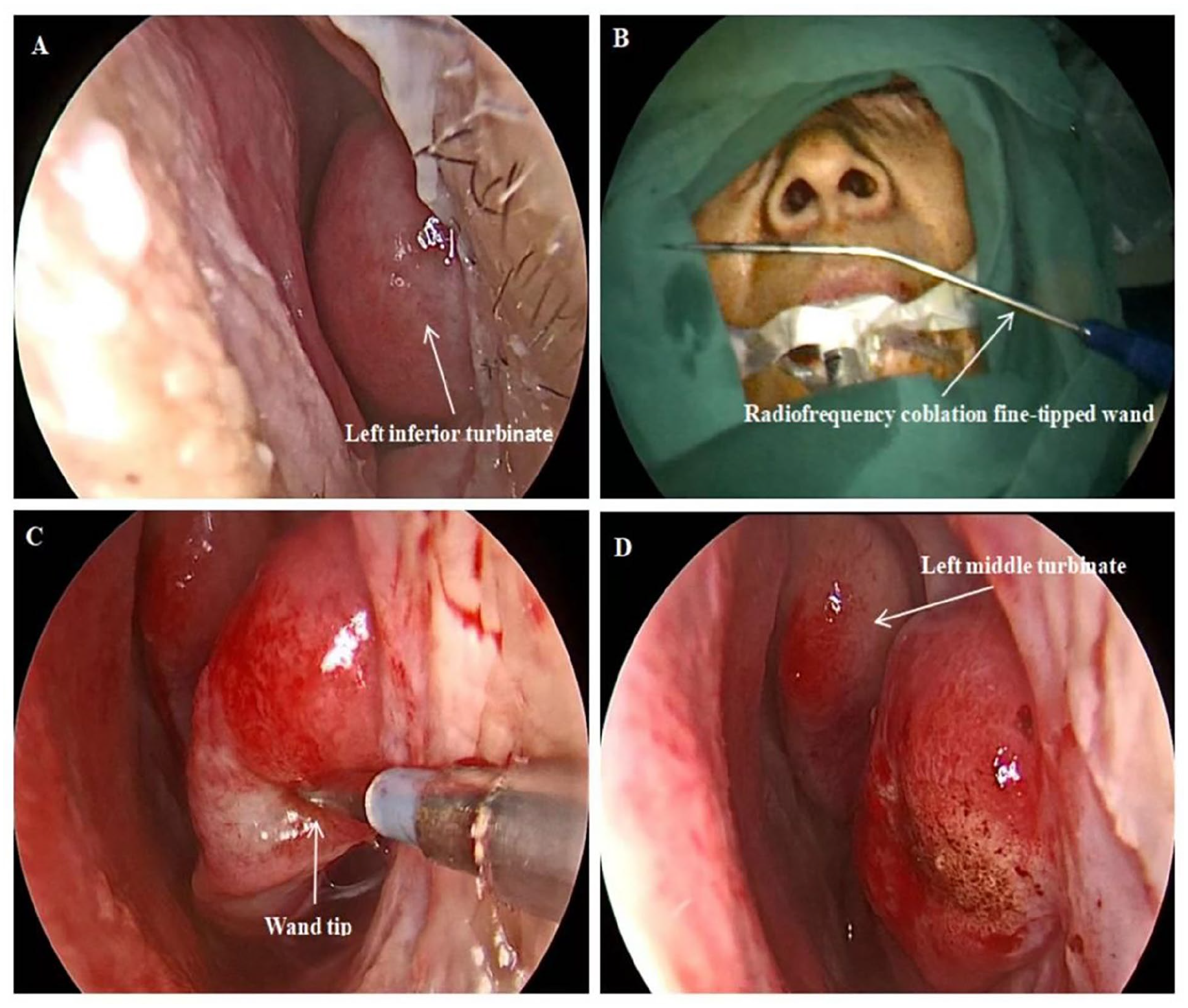
Bilateral radiofrequency coblation inferior turbinoplasty technique. (A) Preoperative. (B) The radiofrequency coblation equipment is activated. (C) The tip of the wand is introduced into the anterior part of the inferior turbinate to create a horizontal channel from anterior to posterior. (D) Postoperative.
Outcome Data
The evaluation criteria for inferior turbinate hypertrophy were based on Camacho’s study, which classified the inferior turbinate size as 4 grades (grades 1–4). 10 When the inferior turbinate occupies 0% to 25% of the total nasal airway space (under nasoendoscopic assessment), it is grade 1, grade 2 is 26% to 50%, grade 3 is 51% to 75%, and grade 4 is 76% to 100%. In our study, when the size of the inferior turbinate exceeded grade 2, we believed that the inferior turbinate was hypertrophy. The sum of the bilateral inferior turbinate size grades (total inferior turbinate size grade) was obtained as evaluation data.
The evaluation of oropharyngeal obstruction was based on the Friedman tongue position (FTP) grade and the Friedman tonsil size grade, which were considered classic indicators of OSAHS, while effectively informing surgical selection. Many studies have identified a strong association between increased OSAHS severity and increased scores in the FTP/tonsil size classifications.11,12 When the patient’s FTP grade and tonsil size grade both exceeded 1 (grades 2-4), we believed that the patient had oropharyngeal obstruction.
All patients underwent an active anterior rhinomanometry (AAR) test to evaluate nasal patency. According to the standard guidance of AAR, 13 the average values of total nasal resistance (TNR) were measured as evaluation data using a rhinomanometer (NR6, GM Instruments Ltd, Scotland, UK) with a standard pressure of 150 Pa in this study. The AARs were performed after at least 5 minutes of sitting rest. We ensured that all subjects reached the measurements from quiet activities. TNRs without nasal decongestion were collected to assess the actual nasal resistance in all OSAHS patients. AAR with pharmacological (oxymetazoline nasal drops) decongestion was performed on a patient who underwent turbinoplasty to predict the surgical outcomes. All measurements were carried out by the same surgeon and were performed in the same room, with the same equipment, and at normal room temperature.
All patients underwent an overnight polysomnographic evaluation with a PSG device (Alice PDx, Philips Respironics, PA, USA). PSG tests were performed by the same sleep technician according to the standard criteria of the American Academy of Sleep Medicine manual. The data recorded for evaluation included: AHI and the lowest O2 saturation (LSaO2).
The patient’s age, neck circumference, body mass index (BMI), FTP grade, tonsil size grade, Epworth sleepiness scale (ESS) score, total inferior turbinate size grade, TNR (without nasal decongestion), AHI, and LSaO2 were recorded on the day before surgery.
Successful Surgical Result
The successful surgical result was defined as a 50% or greater decrease in AHI in postoperative PSG.
Follow-Up
This study established a standard follow-up system after the operation, surgeons were responsible for the summary and registration of the follow-up data. Postoperative follow-up lasted 6 months, PSG and AAR (without nasal decongestion) tests were performed in the 6th month after surgery.
Statistical Analysis
Statistical process SPSS 22.0 statistical software (SPSS Inc, Chicago, IL, USA) was used for the analysis. Categorical variables are presented as percentages (%) and continuous variables are presented as mean ± standard deviation values. Age, neck circumference, BMI, FTP grade, tonsil size grade, ESS score, total inferior turbinate size grade, TNR, AHI, and LSaO2 in 2 groups were obtained and analyzed using the t test. The gender composition, surgical success rate, and total surgical complication rate were analyzed using the Chi-square test. Differences were considered statistically significant when the P value was <.05.
Results
In this study, 79 patients (65 males and 14 females) with moderate to severe OSAHS were selected. According to the OSAHS classification standard, there were 31 patients with moderate OSAHS and 48 patients with severe OSAHS. Before surgery, there were no significant differences in age, gender, neck circumference, BMI, FTP grade, tonsil size grade, ESS score, total inferior turbinate size grade, TNR, AHI, and LSaO2 between the 2 groups. Table 1 presents the characteristics of the patients.
Characteristics in 2 Groups. a

Abbreviations: AHI, apnea-hypopnea index; BMI, body mass index; ESS, Epworth sleepiness scale; FTP, Friedman tongue position; LSaO2, the lowest O2 saturation; Pre-, preoperative; TNR, total nasal resistance; UPPP, uvulopalatopharyngoplasty.
n = 79.
n = 36.
n = 43.
t test.
Chi-square test.
The surgical results of this study are detailed in Table 2. After 6 months of surgery, AHI, LSaO2, and TNR in Group B showed a significant improvement compared to Group A. The comparison of surgical success rates between the 2 groups is detailed in Table 3. There were 33 (76.74%) successful patients in Group B with 10 failed patients, compared to 19 (52.78%) successful patients in Group A with 17 failed patients, with a significant statistical difference between 2 groups (P = .025).
Comparison of the Surgical Outcomes Between 2 Groups. a
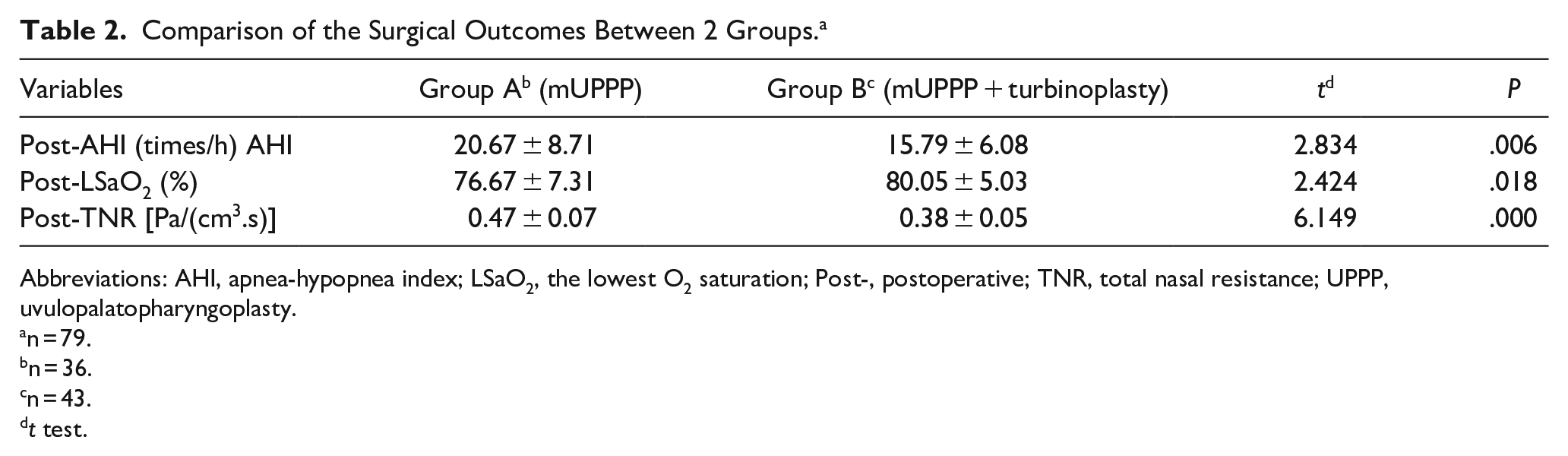
Abbreviations: AHI, apnea-hypopnea index; LSaO2, the lowest O2 saturation; Post-, postoperative; TNR, total nasal resistance; UPPP, uvulopalatopharyngoplasty.
n = 79.
n = 36.
n = 43.
t test.
Comparison of the Surgical Success Rate Between 2 Groups. a
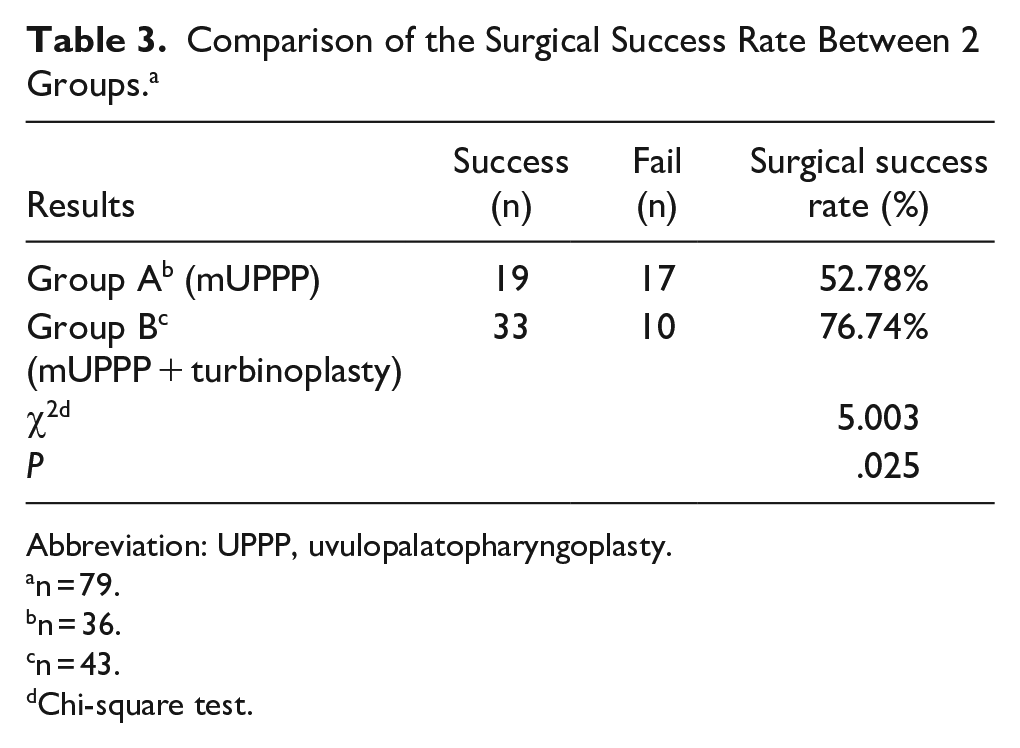
Abbreviation: UPPP, uvulopalatopharyngoplasty.
n = 79.
n = 36.
n = 43.
Chi-square test.
Five patients in Group A and 10 patients in Group B experienced procedure-related complications. In Group A, 2 patients experienced oropharyngeal bleeding, 2 patients experienced postoperative infection, and 1 patient experienced nasal regurgitation. Patients in Group A did not experience any complications in the nasal cavities. In Group B, 1 patient experienced nasal adhesion, 3 patients experienced nasal bleeding, 1 patient experienced oropharyngeal bleeding, 3 patients experienced postoperative infection and 2 patients experienced nasal regurgitation. There was no significant difference in the total surgical complication rate between the 2 groups (13.89% vs 23.26%, P = .290). No serious complications such as asphyxia or shock occurred after surgery. All recurrent patients in the 2 groups did not wish to undergo additional surgery and resumed use of CPAP. Table 4 presents the surgical complications of the patients.
Comparison of the Surgical Complication Between 2 Groups. a

Abbreviation: UPPP, uvulopalatopharyngoplasty.
n = 79.
n = 36.
n = 43.
Differences in summation complications of 2 groups were assessed using the Chi-square test.
Discussion
OSAHS and its surgical management have been constantly evolving and vastly studied, especially for the oropharyngeal obstruction. Ikematsu 14 first introduced palatal surgery in 1964 to treat snoring and then Fujita et al 15 introduced UPPP in 1981 to treat OSAHS in adults. To reduce the discomfort caused by palatine uvula deficiency, modified UPPP has been updated by many scholars. Mantovani et al 16 proposed in 2012 a new surgical technique, barbed reposition pharyngoplasty (BRP), which laterally and anteriorly displaces the posterior pillar to enlarge the oropharyngeal inlet and the retropalatal space. BRP has proven to be an easy-to-learn, quick, and effective new palatopharyngeal procedure. 17 While mUPPP has been recognized as a commonly employed surgery for resolving airway obstructions in the oropharynx, the surgical treatment of patients with moderate to severe OSAHS remains one of the difficulties in the Department of Otolaryngology. Multiple methods have been used to assess the airway and assist in selecting OSAHS surgical techniques. Methods include a general clinical exam, flexible endoscopy, drug-induced sleep endoscopy (DISE), and radiologic studies. No method is uniformly accepted and each may contribute useful information. It has become increasingly clear that the surgical treatment of OSAHS needs multilevel surgery. Nasal patency is also a pivotal factor in the outcome of OSAHS surgery. A narrowed nasal cavity is thought to contribute to OSAHS by increasing the airflow velocity, which, in accordance with Bernoulli’s law, can lead to increased pharyngeal collapse during sleep. Fitzpatrick et al 18 demonstrated that when a nasal obstruction exists, oral breathing is favored, resulting in a narrowed oropharyngeal space and more frequent apnea episodes, this clearly shows that standalone pharyngoplasty for OSAHS is not enough. In particular, DISE has shown that the nasal cavity and soft palate are important anatomic components of obstruction in OSAHS, therefore, many surgeons advocate surgical treatment for nasal obstruction as a modality to improve the severity of OSAHS. 19
Inferior turbinate hypertrophy is considered the most common cause of nasal obstruction. 8 Leitzen et al 20 researched the correlation between nasal anatomy and OSAHS severity, the results confirmed that inferior turbinate hypertrophy was the main factor causing nasal obstruction in OSAHS patients. When managing OSAHS patients with inferior turbinate hypertrophy and oropharyngeal obstruction, the combination of inferior turbinate turbinoplasty and mUPPP seems logical in that they aim to achieve the same goal of a more open upper airway. Due to the risk of airways in OSAHS operations, the preferred method for treating inferior turbinate hypertrophy in OSAHS patients is a more mucosal-friendly turbinoplasty procedure. More and more scholars are supporting that radiofrequency coblation inferior turbinoplasty as a minimally invasive method for treating inferior turbinate hypertrophy. 9 Radiofrequency coblation can reduce the inferior turbinate by vaporizing and destroying the soft erectile tissue, the volume reduction and tissue fibrosis in turbinate are immediate and sustainable. Lee et al 21 conducted a study to determine the efficacy of radiofrequency coblation inferior turbinoplasty in patients with persistent inferior turbinate hypertrophy. This study showed that both subjective and objective outcomes regarding nasal obstruction in radiofrequency coblation turbinoplasty were better than conventional turbinoplasty and with minimal complications. In our study, patients who underwent turbinoplasty had a significant decrease in TNR (without nasal decongestion) compared to patients with standalone mUPPP (t = 6.149; P < .05). This outcome indicated that bilateral radiofrequency coblation inferior turbinoplasty was effective in relieving the nasal obstruction, it is also consistent with some previous research.
Based on the above studies, we speculate that radiofrequency coblation inferior turbinoplasty may improve the severity of OSAHS patients who have inferior turbinate hypertrophy. However, research examining the surgical effectiveness of pharyngoplasty combined with bilateral radiofrequency coblation turbinoplasty for OSAHS is limited, especially lack of the comparison of objective outcomes between the combined surgery and standalone pharyngoplasty. Our study was carried out to determine the efficacy of the combined surgery for OSAHS patients with nasal and oropharyngeal obstruction. We chose the multilevel single-stage approach to avoid the decreased efficacy, increased morbidity, and increased economic burden posed by multiple-stage procedures. However, concern for increased complications from the combined effects of pharyngeal edema, nasal packing, loss of the airway, exacerbation of apnea, and increased sedation has led some authors to argue against single-stage surgery. 22 Recent publications have reported that the lower surgical complications are attributed to a more diligent approach in reducing soft tissue edema and preventing the overuse of sedatives. 23 In our study, surgical complications in OSAHS patients mainly included nasal adhesion, bleeding, infection, and nasal regurgitation. Although patients who underwent turbinoplasty experienced 3 cases of nasal bleeding and 1 case of nasal adhesion, there was no significant difference in the total surgical complication rate between the 2 groups (13.89% vs 23.26%, P = .290). It meant that the single-stage multilevel airway surgery performed in our study did not significantly increase the postoperative complications. No serious complications such as asphyxia or shock occurred in our study and all complications in the patients were cured after treatment and did not develop into permanent damage.
Long-term follow-up of surgical treatment for OSAHS demonstrates that the efficacy of mUPPP may decrease over time, the success rate after 6 months of surgery is approximately 50% to 60%.24,25 The surgical success rate of standalone mUPPP in our study was 52.78%, which was consistent with previous studies. Although BRP can slightly improve surgical efficacy, some studies have confirmed that the rate of postoperative tonsillar bleeding after BRP is higher than mUPPP. 26 Therefore, we did not choose BRP as the surgical method for pharyngoplasty to reduce the occurrence of postoperative oropharyngeal bleeding. Reasons for the failure of mUPPP include not sufficiently managing the areas of airway collapsibility and narrowing. Measurement of the pharyngeal cross-sectional area, airway manometry, and endoscopy have provided verification for the explanations for mUPPP failure. Surgery failures may be redeemed by surgical procedures that alter sites of the upper airway that are not modified by mUPPP. Therefore, procedures that expand the nasal airway may rescue a failed mUPPP. The treatment effect on PSG indicators demonstrated in our study showed that both AHI and LSaO2 after surgery in the combined surgery (radiofrequency coblation inferior turbinoplasty with mUPPP) group were better than standalone mUPPP group, the surgical success rate in the combined surgery group was higher than standalone mUPPP group (76.74% vs 52.78%, P = .025). These results indicated that patients who underwent combined surgery appear to be more beneficial in improving sleep disorders such as apnea, hypopnea, and hypoxemia.
Limitations
This study is limited by the restrictions inherent in a retrospective and non-randomized study including the inability to avoid selective bias or compare with other OSAHS surgical techniques such as BRP or anterolateral advancement pharyngoplasty. Another inherent weakness of our study was the lack of DISE for OSAHS patients. Conceptually, DISE might provide better information than examinations during wakefulness. Due to the inherent limitation of the retrospective study, we were unable to obtain sufficient DISE data from patients (including a lack of detailed assessment of hypopharyngeal collapse). However, studies have shown that there is a strong positive correlation between FTP grade and DISE findings, which can reduce biases caused by the lack of DISE examination. 27
Conclusions
For OSAHS patients with inferior turbinate hypertrophy and oropharyngeal obstruction, radiofrequency coblation inferior turbinoplasty with mUPPP appears to be a more effective surgical method than mUPPP alone.
Supplemental Material
sj-doc-1-ear-10.1177_01455613241307525 – Supplemental material for Radiofrequency Coblation Inferior Turbinoplasty with Modified UPPP for the Treatment of Obstructive Sleep Apnea-Hypopnea Syndrome
Supplemental material, sj-doc-1-ear-10.1177_01455613241307525 for Radiofrequency Coblation Inferior Turbinoplasty with Modified UPPP for the Treatment of Obstructive Sleep Apnea-Hypopnea Syndrome by Qiushi Tian, Teng Chu and Mingjie Pang in Ear, Nose & Throat Journal
Footnotes
Acknowledgements
The authors wish to thank the physicians in our department for their support in collecting data.
Data Availability Statement
The datasets generated during and/or analyzed during the current study are available from the corresponding author on reasonable request.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval and Informed Consent Statements
This study was approved by the local ethics committee of the Qingdao Municipal Hospital (2024-LW-071) and was carried out according to the Declaration of Helsinki of the World Medical Association. Written informed consents were obtained from all the participants for their anonymized information to be published in this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.