
Abstract
Background:
Positional obstructive sleep apnea hypopnea syndrome (P-OSAHS) is a distinct OSAHS type. Whether velopharyngeal surgery is efficacious for patients with P-OSAHS remains unclear.
Aim/Objective:
To investigate the efficacy and factors influencing velopharyngeal surgery for treatment of patients with P-OSAHS, defined as the apnea hypopnea index (AHI) in different body postures (supine AHI ≥2*nonsupine AHI).
Materials and Methods:
A total of 44 patients with P-OSAHS who underwent velopharyngeal surgery were retrospectively studied. The clinical data of these patients, including polysomnography (PSG), physical examination, and surgical information, were collected for analysis. All patients underwent a PSG about 6 months after surgery to determine the treatment outcomes.
Results:
The overall AHI of the 44 patients decreased from 40.2 ± 18.7 events/h to 18.5 ± 17.5 events/h after surgery (P < .001). There were 29 responders (65.9%) according to the classical definition of surgical success. The percentage of sleep time with oxygen saturation below 90% (CT90) was the only predictive parameter for surgical success (P = .014, odds ratio value = 0.894). There was no significant difference between the change in supine AHI (−55.9 ± 35.2%) and the change in nonsupine AHI (−43.4 ± 74.1%; P = .167), and these 2 parameters were significantly correlated (r = 0.616, P < .001). Among the 38 patients with residual OSAHS (residual AHI ≥5), 28 had persistent P-OSAHS, and the percentage was as high as 82.4%.
Conclusions and Significance:
Patients with P-OSAHS with a lower CT90 value are more likely to benefit from velopharyngeal surgery. Positional therapy could be indicated for most of the patients who are not cured by such surgery.
Keywords
Introduction
Velopharyngeal surgery is one of the most common treatments for obstructive sleep apnea hypopnea syndrome (OSAHS). However, this surgery has limited effect, and treatment outcomes vary greatly among patients. 1 Previous studies have identified some predictors of velopharyngeal surgery, including tonsil size, palate position, and severity of the disease.2-4 These research findings are now widely used to guide patient selection for this treatment.
The positional OSAHS (P-OSAHS) is a distinct OSAHS type, wherein the respiratory events in the supine position happen more frequently than in the nonsupine position. 5 Cartwright first defined P-OSAHS as the condition when the apnea hypopnea index (AHI) in the supine position was ≥2* AHI in the nonsupine position. 6 Positional therapy has proven to be effective in alleviating P-OSAHS.7-9 The efficacy of P-OSAHS is limited as some patients continue to suffer greatly in the nonsupine position.
Currently, it remains unclear whether velopharyngeal surgery is indicated in this type of patients, and few studies have been conducted on the efficacy of P-OSAHS. Therefore, we analyzed the efficacy and the factors influencing P-OSAHS by comparing the clinical features of patients before and after velopharyngeal surgery.
Materials and Methods
Study Population
A total of 44 adult patients who underwent velopharyngeal surgery at the Beijing Tsinghua Changgung Hospital between January 2014 and December 2016 were retrospectively reviewed. All patients were preoperatively diagnosed as P-OSAHS according to a polysomnography (PSG) examination conducted within 2 weeks before surgery. The inclusion criteria were as follows: (1) preoperative AHI ≥5/h, and AHI in supine position ≥2*AHI in nonsupine position; (2) obstructive level of only velopharynx observed by fiberoptic laryngoscopy during Müller’s maneuver; (3) refusal or intolerance to the treatment of continuous positive airway pressure; (4) patients with no systemic diseases that might affect the severity of OSAHS, such as thyroid disorders, myasthenia gravis, or recurrent laryngeal nerve paralysis; (5) patients without severe internal medicine complications such as severe cardiovascular and pulmonary diseases. All patients underwent a postoperative PSG examination about 6 months after surgery for the evaluation of objective surgical efficacy. According to the classical criteria, surgical success was defined as a decline of AHI ≥50% and a postoperative AHI <20/h.
Physical Examination
The otorhinolaryngological examinations were performed for all patients by 1 physician before surgery. The body mass index (BMI), palate position, and tonsil size were recorded for analysis. The BMI was calculated as weight (kg)/height (m2). The palate position was evaluated according to the modified Mallampati grade proposed by Friedman et al. 2 The tonsil size was evaluated according to the Brodsky’s classification. 10
Polysomnography
All the preoperative and postoperative PSG studies were performed at the sleep center of Beijing Tsinghua Changgung Hospital. The monitoring results were assessed in accordance with the scoring guidelines proposed by the American Academy of Sleep Science. 11 An apnea was defined as a complete cessation in nasal pressure signal for ≥10 seconds. A hypopnea was defined as a ≥50% decrease in nasal pressure signal for ≥10 seconds in association with oxygen desaturation of ≥3% or a microarousal. The AHI was calculated as the sum of the numbers of apneas and hypopneas per hour of sleep. The lowest oxygen saturation (LSAT) and the percentage of sleep time with oxygen saturation below 90% (CT90) were also collected for analysis.
Surgical Procedures
All surgical procedures were performed under general anesthesia by a single surgeon. The modified palatopharyngoplasty with uvula preservation (H-UPPP) was performed for all included patients. After the completion of H-UPPP, an additional transpalatal advancement pharyngoplasty (TA) was performed if the velopharyngeal airway observed by 70° endoscope during the surgery remained collapsed or nearly collapsed at the anterior–posterior directions under general anesthesia. The detailed procedures for these surgeries have been previously published.12,13
Statistical Analysis
All statistical analyses were performed with SPSS version 17.0 (SPSS Inc.). The continuous data were displayed as the mean value ± standard deviation. The paired Student t test was used to compare preoperative and postoperative mean values. The unpaired Student t test was used to compare quantitative variables among different groups. The Pearson χ2 test was used to compare categorical variables among different groups. The Pearson correlation analysis was used to analyze the correlation of parameters between different groups. The binary logistic regression analysis was used to evaluate the significance of independent variables for treatment outcomes. Statistical significances were taken at P < .05, and the 95% confidence intervals (CI) were also calculated.
Results
Baseline Information and Treatment Efficacy
Among the 44 patients, there were 40 (90.9%) males and 4 (9.1%) females. The average age was 41.3 ± 9.8 years (age range: 23-62 years). The changes of PSG parameters related to disease severity after surgery are shown in Table 1, suggesting significant decreases in AHI and CT90 (all P < .001), and significant increases in LSAT (P < .001). According to the classical criteria of surgical success, there were 29 (65.9%) responders and 15 (34.1%) nonresponders. No severe complications occurred during the perioperative and follow-up periods, including bleeding, severe infections, persistent nasopharyngeal reflux, and persistent rhinolalia aperta.
Changes of PSG Parameters Related to Disease Severity Postsurgery in the Study Participants.

Abbreviations: AHI, apnea hypopnea index; CT90, the percentage of time with oxygen saturation below 90%; LSAT, the lowest oxygen saturation; PSG, polysomnography.
Factors Influencing Efficacy
Comparisons of the baseline information, physical examination data, and PSG parameters between responders and nonresponders are shown in Table 2, suggesting that the CT90 value of responders was significantly lower than that of nonresponders (P < .05), while there were no significant differences in other parameters between the 2 groups (all P > .05). All the parameters listed in Table 2 were also analyzed using logistic regression analysis to identify the factors that can predict the treatment outcomes. The result suggested that CT90 was the only parameter that could predict the treatment outcomes (P = .014), and the odds ratio was 0.894, with a 95% CI of 0.818 to 0.978.
Data of the Enrolled Patients and Comparison Between the Effective and Invalid Groups.
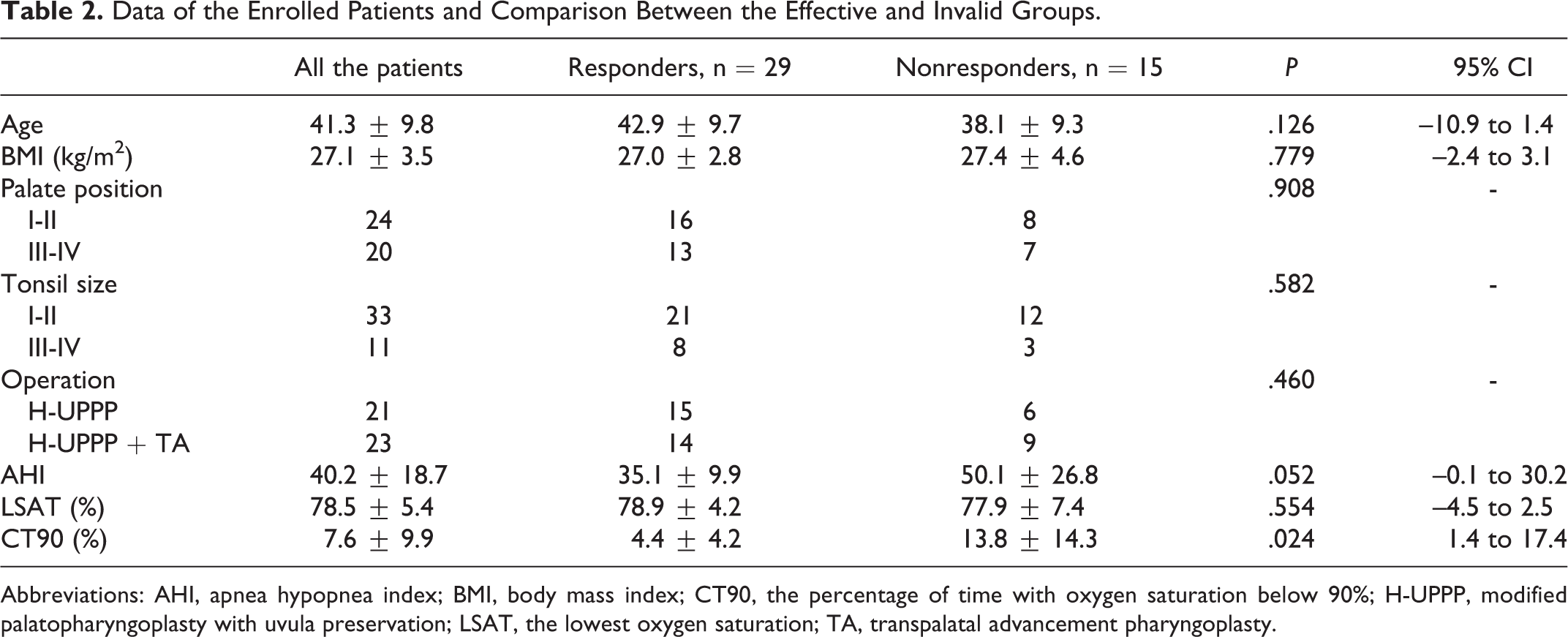
Abbreviations: AHI, apnea hypopnea index; BMI, body mass index; CT90, the percentage of time with oxygen saturation below 90%; H-UPPP, modified palatopharyngoplasty with uvula preservation; LSAT, the lowest oxygen saturation; TA, transpalatal advancement pharyngoplasty.
Relationship Between AHI and Body Position
Apnea hypopnea index in the supine position decreased from 63.6 ± 20.6/h before surgery to 28.3 ± 23.9/h after surgery (P < .001); the percentage change was –100% to 33.5%, with an average of –55.9 ± 35.2%. Apnea hypopnea index in the nonsupine position decreased from 15.9 ± 8.6/h before surgery to 7.9 ± 10.0/h after surgery (P < .001); the percentage change was –100% to 245.7%, with an average of –43.4 ± 74.1%. The percentage change of AHI in the supine and nonsupine positions did not differ significantly (P = .167; Figure 1). A correlation analysis revealed a significant correlation between the two (r = 0.616, P < .001; Figure 2). Among the 34 patients who were not cured after surgery (AHI ≥ 5), 28 had persistent P-OSAHS, accounting for as high as 82.4%.
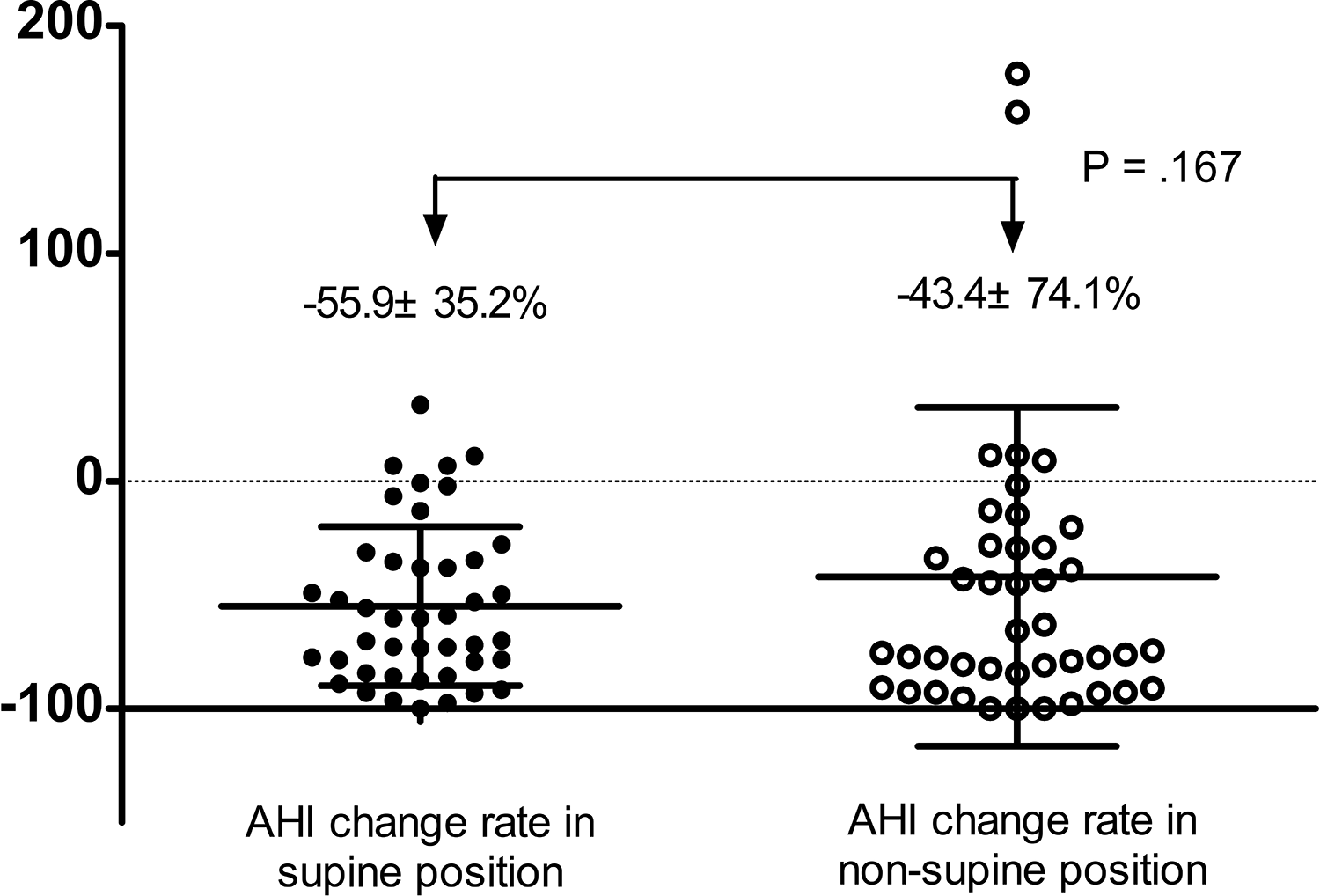
Comparison of apnea hypopnea index in supine and nonsupine positions.
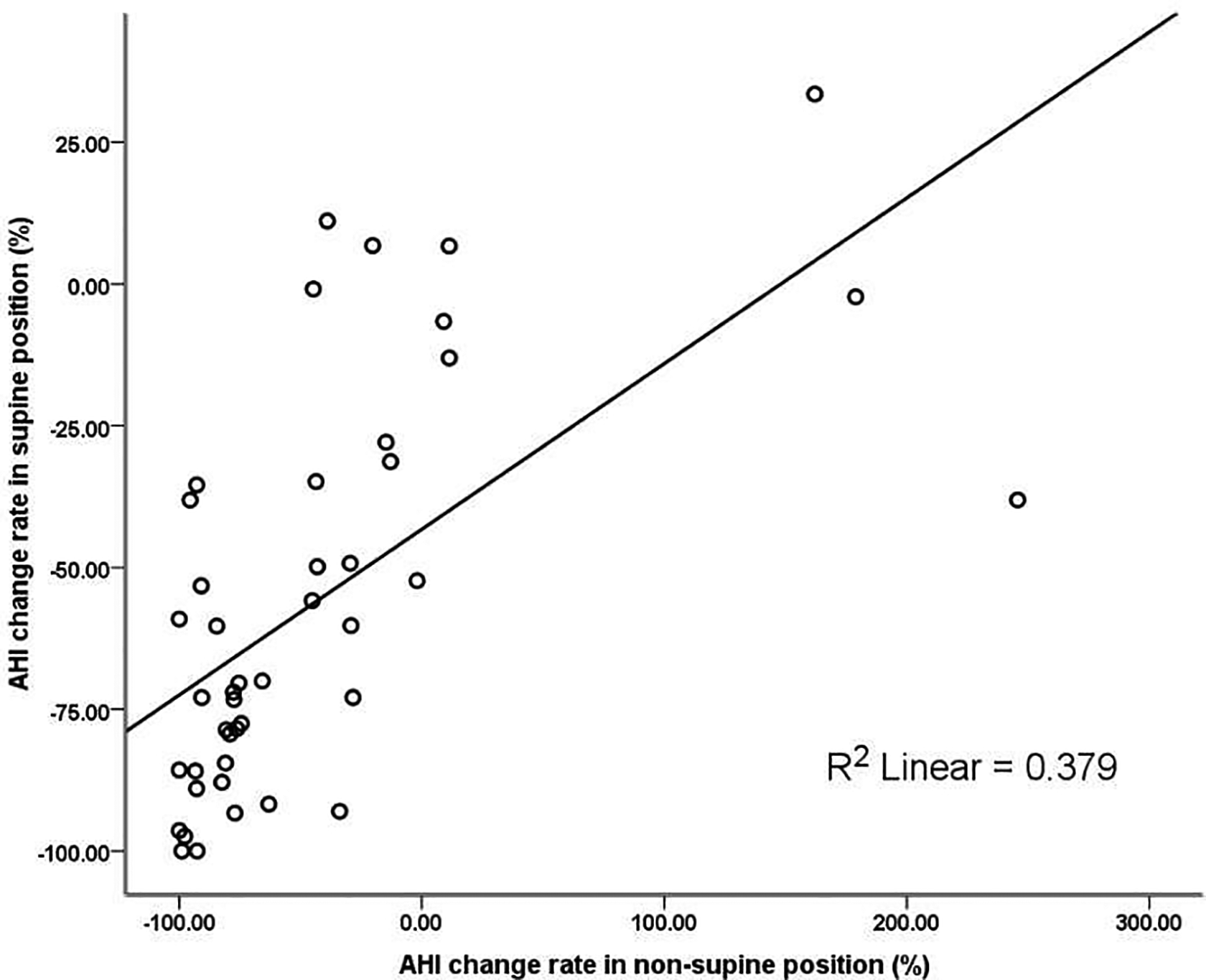
The correlation between apnea hypopnea index change rate in supine and nonsupine positions.
Discussion
It is generally believed that the success rate of velopharyngeal surgery is about 40% in OSAHS. 1 In this study, there was a dramatic decline in AHI after surgery compared with the preoperative AHI (P < .001). The success rate was as high as 65.9%, indicating that many patients benefited from the velopharyngeal surgery.
We further analyzed the predictors of treatment efficacy. The CT90 of the responsive patients was significantly lower than that of the unresponsive patients (P < .05), and the AHI of the responsive patients was nearly significantly lower than that of the unresponsive patients (P = .052). Less severe patients seemed to have benefited more from the surgery. Previous studies showed similar results among the nonselective patients with OSAHS.3,4 Boudewyns et al believed that velopharyngeal surgery can only partially address the pharyngeal cavity collapse. 14 The clinical significance of this research is that for patients with severe P-OSAHS, simple velopharyngeal surgery alone may not revert AHI to the normal range and should be combined with other treatments (weight loss, intraoral devices, and other level surgeries) or mandible surgery. Preoperative CT90 was identified as an independent predictor of efficacy and was closely related to efficacy compared with AHI. This is probably because CT90 can better reflect intermittent hypoxia during sleep. Previous studies have indicated that intermittent hypoxia is related to instability of respiratory regulation, decline of chemoreceptor sensitivity of the respiratory tract, and functional impairment of pharyngeal dilators.15-17 All these factors are believed to be responsible for the poor efficacy of surgery.
We found that tonsil size was not related to treatment outcomes, perhaps due to the following 2 reasons: (1) a limited sample size of the patients, with tonsillar hypertrophy (3°-4°) only accounting for 25% (11/44) of the total; (2) some patients also received H-UPPP combined with TA, resulting in a limited contribution of tonsillectomy to pharyngeal cavity enlargement. However, a previous study in a pediatric population showed no relationship between the tonsil size and OSAHS severity. 18
The mechanism for the reduction of AHI after velopharyngeal surgery is the changes in anatomical structures, especially the changes in velopharynx. In this study, there was no significant difference in the percentage change between AHI in the supine and nonsupine positions (P = .167), suggesting that the anatomical changes had no major impact between the incidences of respiratory events in different positions. After surgery, 28 of 34 cases had persistent P-OSAHS, accounting for as high as 82.4%. In supine position, the pharyngeal cavity collapse is more likely to occur under the action of gravity and muscle tone, which is the reason for the higher AHI in the supine position than in the nonsupine position. However, these leading causes cannot be adequately redressed through surgery, which could be why most patients had persistent P-OSAHS after surgery. Some studies had found that a major percentage of patients with non-P-OSAHS gained positional dependency after velopharyngeal surgery.19,20 The reasons may be the same. The clinical implications of these results were that subsequent positional therapy could be applied to patients unresponsive to surgery and may be more efficient, after surgeries have majorly alleviated the severity of disease.
The limitations of the present study were as follows. First, the sample size was relatively small, and all the surgical procedures were performed by a single surgeon. Therefore, the conclusions need to be validated in further studies with a larger sample size and with surgeries performed by other surgeons. Second, we did not use the preoperative drug-induced sleep endoscopy (DISE) assessment for patient selection, which is considered to be a certain deviation of evaluating the obstructive site and tissues. Instead, we used the fiberoptic laryngoscopy during Müller’s maneuver, which has been proven to show comparable results with DISE. 21 Third, several velopharyngeal procedures had been employed for the treatment of OSAHS. Whether the results are applicable or need to be further explored in patients who underwent other velopharyngeal procedures needs to be assessed. Lastly, the retrospective design of this study may decrease the scientific power of the findings. Hence, a prospective study on more patients is ongoing.
In summary, velopharyngeal surgery can achieve a good efficacy in some P-OSAHS patients, especially severe cases and unresponsive to previous surgery. However, 82.4% of the patients who did not recover through surgery had persistent P-OSAHS. For these patients, positional therapy remains applicable.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by ‘Beijing Hospitals Authority’ Ascent Plan (20191201) and Scientific Research Seed Fund of Peking University First Hospital (2018SF014).