
Abstract
Subcutaneous emphysema is a rare but potentially-serious complication of tonsillectomy. This case report presents a 14-year-old male who developed subcutaneous emphysema following tonsillectomy. A comprehensive literature review was conducted to identify and analyze cases of emphysema following tonsillectomy. The review revealed a diverse range of clinical presentations, from mild neck swelling to severe respiratory distress. Most cases resolved spontaneously with conservative management, but a small subset required surgical intervention. Early recognition, prompt evaluation, and appropriate management are essential to prevent complications and ensure favorable outcomes. This case highlights the importance of considering subcutaneous emphysema as a differential diagnosis in patients presenting with neck swelling or respiratory symptoms following tonsillectomy.
Introduction
Tonsillectomy is among the most-frequently-performed surgeries in otolaryngology, a cornerstone in the management of recurrent tonsillitis and sleep-disordered breathing, including obstructive sleep apnea. 1 Despite its relatively-high safety profile, it is essential for clinicians to be mindful of potential complications and well-prepared to address them. Common postoperative issues can include glossopharyngeal nerve injury, hemorrhage, postoperative infection, tongue swelling, and, less frequently, carotid artery damage. 2 Rare complications, such as pneumothorax or subcutaneous emphysema, may also arise after tonsillectomy, although they often resolve spontaneously. 3 Subcutaneous emphysema involves the presence of air within the fascial planes of connective tissue, either spontaneously or as a result of traumatic or iatrogenic causes. When occurring in the head and neck region, subcutaneous emphysema poses a potentially-life-threatening risk. 4 In cases where large volumes of air enter the fascial planes, areas such as the subcutaneous tissue, retropharyngeal, mediastinal, pleural, and retroperitoneal spaces may be affected. Although subcutaneous emphysema is an uncommon complication, it has been reported in association with various maxillofacial surgical procedures.4,5
This report presents a case of emphysema following tonsillectomy, alongside a thorough review of similar cases documented in the literature, aiming to highlight this exceptionally rare but potentially-critical complication.
Case presentation
A 14-year-old previously-healthy child presented to the otolaryngology clinic with a history of recurrent tonsillitis, necessitating multiple courses of antibiotics. On physical examination, he was noted to have grade 3 cryptic tonsils, leading to the decision to proceed with surgical intervention. The tonsillectomy was performed under general anesthesia with endotracheal intubation, which was carried out smoothly without any complications. The procedure involved the use of bipolar cautery, but the tonsils were fibrotic and adherent, making dissection challenging. Immediately following extubation, the patient developed subcutaneous emphysema at both mandibular angles, extending slightly into the cheeks bilaterally (Figure 1; Supplemental Video 1). He was promptly evaluated to ensure there was no active bleeding, and his vital signs remained stable throughout. As a precaution, he was admitted to the ENT department for 24 hours of observation to monitor for any potential complications. The emphysema began to resolve within the first hour postoperatively, and by 6 hours, it had completely subsided without any adverse effects. To prevent forced glottic closure and reduce the risk of infection, the patient was kept on prophylactic antibiotics. The remainder of his hospital course was uneventful, with stable respiratory function and full resolution of the emphysema. He was discharged the following day in stable condition, with normal vital signs and no lasting complications.

The images show swelling in the neck below the angles of the mandible, more pronounced on the left side, in addition to the area beneath the chin.
Discussion
Subcutaneous emphysema is an uncommon complication after tonsillectomy, ranging from mild air collection to severe, life-threatening conditions such as airway compression, pneumomediastinum, and pneumothorax. 6 The mechanisms behind this complication are uncertain, but 2 theories are cited. The first theory links it to anesthesia, suggesting a laryngeal or tracheal tear from intubation, cuff inflation, or high-pressure ventilation.7,8 The second theory proposes air entry through a pharyngeal tear at the superior constrictor muscle and deep cervical fascia, via the tonsillar bed.8,9 Emphysema can present immediately during or after surgery, even without observed intraoperative injury.9,10
Our review identified 37 cases of emphysema as a complication following tonsillectomy, documented in the literature, including our case presented in this report. The patients’ ages ranged from 3 to 55 years, with a mean age of 23.7 years. The distribution was nearly equal between genders, with 19 females and 18 males. The symptoms were varied and included swelling, cough, dyspnea, vomiting, chest pain, dysphagia, decreased neck motion, stridor, crepitus, sore throat, neck pain, gagging, bleeding, increased fluid intake, and fever. The most common symptom was swelling, which was the main presentation in 89.1% of cases (33 cases), followed by dysphagia and dyspnea. In 29 cases, tonsillectomy alone was performed, while 8 cases involved adenotonsillectomy. Regarding radiological investigations, 14 cases had only an X-ray, while 21 cases required additional imaging such as CT, fluoroscopy, flexible bronchoscopy, or barium swallowing. The duration of emphysema ranged from immediate resolution in the operating room to 7 days, with a mean duration of 1.3 days. As for management, 29 cases were treated conservatively. Among these, 6 cases were managed with observation only, 23 cases received antibiotics, 2 cases were given cough suppressants, 1 case was prescribed laxatives, 1 case received intravenous steroids, and 1 case was treated with intravenous immunoglobulin. Only 8 cases required intervention, primarily for repairing the tonsillar fossa, airway management, or associated chest procedures. In terms of outcomes, only 3 patients required admission to the Intensive Care Unit (ICU), and only 1 patient died within 1 day. The mean follow-up period was 4.9 days, excluding an outlier in which the follow-up extended to 1 year. Table 1 summarizes all cases documented in the literature.
Summary of All Cases of Emphysema Following Tonsillectomy in the Literature.
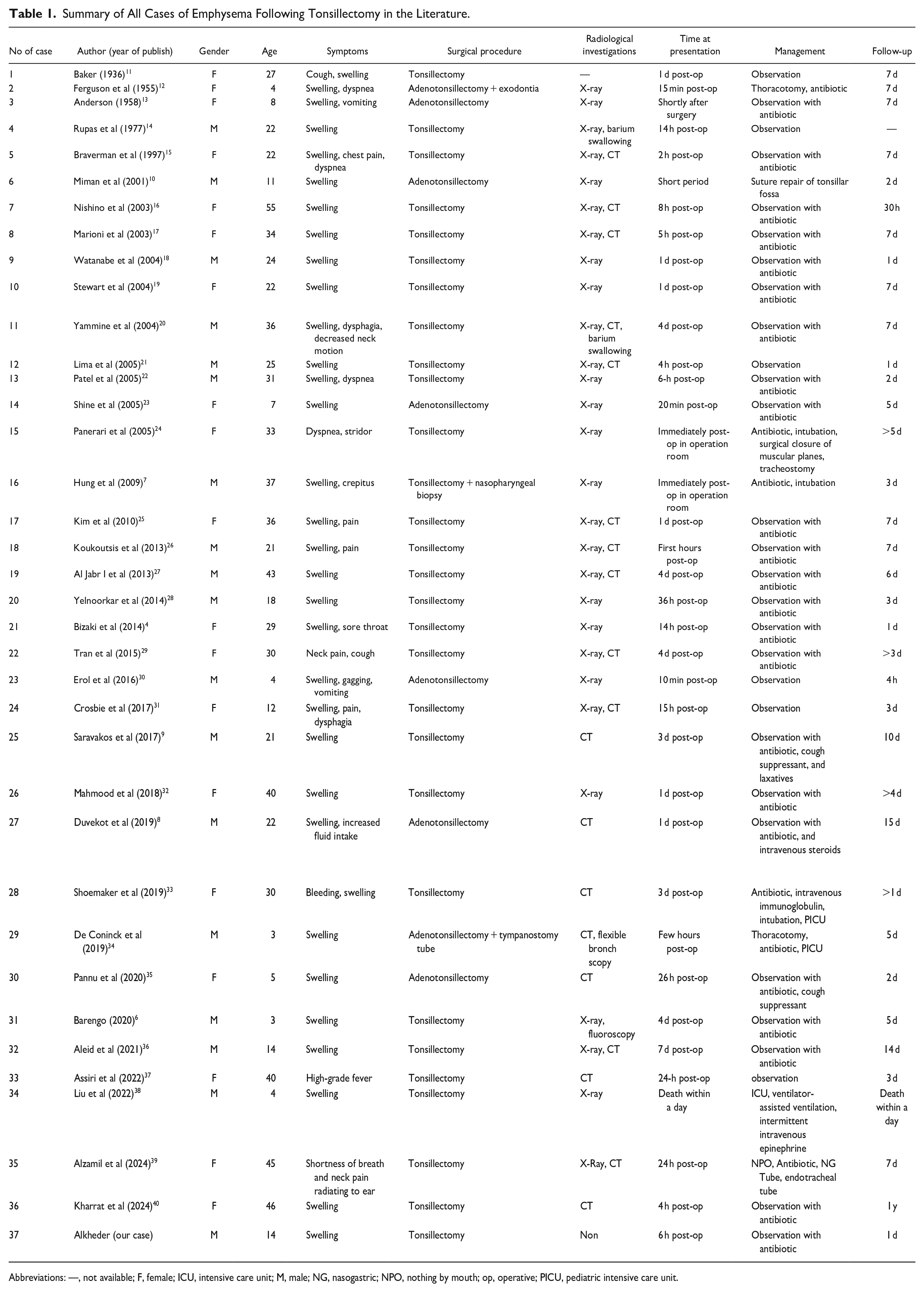
Abbreviations: —, not available; F, female; ICU, intensive care unit; M, male; NG, nasogastric; NPO, nothing by mouth; op, operative; PICU, pediatric intensive care unit.
This wide age range suggests that physicians should consider emphysema as a differential diagnosis for postoperative issues in any patient, regardless of age or gender, especially when specific symptoms such as neck swelling and respiratory discomfort are present.
The symptom profile associated with post-tonsillectomy emphysema is diverse, ranging from localized symptoms (eg, neck swelling, pain) to systemic signs (eg, fever) and respiratory distress (eg, dyspnea, stridor). Given the proximity of the tonsillar region to respiratory structures, it is understandable that emphysema in this area can lead to both airway and pharynx symptoms. So, physicians should be vigilant in monitoring symptoms, particularly in patients who report increasing neck swelling or respiratory symptoms postoperatively. These symptoms should prompt further investigation to rule out emphysema. The possibility of emphysema should be considered regardless of whether only tonsillectomy or adenotonsillectomy was performed, as the complication can occur with either procedure.
Radiological evaluation played an essential role in diagnosing emphysema, with 14 cases managed with only an X-ray and 21 requiring additional imaging such as CT, fluoroscopy, or bronchoscopy. X-rays may detect subcutaneous emphysema but often lack the sensitivity to identify deeper air collections or subtle fascial plane involvement, which explains the need for advanced imaging in some cases. A tiered imaging approach should be adopted. For patients presenting with mild symptoms, an initial X-ray may be adequate. However, for those with more severe respiratory complaints or unclear findings on X-ray, CT, or bronchoscopy should be considered. CT scans, in particular, can delineate the exact location and extent of air, which is crucial for deciding between conservative and interventional management.
This relatively-short mean duration suggests that emphysema following tonsillectomy is usually self-limiting, often resolving within days without long-term sequelae. The rapid resolution may be attributed to the natural reabsorption of subcutaneous air, especially in cases without significant airway compromise or infection. The fascial planes involved likely allow air to dissipate relatively quickly, limiting the duration of symptoms. Clinicians should provide reassurance to patients, noting that the complication generally resolves within a few days, particularly with conservative management. However, they should still maintain close monitoring for signs of worsening respiratory function, as rapid intervention could be required if symptoms escalate.
The majority of cases (29) were treated conservatively, with observation and antibiotics being the most common measures. The 6 cases managed with observation alone emphasize that mild cases may not require any intervention. However, the administration of antibiotics in 23 cases suggests a perceived risk of secondary infection, especially with the fever. In rare cases, additional treatments such as intravenous steroids or immunoglobulins were used, which may reflect attempts to reduce inflammation and immune modulation in severe or complicated cases. A conservative approach should be the first line for most cases, especially in the absence of infection or airway compromise. Antibiotics may be considered to prevent infection, although their use should be evaluated on a case-by-case basis. Clinicians might also consider cough suppressants and other symptomatic treatments as appropriate. Interventions may become necessary if conservative management fails or if there is evidence of air tracking into the mediastinum or other vital structures. For patients not responding to conservative treatment or with worsening symptoms, early consultation with specialists in airway management or thoracic surgery is advisable. Repairing tissue disruption in the tonsillar fossa could prevent further air leakage, particularly in cases of extensive emphysema.
Most patients had favorable outcomes, with only 3 ICU admissions and 1 fatality. The short mean follow-up period (4.9 days) suggests that prolonged follow-up may not be essential, except in cases with complications or residual symptoms. The generally-good prognosis reflects the self-limiting nature of this complication in the majority of cases. However, the fatality reported within a day underscores that, although rare, severe outcomes can occur. Prompt recognition and management remain critical for improving outcomes. A minimum follow-up period of 4 to 5 days may be sufficient in uncomplicated cases. For patients with severe presentations, a longer follow-up is warranted to monitor for complications.
In our presented case, it is difficult to determine the exact mechanism behind this complication, as there is evidence supporting both hypothesized causes of this complication. One hypothesis suggests that the cause might be related to anesthetic procedures, especially since the swelling appeared immediately after extubation. The other hypothesis involves injury to the pharyngeal constrictor muscle and tonsillar fossa, especially given that the tonsils were severely fibrotic and adherent, which might have necessitated a certain level of force during dissection, despite the absence of any signs indicating injury to the tonsillar fossa following the tonsillectomy.
This review underscores the importance of prompt diagnosis and appropriate management of emphysema as a post-tonsillectomy complication. Clinicians should maintain a high index of suspicion and utilize a combination of imaging and conservative management, reserving surgical interventions for refractory cases. Further research into the optimal management strategies and long-term outcomes of post-tonsillectomy emphysema is warranted to enhance patient care.
Conclusion
This case report highlights the importance of recognizing and managing subcutaneous emphysema as a potential complication of tonsillectomy. While this complication is rare, its rapid onset and potential for severe respiratory compromise necessitate prompt attention. Our review of the literature emphasizes the diverse clinical presentation of this condition, ranging from mild neck swelling to life-threatening airway obstruction. The majority of cases resolve spontaneously with conservative management, including observation and antibiotics. However, a small subset may require surgical intervention to address airway compromise or repair tissue damage. Physicians should be vigilant in monitoring patients postoperatively for signs of emphysema, such as neck swelling, respiratory distress, or subcutaneous crepitus. Early recognition and timely management are crucial to ensure favorable outcomes. Further research is needed to better understand the underlying mechanisms and optimal treatment strategies for this uncommon but potentially-serious complication.
Footnotes
Data Availability Statement
The data that support the findings of this study are available from the author or corresponding author upon reasonable request.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval
Our institution does not require ethics approval for reporting individual cases. Written informed consent was obtained from the patient’s legal guardian for publication of this case report and accompanying images.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.