
Abstract
Horner’s syndrome, though very rare, is a recognized complication following tonsillectomy, as presented in this case report of a 4.5-year-old girl. She developed Horner’s syndrome after a tonsillectomy, which was performed using cold steel technique and bipolar diathermy for hemostasis. The patient exhibited symptoms such as ptosis, miosis, and anhidrosis on the left side, detected following a secondary post-tonsillectomy hemorrhage that required surgical intervention. No improvement in Horner’s syndrome was noted after 3 months. Our review of the literature revealed 15 documented cases of Horner’s syndrome as a complication of tonsillectomy, with an increase in recent years possibly due to the advancements in surgical techniques and heightened awareness of the condition. Interestingly, Horner’s syndrome occurred with a wide range of surgical methods, indicating that the etiology is likely multifactorial, involving factors such as surgical technique, anatomical variations, and the extent of cauterization. This report emphasizes the need for caution in the application of modern hemostatic techniques, advocating for a balanced approach that considers traditional methods like ligation and suturing, which may reduce the risk of such complications. Continuous reporting and further research are crucial to better understanding the mechanisms behind Horner’s syndrome following tonsillectomy and improving patient outcomes.
Introduction
Tonsillectomy was first performed over 2000 years ago, with the oldest reference to the procedure dating back to 1000 BC.1,2 Today, more than 500,000 tonsillectomies are performed annually in the United States, making it the most common major surgery and the second most commonly performed procedure on children behind myringotomy with tube insertion.1,2 Several different techniques and instruments are currently in use in tonsil surgery, such as coblation, monopolar electrocauterty, cold steel, diode laser, bipolar scissors, harmonic scalpel, ligaSure, CO2 laser, microdébrider, and radiofrequency ablation. Regardless of the technique, there are many posttonsillectomy complications such as pain, airway fire, nausea and vomiting, condyle fracture, temporomandibular joint dysfunction, poor feeding/dehydration, subcutaneous emphysema, electrolyte imbalance, dysgeusia/ageusia/phantogeusia, voice changes, tongue paresthesia, primary or secondary hemorrhage, Grisel syndrome, death (aspiration, cardiopulmonary failure), internal jugular vein thrombosis, post-obstructive pulmonary edema, vascular injury, and laryngospasm. Posttonsillectomy hemorrhage is the most commonly encountered serious complication after tonsillectomy. Bleeding occurring during the first 24 hours is known as primary posttonsillectomy hemorrhage and occurs approximately 0.2% to 2.2% of the time. Secondary posttonsillectomy hemorrhage occurs after 24 hours but tends to peak at 7 to 10 days postoperatively. The cause of late bleeding is unclear but is believed to be related to the shedding of eschar formed at the time of surgery. Secondary posttonsillectomy hemorrhage occurs 0.1% to 3% of the time.1,2 Here, in our report, we present a rare case of a complication, represented by Horner’s syndrome following tonsillectomy with excessive use of cauterization. This condition presents with miosis, ptosis, apparent enophthalmos, and anhidrosis on the affected side. According to our review of the literature, this is the 15th case that documents this complication. In addition, we present a comprehensive review of the literature.
Case Presentation
A 4.5-year-old girl was brought to the ENT emergency department, and referred from an external hospital, presenting with difficulty swallowing and a droopy left upper eyelid, along with a generally poor condition after a tonsillectomy. The child had undergone a tonsillectomy 8 days prior, with an uneventful postoperative period, but on the 7th day, she experienced secondary post-tonsillectomy hemorrhage. As a result, she was re-admitted to the operating room, and the bleeding was controlled. The tonsillectomy was performed using the cold steel technique and bipolar diathermy for hemostasis under general anesthesia. The parents noticed drooping of the left upper eyelid immediately after the second surgery. Upon examination, a severe burn was found in the area of the tonsils, especially on the left side (Figure 1), along with decreased left pupil size (miosis; Figure 2) and drooping of the left upper eyelid (ptosis; Figure 3). Decreased sweating and tearing were also observed on the same side. Based on these findings, Horner’s syndrome was diagnosed as a complication following the tonsillectomy. An MRI was performed to rule out neurological damage, which returned normal results. The patient was administered antibacterial treatment, and her general condition improved. She was discharged from the hospital after a week. Follow-up for 3 months showed no improvement in the symptoms of Horner’s syndrome.
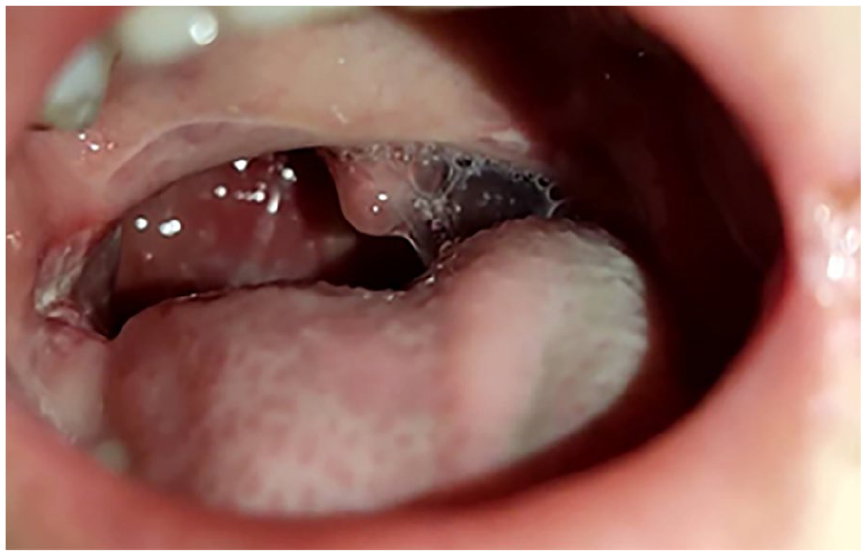
View of the oropharynx, showing the burning of the tonsil site and signs of excessive bipolar diathermy use.

A view showing decreased left pupil size (miosis).

A view showing drooping of the left upper eyelid (ptosis).
Discussion
Horner’s syndrome is a neurological condition characterized by a constellation of symptoms resulting from damage to the sympathetic nerve pathway. The condition, affecting approximately 1.42 children per 100,000, arises from disruption of the oculosympathetic nerve chain, which extends from the hypothalamus to the orbit. While neoplasms and trauma are frequently associated with Horner’s syndrome, postoperative complications involving the neck and thorax represent the most prevalent causes of acquired cases.11,12
The precise cause of Horner’s syndrome remains unclear. We suggest 2 potential mechanisms to elucidate its origins. First, inflammation and swelling around the tonsillar tissue posttonsillectomy may exert pressure on the sympathetic plexus. Alternatively, the more probable explanation involves direct injury to the sympathetic plexus due to the elevated temperatures employed during the procedure, aligning with the specifics of our case. Additional potential mechanisms contributing to this complication encompass the infiltration of local anesthetic into the peritonsillar region, as well as the formation of postoperative hematomas or abscesses that exert pressure on the sympathetic ganglion.
The close anatomical relationship between the palatine tonsil and the superior cervical ganglion puts the oculosympathetic pathway at risk during tonsillectomy. The superior cervical ganglion is positioned approximately 1.5 cm posterolateral of the palatine tonsil. However, anatomical variations may occur where this ganglion is located closer to the palatine tonsil. In such cases, the oculosympathetic pathway could be at a higher risk of injury due to its increased proximity. 4 However, isolated Horner’s syndrome as a complication of tonsillectomy is a rare entity, as it has been reported very little in the literature.
Our review uncovered 15 documented cases in the medical literature of Horner’s syndrome as a complication following tonsillectomy, including the case presented in this report. This rare complication was first described in 1933. This complication was reported in 8 children and 6 adults, while 1 report did not specify the patient’s age. Among them, 8 were females, 6 were males, and 1 report did not specify the gender. Horner’s syndrome was temporary in 9 cases, with durations ranging from 2 hours to 7 years, with an average of 387.525 days. By contrast, 6 reports indicated that Horner’s syndrome was persistent, with an average follow-up period of 166.33 days. Tonsillectomy was performed under local anesthesia in 6 cases and under general anesthesia in 8 cases, while 1 case involved both types of anesthesia. Regarding the surgical technique used, 4 cases involved sharp dissection, 2 cases used a combination of blunt dissection, snare, and electrocautery, 1 case used blunt dissection and snare together, 2 cases used blunt dissection and electrocautery together, 3 cases employed radiofrequency ablation, while 3 reports did not specify the surgical technique used.
Through our review, we observed an increase in this complication in recent years. From the first recorded case in 1933 until the early 2000s, approximately 70 years, there were 7 documented cases. However, in the last 18 years, 8 cases have been recorded. This may be linked to significant advancements in surgical techniques for tonsillectomy and hemostasis methods, particularly electrical techniques. At the same time, it is important to consider that this increase could also be due to improved diagnosis and greater awareness of the condition, which may have been overlooked or undocumented in the past. Regarding age, we observed a slight predominance of this complication in children compared to adults. This could be attributed to specific anatomical characteristics in children, particularly concerning the anatomy of the neck and cervical sympathetic chain in relation to the tonsils. Alternatively, it could simply reflect the fact that tonsillectomy is a more common procedure in children. As we mentioned earlier, there were 9 cases of temporary Horner’s syndrome and 6 cases of persistent. However, when considering the follow-up periods in both groups, which were 387.525 and 166.33 days, respectively, we find that the average follow-up period in the persistent group was much shorter compared to the temporary group. This may suggest that the recovery rate for this complication is higher than reported, but in some cases, the follow-up period was insufficient. Therefore, we should be cautious when concluding the final outcome of the condition. Looking at the surgical techniques used in tonsillectomy and hemostasis methods, we found that this complication occurred with the use of the most commonly known and widespread techniques, with no significant numerical differences between them. In other words, Horner’s syndrome following tonsillectomy was not strongly or significantly associated with any particular technique. This leads us to suggest that the mechanism of Horner’s syndrome after tonsillectomy may be multifactorial. It could be related to the type of technique used, the surgeon’s approach (as seen in our case with excessive use of cautery), anatomical factors, or improper use of electrical and thermal methods for hemostasis. Table 1 presents a summary of all cases of Horner’s syndrome following tonsillectomy documented in the literature.
Summary of All Cases of Horner’s Syndrome Following Tonsillectomy Reported in the Literature.
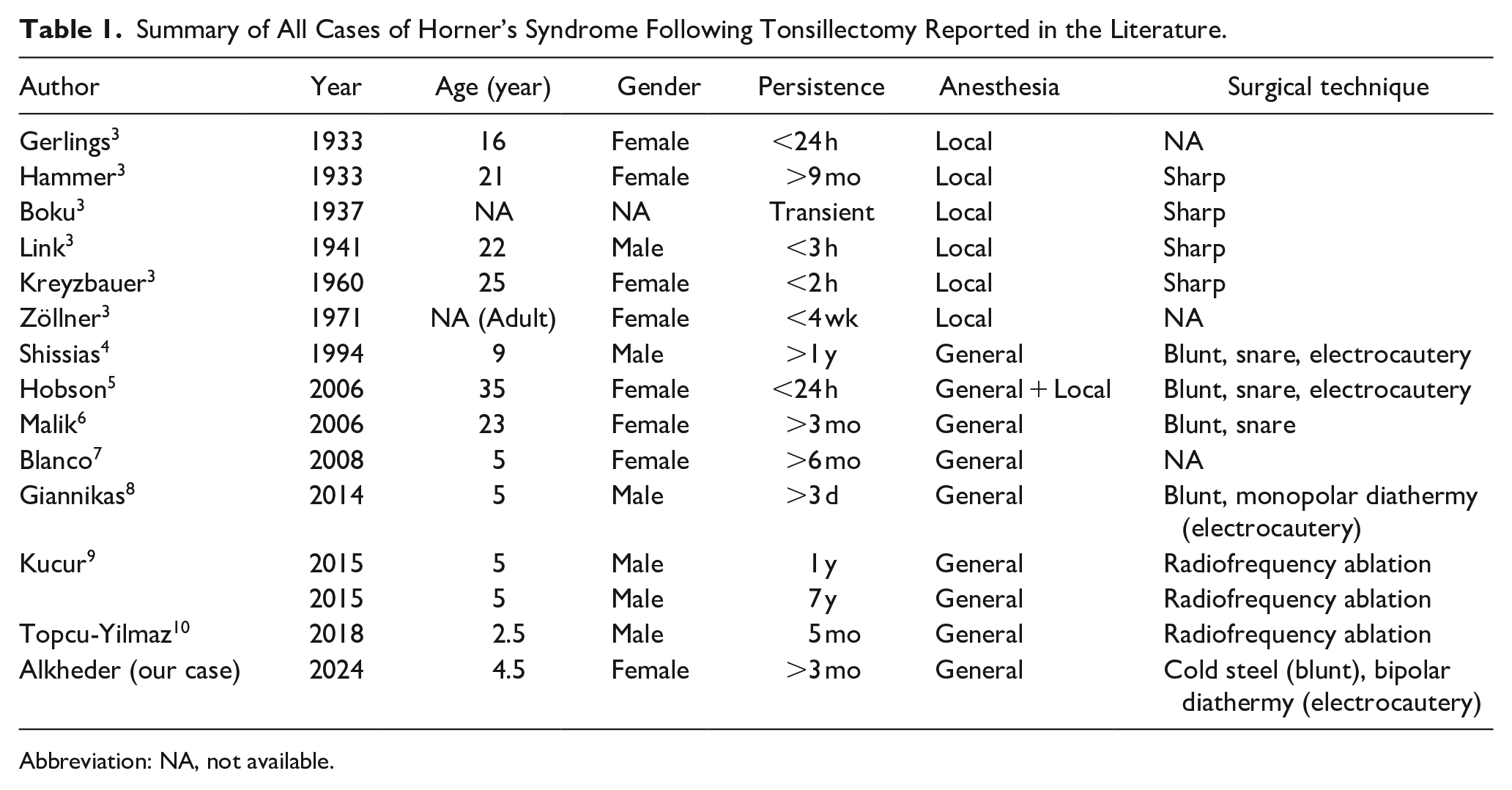
Abbreviation: NA, not available.
As a recommendation, we suggest that modern techniques for tonsillectomy and hemostasis should be used with caution and prudence, avoiding overuse or aggressive application. Traditional methods of excision and hemostasis, such as ligation and suturing, which seem to be safer regarding this complication, should also be considered.
Conclusion
Horner’s syndrome is a rare but significant complication following tonsillectomy, as highlighted in our case report. While the exact mechanism remains unclear, the multifactorial nature of the condition suggests that various elements, such as surgical technique, anatomical factors, and the extent of cauterization, may contribute to its development. Our case, along with the reviewed literature, underscores the importance of cautious application of modern surgical and hemostatic techniques to minimize such risks. Surgeons should remain vigilant and consider less aggressive methods, such as traditional ligation, when appropriate, to reduce the potential for severe complications. Continuous follow-up and reporting of such cases are essential for further understanding and improving patient outcomes.
Footnotes
Author Contributions
A.A.: Validation, Writing – review – editing, Visualization, Methodology, Software, Writing – original draft, Formal analysis. H.A. and V.A.: Validation, Writing – review – editing, Visualization, Writing – original draft, Formal analysis. Z.A.: Validation, Formal analysis, Writing – review – editing, Writing – original draft, Methodology. S.A.: Validation, Writing – review – editing. A.M.: Supervision, Writing – review & editing, Project administration.
Data Availability Statement
The data that support the findings of this study are available from the author or corresponding author upon reasonable request.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval
Our institution does not require ethical approval for reporting individual cases. Written informed consent was obtained from the patient’s legal guardian for publication of this case report and accompanying images.