
Abstract
Paragangliomas are rare neuroendocrine tumors originating from the paraganglia. They are mostly benign, slow-growing, and non-secretory. This report describes a rare case of a catecholamine-secreting paraganglioma located in the pterygopalatine fossa. A 45-year-old man presented with severe hypertension, occipital headache, and facial pain. Imaging revealed a large pterygopalatine mass, initially misdiagnosed as chondrosarcoma. Gamma knife stereotactic radiosurgery was performed, followed by surgical resection via a maxillary swing approach. Histological examination confirmed the zellballen pattern typical of paraganglioma. Post-surgery, the patient’s blood pressure normalized immediately and subsequently. This case highlights the diagnostic challenges of head and neck paragangliomas in atypical locations and underscores the importance of surgical intervention for catecholamine-secreting tumors. Future studies should focus on refining diagnostic protocols and comparing the efficacy of radiosurgery versus surgical resection for these tumors.
Keywords
Introduction
Paragangliomas are a rare type of neuroendocrine tumor originating from the paraganglia associated with the sympathetic and parasympathetic systems, deriving embryologically from neural crest cells. 1 These tumors are mostly benign and slow-growing, with 95% being non-secretory. They are considered the extra-adrenal counterparts of pheochromocytomas. 2 Head and neck paragangliomas make up 65% to 70% of all paragangliomas and 0.65% of head and neck tumors. 3 Predominantly found in middle-aged women, their most common site is the carotid body (60%), followed by the temporal bone (20%-30%) and vagal nerve (5%). They can also arise in less common sites such as the glossopharyngeal paraganglia, jugular-tympanic region, larynx, nasal cavity, trachea, thyroid gland, and orbit. Although most paragangliomas are benign, 6% to 19% can behave malignantly, causing distant metastases. 2 Traditionally, head and neck paragangliomas are considered non-secreting, unlike their thoracic or abdominal counterparts, with secretory tumors typically linked to sympathetic origin. It is estimated that 3% to 4% of all paragangliomas secrete catecholamines, though they all have the potential to do so. Symptoms indicating a secretory paraganglioma include tachycardia and hypertension, often presenting with headaches, palpitations, and sweating. 4 This report details a rare case of a catecholamine-secreting paraganglioma located in the pterygopalatine fossa, with surgical management of this unique tumor.
Case Presentation
A 45-year-old man suffered from occipital headache which was the result of increased blood pressure (SBP was 300 mmHg), so he was admitted to the ICU, and further labs and images workup were done, brain MRI showed a large pterygopalatine well-enhanced mass 3.1*3*2.2 cm extended to the left nasopharynx, sphenoid, ethmoidal, and maxillary sinuses. The patient complained of left facial pain and odynophagia for 1-year duration with a normal neurological examination. Headaches, palpitations, diaphoresis, severe hypertension, and erectile dysfunction manifested frequently as spells at variable times. No history of smoking or weight loss was informed. According to the location of the mass, the patient referred for Gamma knife stereotactic radiosurgery treatment without a biopsy being taken (suspicion of chondrosarcoma), which was targeted with 20 numbers of shots, prescribing 16 Gy at the external margins and 32 Gy at the center of the tumor. No complications was occurred and the patient discharged on the same day. MRI to the head was repeated 3 months later to reveal low signal lobulated mass on the T1-weighted image and intermediate signal intensity on the T2-weighted image with mild homogeneous enhancement on the postgadolinium T1-weighted image (Figure 1). Normal abdominal and pelvis ultrasound was assured. The tumor was resected using a maxillary swing approach (Figures 2 and 3). Normal blood pressure was attained the next day and thereafter. The histological examination showed a zellballen pattern of paraganglioma (Figure 4).
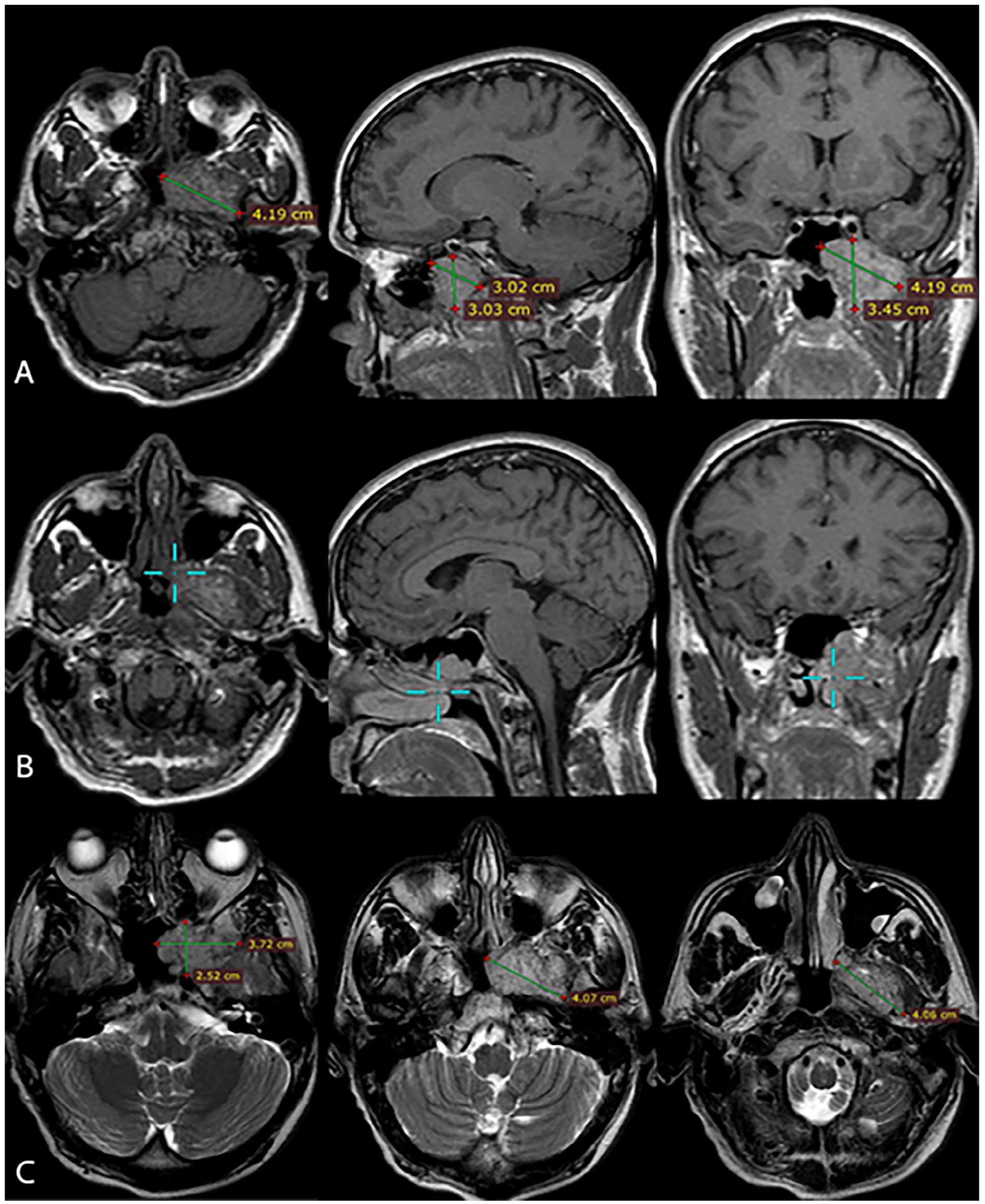
MRI to the head (A) postgadolinium T1-weighted images show the greatest dimensions of the lobulated mass 4.19*3.45*3.02 cm (B) postgadolinium T1-weighted images show 3D cursor localization across sections for adequate surgical planning (C) axial T2-weighted images demonstrate sequential extensions of the lesion with adjacent structures.
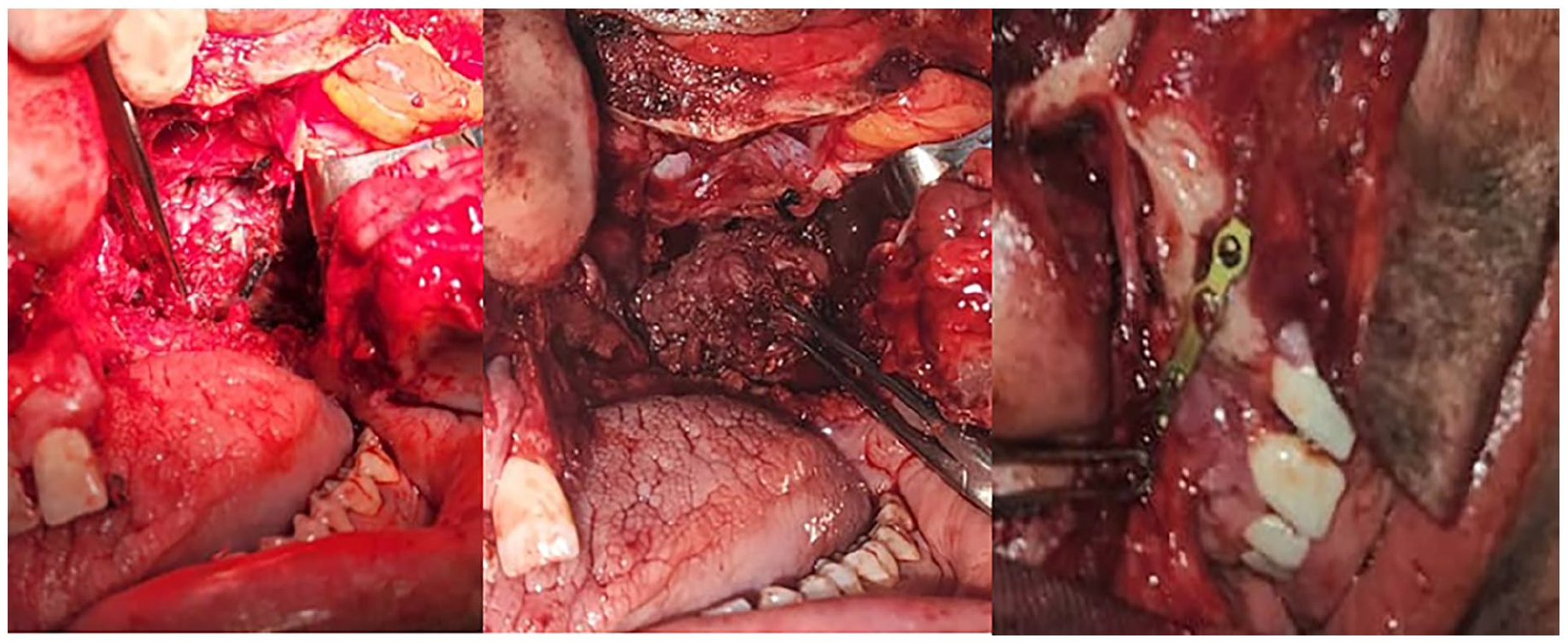
Tumor in the pterygopalatine fossa after exposure using maxillary swing approach.
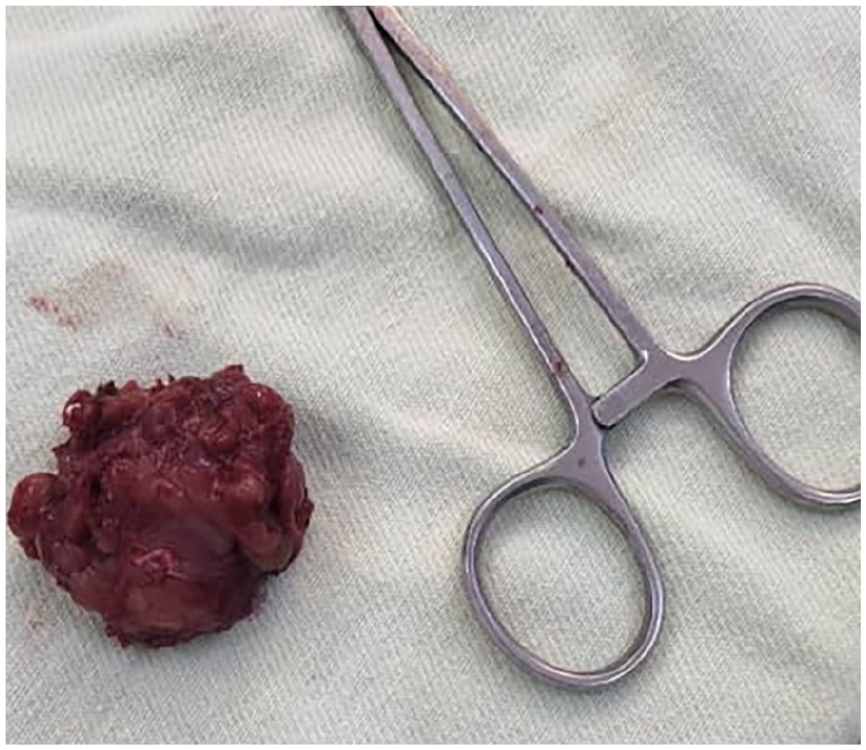
Well-defined soft tissue mass measuring 4.5*4*3.5 cm with solid cut surfaces.
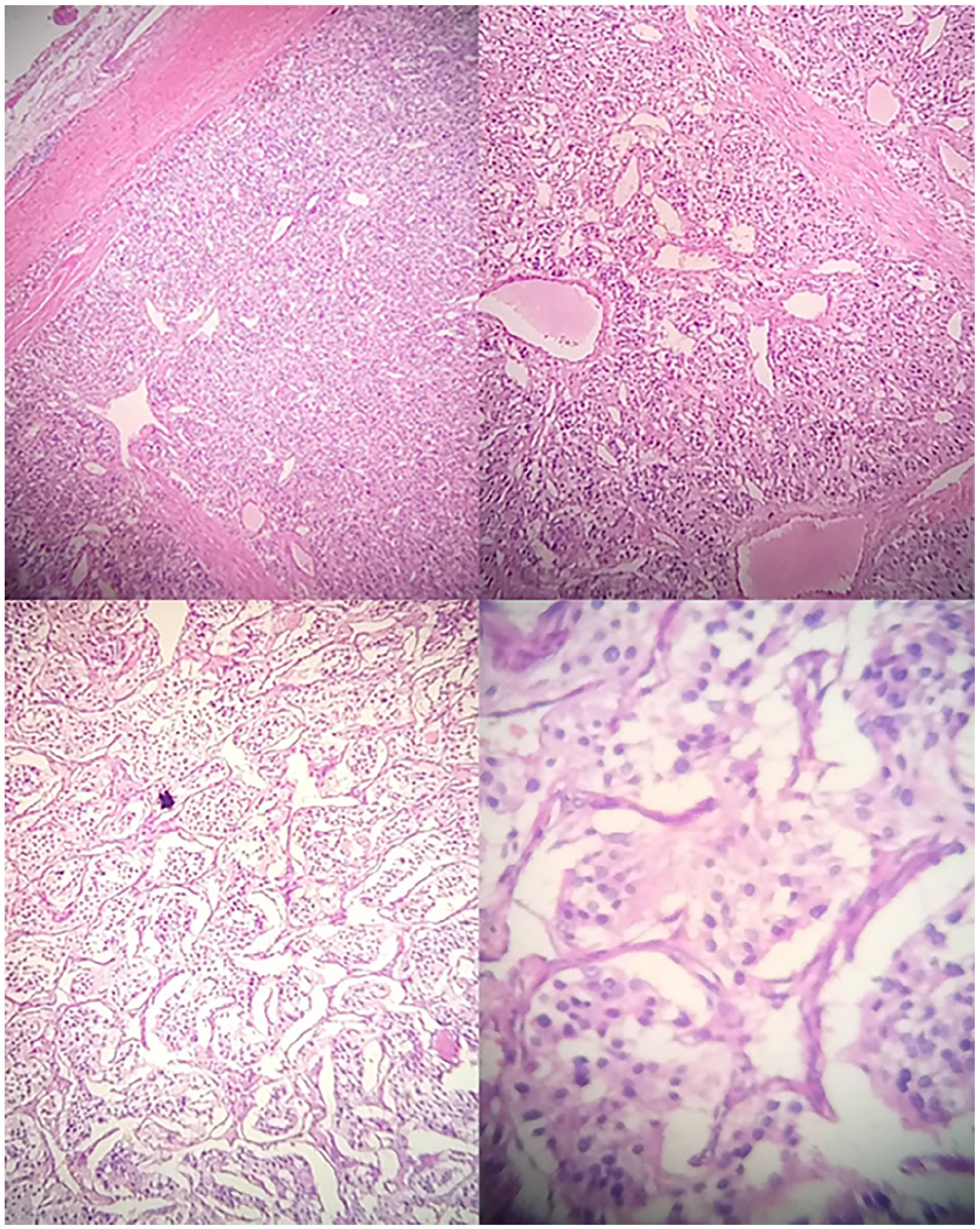
Histological examination shows zellballan pattern of paraganglioma HE-stained pictures with no necrosis, mitotic activity, or vascular invasion is seen.
Discussion
Head and neck paragangliomas typically emerge as silent, space-occupying masses in individuals in their 30s or 40s.5,6 This case highlights a unique presentation of catecholamine-secreting paraganglioma in the pterygopalatine fossa, an unusual and infrequently documented site for these tumors. Paragangliomas in this region are exceedingly rare and typically non-secreting, which makes this case notable. The pterygopalatine fossa is a deep structure located posterior to the maxillary sinus, and tumors in this region are rare. Most masses in this area are typically benign, including schwannomas, vascular malformations, and some types of sarcomas. 7 The differential diagnosis of a mass in this region would not typically include a paraganglioma due to its rarity, especially a catecholamine-secreting variant. This unique anatomical presentation likely contributed to the initial misdiagnosis of chondrosarcoma in this case, underscoring the diagnostic challenges associated with these tumors. 8 The patient’s clinical symptoms of occipital headache, facial pain, and odynophagia are consistent with mass effect from the tumor invading adjacent structures such as the maxillary and ethmoid sinuses, as well as the nasopharynx. 9 The frequent spells of hypertension, palpitations, and diaphoresis point toward catecholamine excess, a hallmark of functional paragangliomas. Interestingly, the tumor’s catecholamine-secreting nature was not suspected preoperatively due to the unusual location, as functional paragangliomas are more commonly associated with adrenal or abdominal locations. 10 The imaging findings in this case well-defined mass with moderate enhancement on post-contrast MRI are characteristic of paragangliomas. The lesion’s intermediate signal intensity on T2-weighted images and mild homogenous enhancement after gadolinium contrast administration aligns with the typical radiologic appearance of paragangliomas. 11 The histopathological zellballen pattern, consisting of tumor cells arranged in nests surrounded by sustentacular cells, is pathognomonic of paragangliomas, confirming the diagnosis upon resection. 12 Given the tumor’s complex location in the pterygopalatine fossa and its initial misidentification as a chondrosarcoma, the decision to proceed with Gamma knife stereotactic radiosurgery was appropriate at the time. Radiosurgery is an effective modality for controlling tumor growth in this region, where surgical resection can be challenging due to the proximity to critical neurovascular structures. 8 However, definitive treatment for catecholamine-secreting paragangliomas generally involves surgical resection, as seen in this case, which led to immediate normalization of blood pressure postoperatively. 13 The maxillary swing approach, used for surgical resection, provides excellent exposure of the pterygopalatine fossa and adjacent regions, allowing for safe tumor removal with minimal complications. The successful resection of the tumor and subsequent histopathological confirmation highlight the importance of surgical intervention in managing functional paragangliomas, even in anatomically challenging locations. The decision to proceed with surgical resection was based on the persistence of symptoms and the need for definitive treatment. The successful resection and normalization of blood pressure postoperatively demonstrate the efficacy of surgical intervention in managing these tumors. The “zellballen” pattern in paragangliomas, is characterized by loose cell clusters surrounded by thin vascular channels. This cytological feature is uncommon but significant for diagnosis. Identifying this pattern aids in early, optimal surgical planning, crucial for managing head and neck tumors such as carotid body tumors and extra-adrenal paragangliomas. 14 These tumors are generally benign, with malignant cases accounting for approximately 10% of instances. Familial links are well-documented, as over 10% of paragangliomas arise from genetic mutations, particularly involving 3 of the 4 succinate dehydrogenase subunit genes (SDHB, SDHC, and SDHD). This genetic basis notably heightens the likelihood of multiple tumors, with familial cases showing up to an 80% incidence of multicentricity, compared to a 10% to 20% occurrence in sporadic cases. The genetic traits specific to hereditary paragangliomas are thoroughly characterized in the literature.5,6
This case adds to the limited literature on head and neck paragangliomas and highlights the diagnostic complexity associated with tumors in the pterygopalatine fossa. It emphasizes the need for a high index of suspicion for catecholamine-secreting tumors in patients presenting with hypertension and other symptoms of catecholamine excess, even when the mass is located in an atypical region. Future studies should focus on improving diagnostic protocols for head and neck masses, especially in deep anatomical locations such as the pterygopalatine fossa, where radiological characteristics may overlap with other tumor types. Moreover, further investigation into the long-term outcomes of stereotactic radiosurgery versus surgical resection for paragangliomas in this region is warranted.
Conclusion
This case illustrates a rare instance of a catecholamine-secreting paraganglioma located in the pterygopalatine fossa, a site infrequently associated with such tumors. The initial misdiagnosis as chondrosarcoma underscores the diagnostic challenges posed by tumors in deep anatomical regions, where atypical presentations can obscure the true nature of the condition. The effective surgical intervention not only confirmed the diagnosis histologically but also resulted in the immediate resolution of the patient’s symptoms, particularly hypertension. This case highlights the critical importance of maintaining a high index of suspicion for functional paragangliomas in patients exhibiting symptoms of catecholamine excess, even when the tumor’s location deviates from typical patterns. Enhanced awareness and refined diagnostic strategies are essential for improving outcomes in similar cases. Future research should aim to delineate the optimal management approaches for head and neck paragangliomas, particularly regarding the comparative efficacy of radiosurgery and surgical resection in these challenging anatomical locations.
Footnotes
Data Availability Statement
The data that support the findings of this study are available from the author or corresponding author upon reasonable request.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval
Our institution does not require ethical approval for reporting individual cases. Written informed consent was obtained from the patient for publication of this article.