
Abstract
Multifocal head and neck paragangliomas are exceptionally rare. We present a patient with 4 synchronous tumors including a sympathetic chain lesion. This is a case report and literature review conducted from September 2021 to the present. Our 69-year-old male patient presented to the clinic with multifocal paraganglioma involving the right carotid body, right cervical sympathetic trunk, right glomus jugulare, and left glomus tympanicum. After preoperative embolization, successful surgical resection was performed for the right sympathetic trunk and right carotid body tumor. Postoperatively, the patient had a right Horner’s syndrome but a strong voice and intact recurrent laryngeal nerve function. He also had first-bite syndrome and right cranial nerve XII weakness which resolved. Of interest, patient also has a strong family history of paragangliomas: his sister has malignant paragangliomas with lymph node involvement and his mother and nephew have non-malignant paragangliomas. To our knowledge, multifocal tumors including synchronous carotid body, sympathetic chain, glomus jugulare, and glomus tympanicum lesions occurring in 1 person have not been reported until now. As a result of this study, there is new light shed on the treatment and evaluation of patients who present with multifocal paraganglioma involving the sympathetic chain.
Keywords
Introduction
Neoplasms that arise from chemoreceptive tissue extra-adrenally are known as paragangliomas. Only a small minority of all paragangliomas are found in the head and neck, the majority of which are found within the carotid sheath and localized to the carotid body bifurcation. Paragangliomas arising from the cervical sympathetic chain are exceedingly uncommon and are often misattributed as other paragangliomas or schwannomas until surgical resection where they can be properly identified. Multifocal paragangliomas are also rare. In this report, we discuss the exceptionally rare finding of 4 concurrent paragangliomas in a single patient involving the right carotid body, right cervical sympathetic trunk, right glomus jugulare, and left glomus tympanicum. The right cervical sympathetic trunk was the largest of the tumors and was subsequently removed along with the right carotid body tumor.
Case Presentation
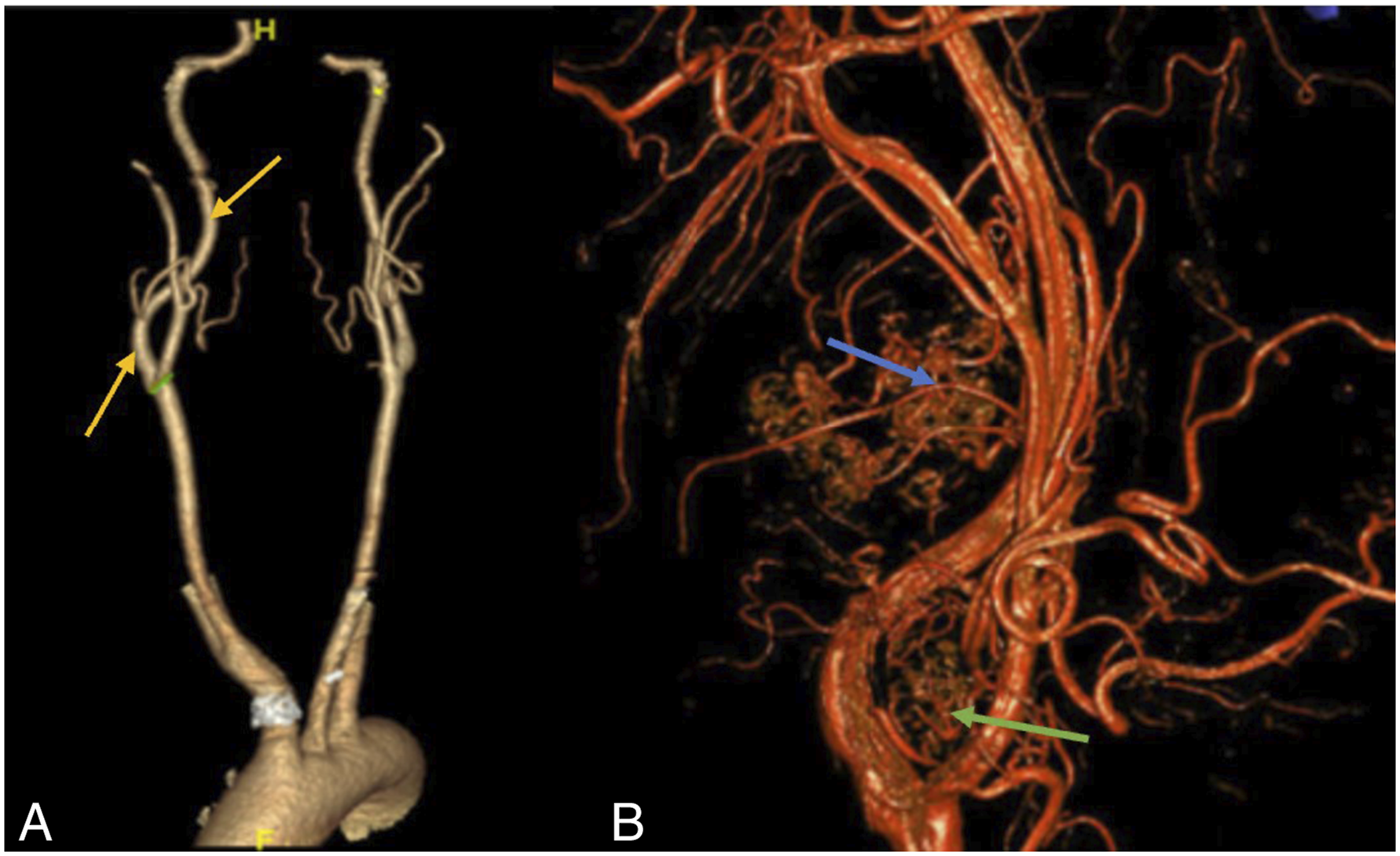
A 69-year-old South African male with a history of Wolff-Parkinson-White syndrome presents with multifocal paragangliomas (Figures 1 and 2). The patient was otherwise asymptomatic and did not complain of hoarseness. Physical examination confirmed palpable right-sided neck masses. Computed tomography angiography (CTA) and carotid duplex scans revealed a highly vascular 1.6 cm right-sided carotid body tumor splaying the internal and external carotid arteries (ICA and ECA, respectively), as well as an additional 3.5 cm right-sided paraganglioma assumed to be a glomus vagale tumor (Figure 2). Preoperative angiogram demonstrated a right glomus jugulare tumor and a left glomus tympanicum lesion. The patient underwent preoperative embolization followed by a right neck dissection with removal of the right carotid body tumor and right glomus vagale; however, the latter was noted to be originating from the sympathetic chain and was completely resected from the parapharyngeal space. Postoperatively, the patient had a right Horner’s syndrome with eyelid ptosis but a strong voice and intact recurrent laryngeal nerve function. He also had first-bite syndrome and right cranial nerve XII weakness. Final pathology confirmed paraganglioma for both resected tumors but no evidence of malignancy. On last follow up, his hypoglossal nerve dysfunction resolved. Of interest, patient also has a strong family history of paragangliomas: his sister has malignant paragangliomas with lymph node involvement and his mother and nephew have non-malignant paragangliomas. (A) and (B) coronal CTA neck: right carotid body tumor (pink arrow) and right sympathetic chain tumor (orange arrow). (C) Sagittal CTA neck: right carotid body tumor (red star) and sympathetic chain tumor (yellow star). (A) 3D CTA neck: displaced right carotid artery (yellow arrows). (B) 3D angiogram: highly vascular right cervical sympathetic chain paraganglioma (blue arrow) and highly vascular right carotid body paraganglioma (green arrow).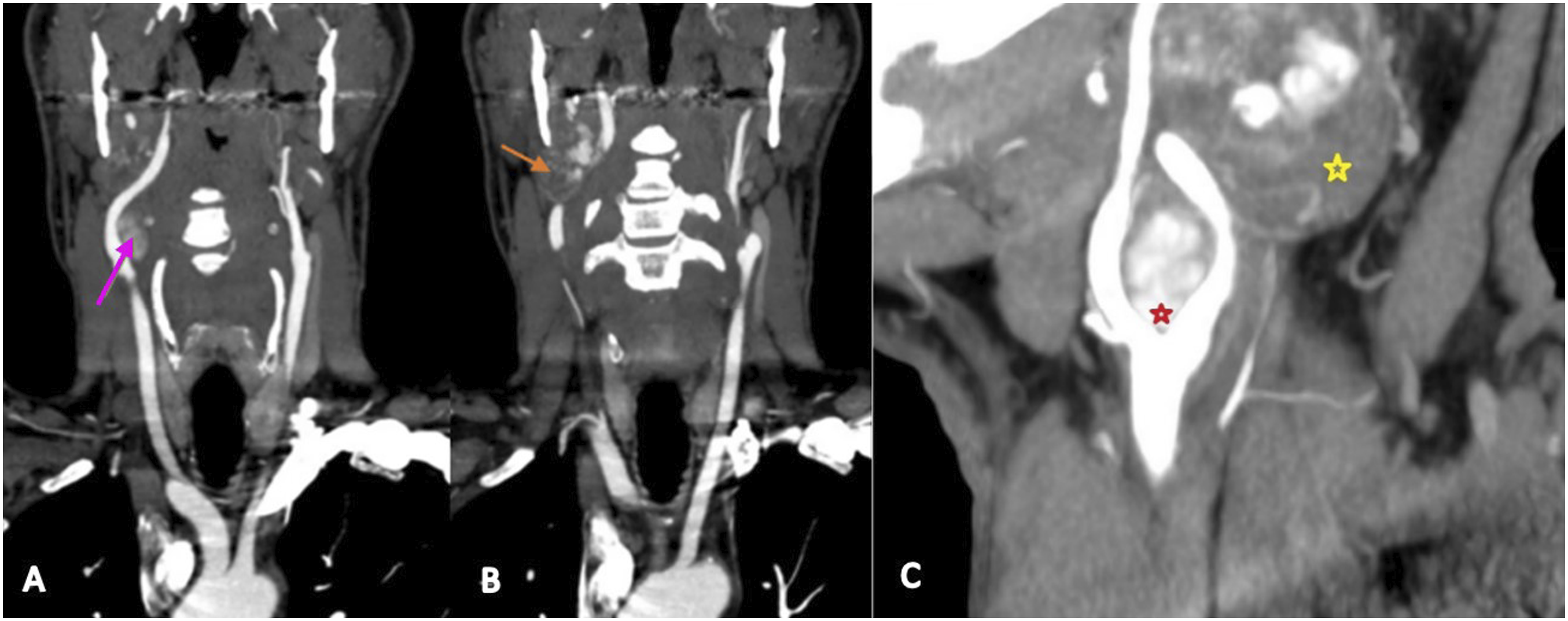
Discussion
Paragangliomas are histologically indistinguishable from their adrenal counterpart—pheochromocytoma—and are only differentiated by anatomic location. Cervical sympathetic chain paragangliomas typically displace the carotid and jugular vessels anterolaterally or laterally. Carotid body paragangliomas are generally located at the carotid bifurcation and splay the ECA anteromedially and the ICA posterolaterally. Generally, they occur in adults between the 3rd and 5th decades of life, and approximately 20% of cases are in the pediatric population. With an overall incidence between 2 and 8 per million and prevalence between 1:2500 and 6500, paragangliomas are exceedingly rare. 1 According to Sharif et al., there are less than 21 cases of cervical sympathetic chain paraganglioma reported in the literature. 2 To our knowledge, multifocal tumors including synchronous carotid body, sympathetic chain, glomus jugulare, and glomus tympanicum lesions occurring in 1 person have not been reported.
The incidence of multiple paragangliomas is approximately 10% of the total patients, but in familial cases, it increases up to 35–50%. 3 The most common presentation of multiple paraganglioma is bilateral carotid body tumors. Inheritance is autosomal dominant for many paraganglioma-predisposing germline mutations, many of which occur in the tumor suppressing succinate dehydrogenase (SDH) genes. Our patient has a strong family history of paragangliomas in several of his first-degree relatives including his mother, sister, and nephew. Any first-degree relative of a mutation carrier should be counseled for genetic testing.
Paragangliomas of the head and neck will commonly present as painless, non-tender, slow growing neck masses, and carotid body tumors will be fixed lesions that do not move in the cranio-caudal direction (Fontaine sign). Over time, symptoms may include hoarseness, vision changes, dysphagia, Horner’s syndrome, and/or other cranial neuropathies. In rare cases, these tumors can synthetize and secrete catecholamines. In those cases, associated symptoms may include hypertension, tachycardia, tremors, and palpitations. Malignant paragangliomas are rare but could result in symptoms of malaise, weight loss, and nausea.
Given the location of the tumor, it is difficult to differentiate cervical sympathetic paraganglioma from other lesions of the neck, such as glomus vagale. Often the distinction is unknown until the time of resection. Ultrasound, CT (Figure 1), and MRI are all useful imaging modalities used to visualize these tumors. Typical appearances on a post-contrast CT include soft tissue density like muscle and bright and rapid enhancement. T1 MRI images include a classic “salt and pepper” appearance and iso- to hypointense compared to muscle. Traditionally, a tumor found medial to the carotid sheath displacing the carotids and jugular vein anterolaterally with no splaying of the internal or external carotid and no separation of the jugular vein and carotids can be considered diagnostic of a sympathetic chain tumor. 4
Histologically, these tumors show a “Zellballen” pattern which consists of well-developed tumor cells that show nest growth and have an intervening stromal component of fibrovascular tissue and peripheral sustentacular cells (Figure 3).
5
Malignancy, however, is determined only by evidence of spread to regional lymph nodes or distant sites. (A) (H&E stain, 100X): Histopathologic features of the paraganglioma. Epithelioid cells with eosinophilic to clear cytoplasm arranged in nests (Zellballen pattern) in a background of hyalinized fibroconnective tissue with ectatic vessels. (B) (H&E stain, 400X): Generally round nuclei with focal pleomorphism; no mitotic activity or necrosis identified.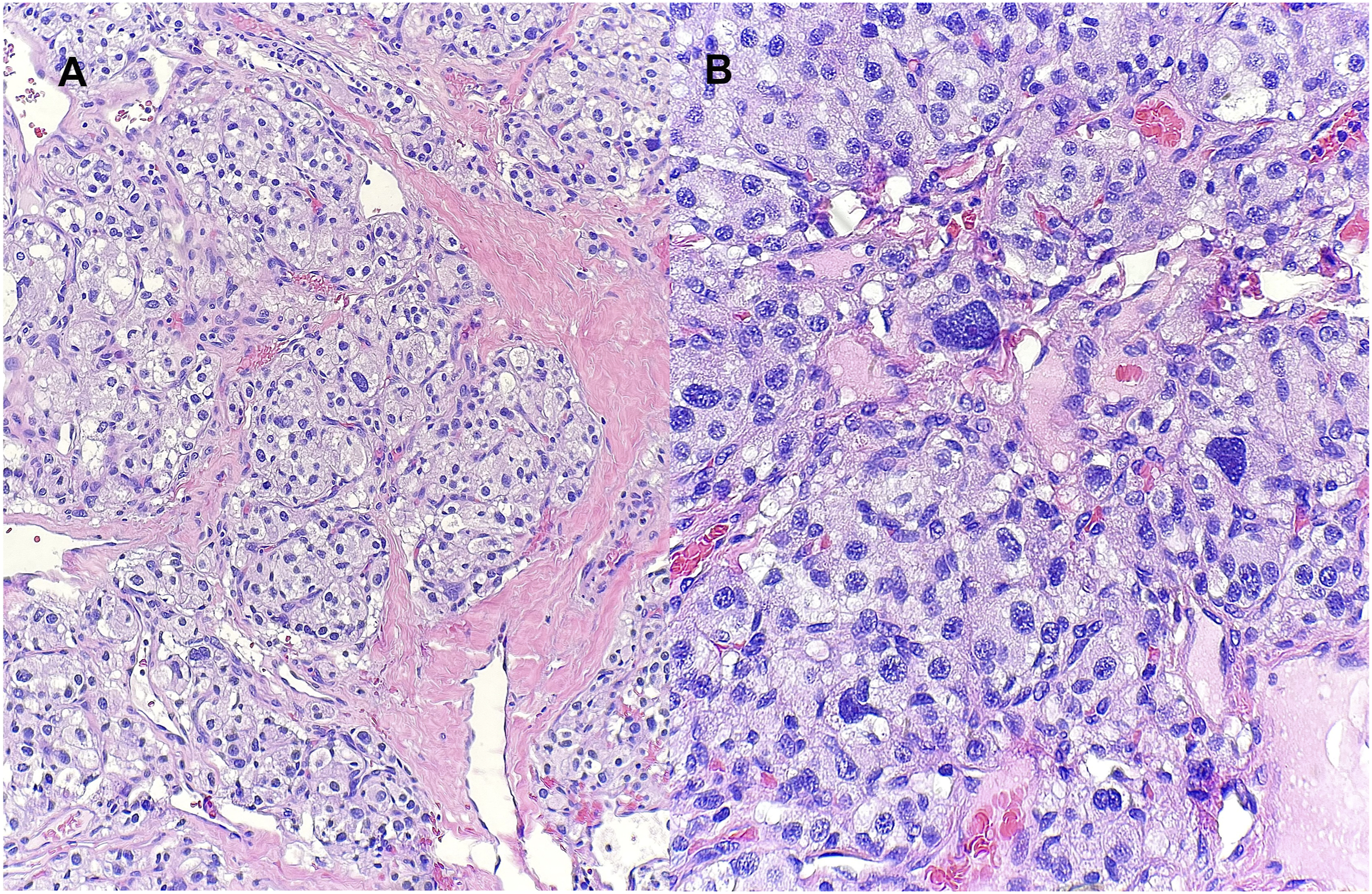
Preoperative embolization followed by surgical extirpation is the main stay for cervical sympathetic chain paragangliomas. Often, parts of the sympathetic chain are taken along with the tumor which can lead to ipsilateral Horner syndrome. Typically, the tumor is dissected in the parapharyngeal plane and great care should be taken to avoid injury to any of the nearby cranial nerves and blood vessels. Incomplete resection is often associated with high recurrence rates, so care must be taken to remove the entirety of the tumor when possible. Non-operative treatment options like radiotherapy are typically reserved for elderly patients, are poor surgical candidates, and individuals where resection could be highly morbid. Radiotherapy may make future resection more difficult due to radiation-induced fibrosis.
Multifocal paraganglioma that includes cervical sympathetic chain origin is a clinical presentation that remains exceedingly uncommon in reported literature. The evaluation and management of such requires special consideration and insight into the unique nature of cervical sympathetic chain paragangliomas.
Footnotes
Author Note
This case report was conducted at Houston Methodist Hospital with full support. There is no funding or financial support to report. As a case report on a singular patient, this report is exempt from IRB approval at our institution.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.