
Abstract
Keywords
Introduction
Over the past few decades, skull base reconstruction techniques have advanced significantly. Reconstruction is a critical aspect of the success of skull base surgeries, as it enables the treatment of more complex pathologies while minimizing the risk of postoperative cerebrospinal fluid leakage. 1 The reconstructive ladder includes a variety of approaches, such as autologous and non-autologous grafts, endonasal pedicled flaps, regional pedicled flaps, and free flaps.2-4 Among these, locally raised vascularized flaps, particularly the nasoseptal flap, are commonly employed when available. However, when local flaps are unavailable or compromised, regional or free flaps may be required.
Pedicled regional flaps, originating from extranasal vessels in the head and neck, serve as important alternatives when local flaps are unavailable or inadequate. These include the pericranial flap, tunneled temporoparietal fascia flap, palatal flap, and others.5,6 It is crucial for skull base surgeons to possess a comprehensive understanding of these secondary options, as they become essential in managing more complex defects or when primary reconstruction options have failed. Additionally, as the complexity of repairable defects continues to grow, the need for alternative approaches becomes increasingly vital in addressing intricate reconstructions.
The use of the platysma myocutaneous flap (PMF) for intraoral reconstruction was first introduced by Futrell in 1978. 7 In this study, we aim to validate the surgical technique and evaluate the feasibility of employing the PMF for skull base reconstruction, utilizing cadaveric specimens in a preclinical setting.
Materials and Methods
This descriptive anatomical study was conducted on 2 fresh human cadavers (4 sides) in the animal lab at the College of Medicine. Ethical approval for the study was obtained from the Institutional Review Board of the College. The cadaveric specimens were arranged and fixed to simulate the intraoperative position of a patient. Various nasal telescopes (4 mm, 0°, and 30° angled views; Karl Storz GmbH, Tuttlingen, Germany; Richard Wolf GmbH, Knittlingen, Germany) were utilized. The study assessed the flap’s size, range of rotation, suitability for covering the anterior skull base and clivus, and the corridor technique for transferring the flap to the skull base.
Surgical Technique
To harvest the flap, a transverse neck incision was made 2 fingerbreadths below the mandible, followed by dissection of the skin and subcutaneous layers in the supraplatysmal plane down to the clavicle. The platysma muscle was sharply transected inferiorly, just above the clavicle. Subplatysmal dissection was then performed laterally, with a 0° endoscope used to assist in visualizing and dissecting the plane. Once the plane was fully developed, the platysma flap was transected vertically from the midline. The facial artery and its proximal branches, including the submental artery, were carefully dissected and preserved to serve as the pedicle for the flap (Figure 1).
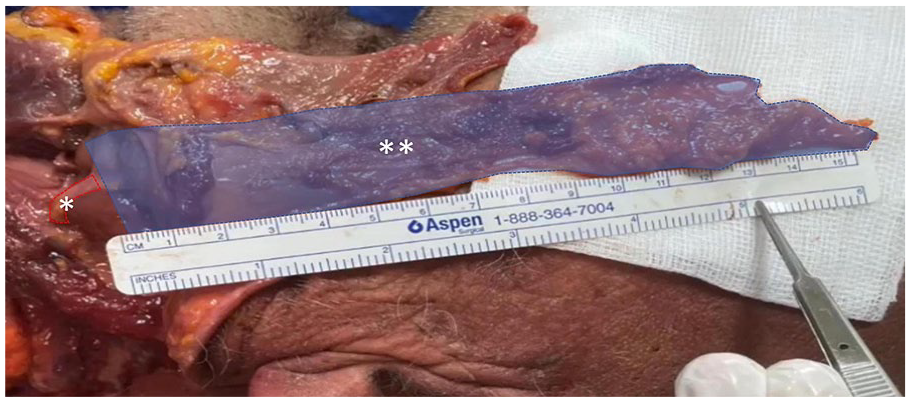
Left-sided platysma flap.
To establish the corridor, an endoscopic endonasal incision was made at the level of the pyriform aperture, exposing the anterior wall of the ipsilateral maxilla. A diamond drill was then used to perform an anterior maxillotomy while preserving the structure of the pyriform aperture. This was followed by an uncinectomy and a wide maxillary antrostomy, after which further dissection was performed to achieve full exposure of the skull base. A subcutaneous facial tunnel was then created using a combination of sharp and finger dissection between the neck and maxilla, facilitating the delivery of the flap into the maxillary sinus (Figure 2; Supplemental Video 1).
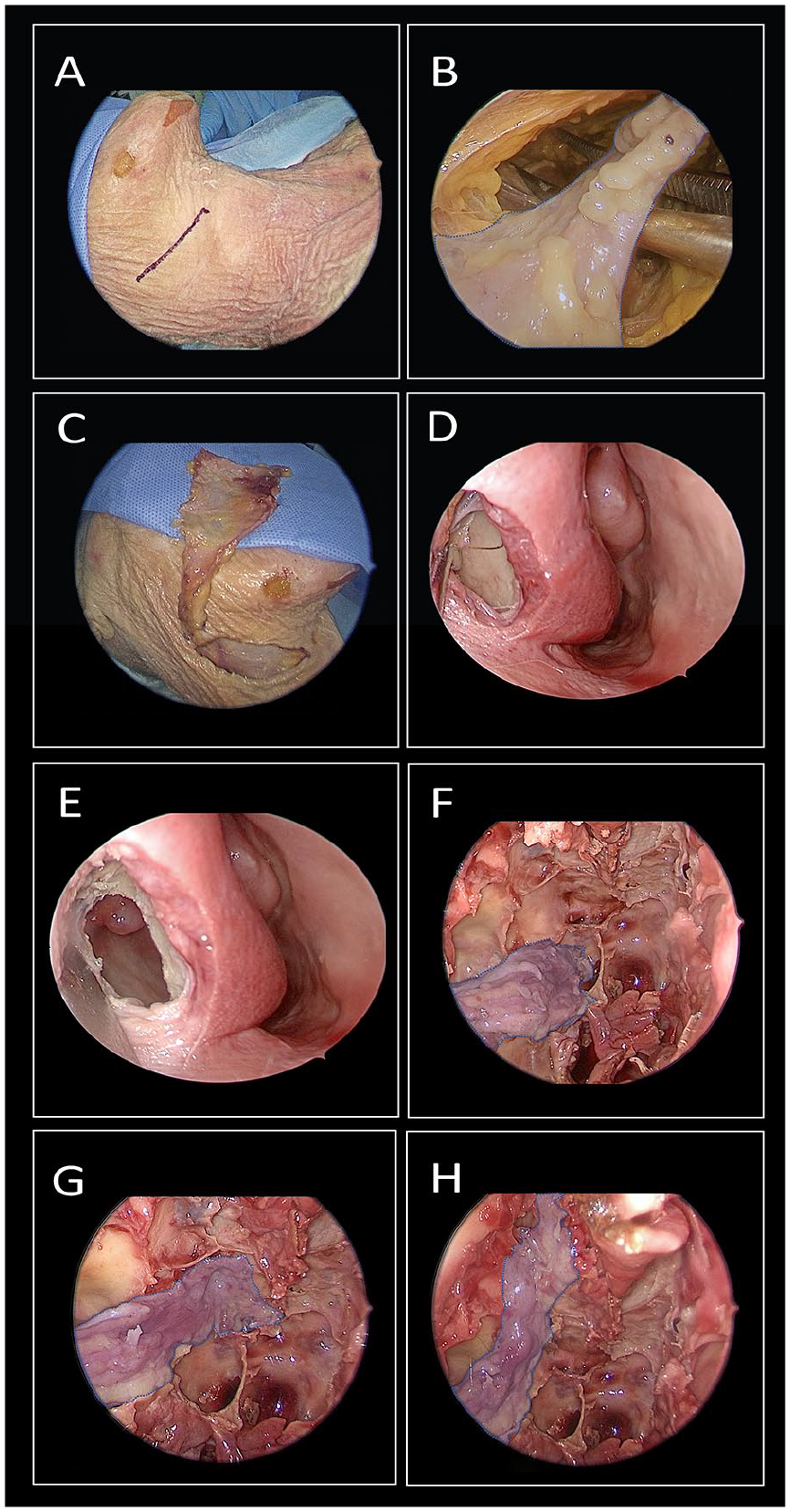
(A-C) Platysma flap harvest. (D, E) Subperiosteal dissection of the anterior maxilla, followed by anterior maxillotomy for flap delivery. (F-H) The flap is shown reaching the ipsilateral carotid artery, ipsilateral planum sphenoidale, and ipsilateral cribriform plate.
Results
The surgical technique was applied to 2 cadavers. A total of 4 flaps were raised, with an average length of approximately 15 cm, measured from the base near the pedicle to the most distal point. The flap was found to adequately cover the ipsilateral carotid artery and the anterior skull base, extending from the level of the planum sphenoidale posteriorly to the cribriform plate anteriorly, reaching up to the frontal recess on the ipsilateral side.
Discussion
As skull base defects become more complex, alternative strategies are essential for managing difficult reconstructions and cases where primary reconstruction has failed. Increasingly, we encounter patients with a history of extensive endonasal surgeries, craniotomies, and radiotherapy, where local or regional flaps are no longer viable, leaving a free flap as the only option. 8 This cadaveric study demonstrates the feasibility of using the PMF as a regional alternative for skull base reconstruction. While well-established for intraoral reconstruction,7,9 the PMF shows promise as a viable option for challenging skull base cases.
The advantages of this method include the readily available PMF, its ease of harvesting, thin and pliable characteristics that make it suitable for three-dimensional reconstruction, and minimal donor site morbidity. 9 Additionally, the size of the flap can be tailored to the defect, with dimensions reaching up to 70 cm². 10 In our study, the primary objective was to measure the maximum length to ensure the flap’s reachability. The PMF demonstrated adequate reach, covering critical areas such as the ipsilateral carotid artery, ipsilateral planum sphenoidale, and ipsilateral cribriform plate.
While these findings highlight the flap’s potential utility for skull base reconstruction, the study has several limitations. The small sample size restricts the ability to generalize the results and assess anatomical variations comprehensively. Additionally, there is a potential risk of flap retraction or movement, which could compromise the reconstruction. To mitigate this risk, appropriate multilayer reconstruction and the use of adequate nasal packing are necessary. Further clinical studies are needed to validate the flap’s safety, effectiveness, and long-term results in routine surgical practice.
Conclusion
Harvesting a PMF is a feasible option for skull base reconstruction, providing adequate coverage for the ipsilateral carotid artery and anterior skull base.
Footnotes
Acknowledgements
Not applicable.
Data Availability Statement
The data that support the findings of this study are available within the article.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Considerations
The study was approved by the IRB committee at the College of Medicine, King, Saud University (No. E-21-6500).
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.