
Abstract
Keywords
Introduction
Chronic rhinosinusitis with nasal polyposis (CRSwNP) is a chronic inflammation of the sinonasal mucosa that lasts for 12 weeks or more, with specific symptoms and clinical signs. This condition seriously interferes with daily activities and compromises quality of life.
Epidemiological data suggest that the general population has an estimated CRSwNP prevalence between 2% and 3% when the guideline-diagnostic criteria are applied.1,2 Additionally, chronic airway diseases, such as bronchial asthma, allergic rhinitis, eosinophilic chronic obstructive pulmonary disease, and chronic rhinosinusitis, share a common pathophysiology characterized by type 2 inflammation. 3 Type 2 inflammation is driven by innate and adaptive immune systems initiated by pollutant, viral, or fungal infection through multiple pathways in which type 2 cytokines are produced at the cellular level, CRSwNP is characterized by eosinophilic inflammation, with elevated levels of type 2 cytokines such as IL-4, IL-5, and IL-13 Additionally, the role of innate lymphoid cells type 2 (ILC2s) has been increasingly recognized in orchestrating the type 2 inflammatory response in CRSwNP. These cytokines, as well as other inflammatory mediators, have a range of roles including IgE production, mast cell degradation, goblet cells hyperplasia, barrier dysfunction, tissue remodeling, eosinophil trafficking to the tissue, and microbiome alteration. 4 However, research on chronic rhinosinusitis (CRS) has revealed that patients with type 2 inflammation tend to be resistant to current therapies, with a high recurrence rate compared with other types of CRS. 2 Hence, understanding the disease pathophysiology and exploring possible new treatment options are crucial for such cases.
Recently, the role of vitamin D in the development of allergic diseases, including CRSwNP, has attracted considerable attention. Vitamin D has been shown to have immunomodulatory effects and is essential for the control of several immune cells, including T cells and dendritic cells, 5 as well as reducing inflammation through multiple mechanisms, as it affects the innate and adaptive immune systems by switching the T-helper 1 (Th1)/Th17 response to a Th2/Treg less inflammatory profile. 6 Additionally, it reduces the production of multiple pro-inflammatory markers such as tumor necrosis factor α (TNF- α), and interferon-gamma (INF-g) in vitro. 7
Additionally, studies suggest that vitamin D affects the innate and adaptive immune systems, as well as structural cells in the respiratory tract. Moreover, insufficient levels of vitamin D can intensify inflammation, whereas supplementation can reduce these inflammatory effects.5,8
Therefore, this study aimed to investigate the relationship between serum vitamin D levels and the severity of CRSwNP. The primary objective was to evaluate the correlation between the disease severity, determined through endoscopic evaluations, imaging, patient-reported outcome measures (SNOT 22), absolute eosinophilic count, and vitamin D levels. The secondary objective was to determine the prevalence of vitamin D deficiency in patients with CRSwNP.
Methods
Informed Consent and Ethics Committee Review Approval
This study was approved by the Institutional Review Board of King Saud University Medical City (No. E-22-7287), and informed consent was obtained prior to the study commencement.
Patients
We interviewed patients with uncontrolled CRSwNP between November 2022 and February 2024 who failed maximum medical management and were scheduled to undergo elective endoscopic sinus surgery. During patients’ clinic visits, baseline information such as age, sex, cigarette smoking, medical comorbidities, weight, height, and BMI were gathered through a structured survey administered by trained personnel. Subsequently, additional information was collected regarding nasal symptoms such as nasal congestion/obstruction, nasal discharge (anterior rhinorrhea or postnasal drip), facial pain or pressure, and loss of smell persisting for >3 months. Residents/fellows simultaneously physically examined patients aged ≥ 18 years using a 3 mm, 0° rigid nasal endoscope. Physical examinations and questionnaires were completed to ensure that every patient satisfied the European Position Paper on Rhinosinusitis and Nasal Polyps (EPOS 2020) criteria for CRSwNP diagnosis. 2
We excluded patients with other forms of secondary CRS and fungal rhinosinusitis, those diagnosed with CRS without nasal polyps and those who used medications that may affect vitamin D levels (such as systemic corticosteroids and vitamin D supplements). The endoscopic total Nasal Polyp score, 9 the Lund-Mackay score, 10 the SNOT-22 scoring system, 11 and absolute eosinophilic count were used to assess CRSwNP severity.
Vitamin D Measurement
An immunoassay kit (Roche e801; Electrochemilumine-scence, Germany) was used to collect blood samples and measure serum 25-hydroxyvitamin D (25D) levels. Patients were divided into 3 groups based on their serum 25D levels as defined by The Endocrine Society: deficient, for levels < 20 ng/mL (50 nmol/L), insufficient, for levels ranging from 20 to 29.9 ng/mL (50-74 nmol/L), and sufficient, for levels > 30 ng/mL (75 nmol/L). 12
Serum Eosinophils
Flow cytometry (Xn 9000; Sysmex, Kobe, Japan) was used to quantify the absolute eosinophil count, expressed as cells per liter (L).
Demographic Characteristics
The association between serum 25D levels and demographic factors was analyzed. These factors include clinically-relevant sociodemographic and medical factors such as sex, age, smoking status, height, weight, body mass index (BMI), activity level, bronchial asthma, and allergic rhinitis. Age, height, weight, and BMI were treated as numerical variables, whereas the remaining factors were considered categorical variables. All variables were defined based on the responses to the questionnaire.
Statistical Analysis
Statistical analyses were performed using IBM SPSS Version 26. Clinical and demographic data are presented as means, standard deviations, frequencies, and percentages. Normality distribution guided Pearson’s or Spearman’s correlation tests were used to investigate the relationship between serum 25D levels and several variables, including the total nasal polyp score, LM score, the SNOT-22, absolute eosinophil count, age, height, weight, and BMI. Statistical significance was set at P = .05.
Results
We analyzed baseline data from 104 individuals with an average age of 42.09 ± 13.3 years and mean BMI of 27.74 ± 6.2. Most of the patients were men (63.5%).
Comorbidities (including asthma, diabetes, and hypertension) and smoking habits of the participants are shown in Table 1.
Patients’ Demographic Characteristics, Continuous Variables, Dichotomous Variables.
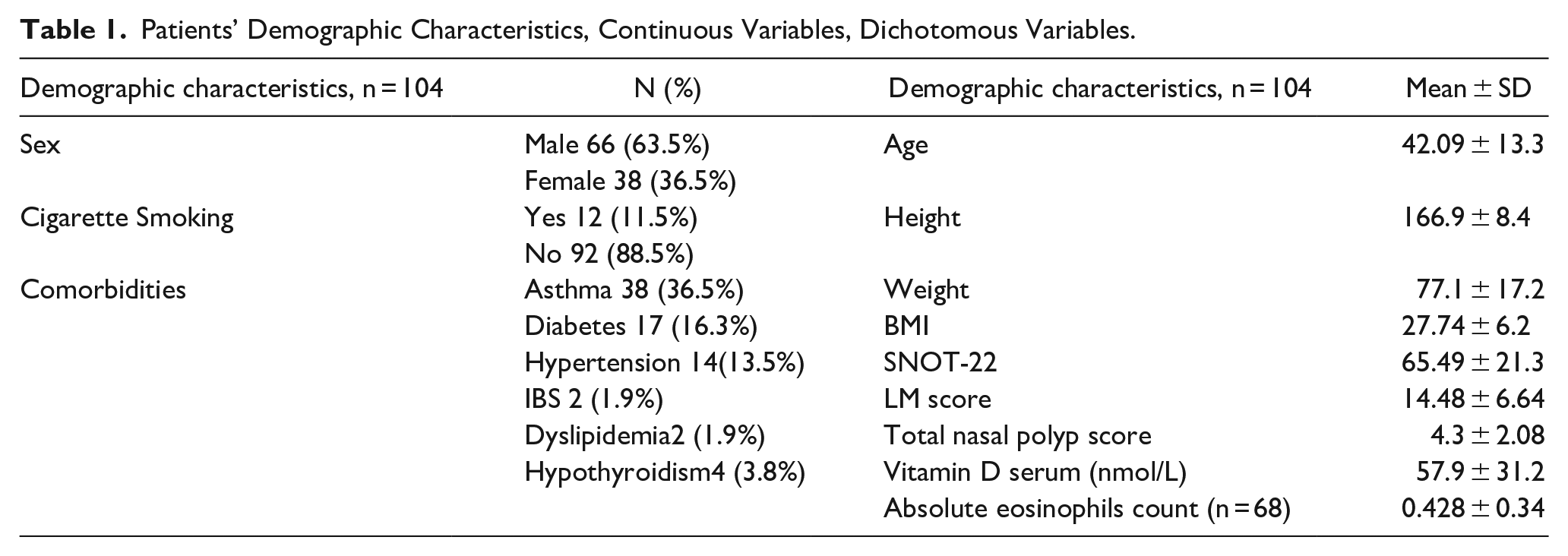
The mean SNOT-22 score was 65.49 ± 21.3, mean LM score was 14.48 ± 6.64, mean total polyp score was 4.3 ± 2.08, and absolute eosinophil mean count (n = 68) was 0.428 ± 0.34 (Table 1).
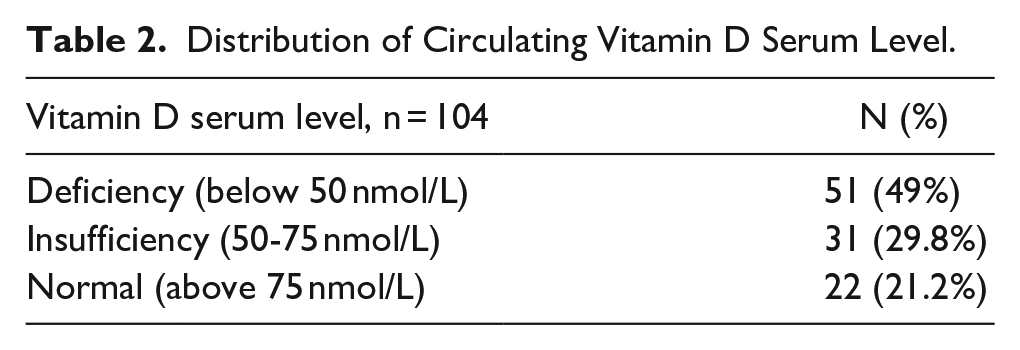
Furthermore, vitamin D serum levels among all the patients had a mean value of 57.9 ± 31.2 nmol/L. Among the 104 patients, 49% were deficient (<50 nmol/L), 29.8% had an insufficiency (50-75 nmol/L), and 21.2% were within the normal range (>75 nmol/L) (Table 2).
Distribution of Circulating Vitamin D Serum Level.
Additionally, we explored the correlations between serum vitamin D levels and various variables such as the total nasal polyp score (r = −.264, P = .007) as well as the LM score (r = −.210, P = .032), which showed a significant negative correlation (Figure 1). In contrast, significant correlations were not observed between serum vitamin D levels and the SNOT-22 score, absolute eosinophil count (Figure 2), age, height, weight, or BMI (Table 3).
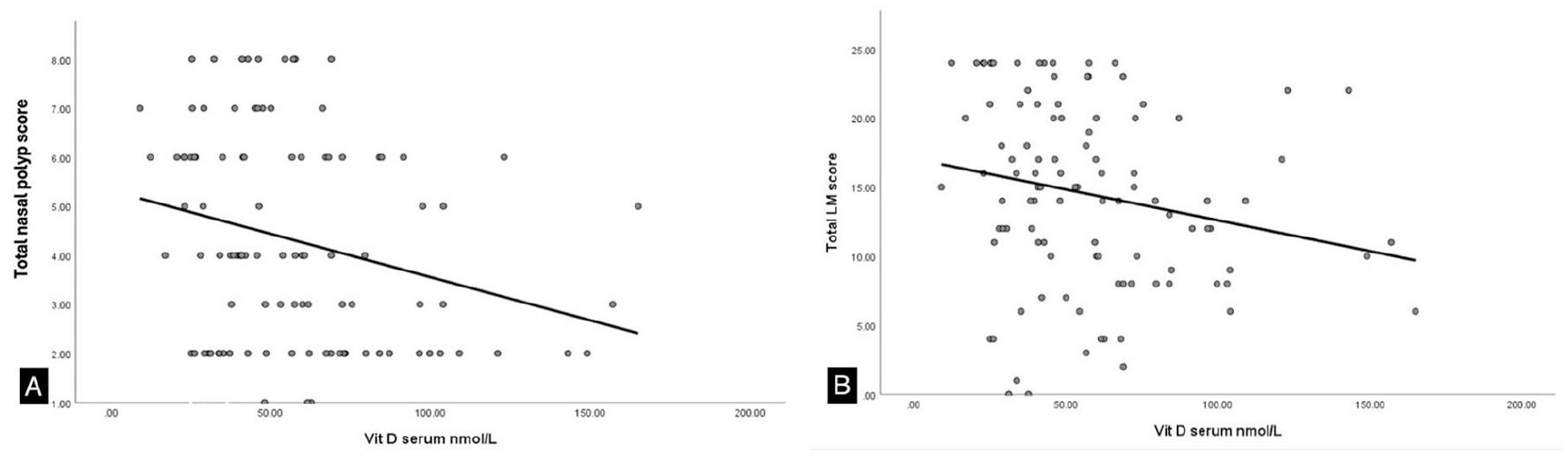
(A) Relationship between the total nasal polyp score and the serum vitamin D level. (B) Relationship between the LMS and the serum vitamin D level.
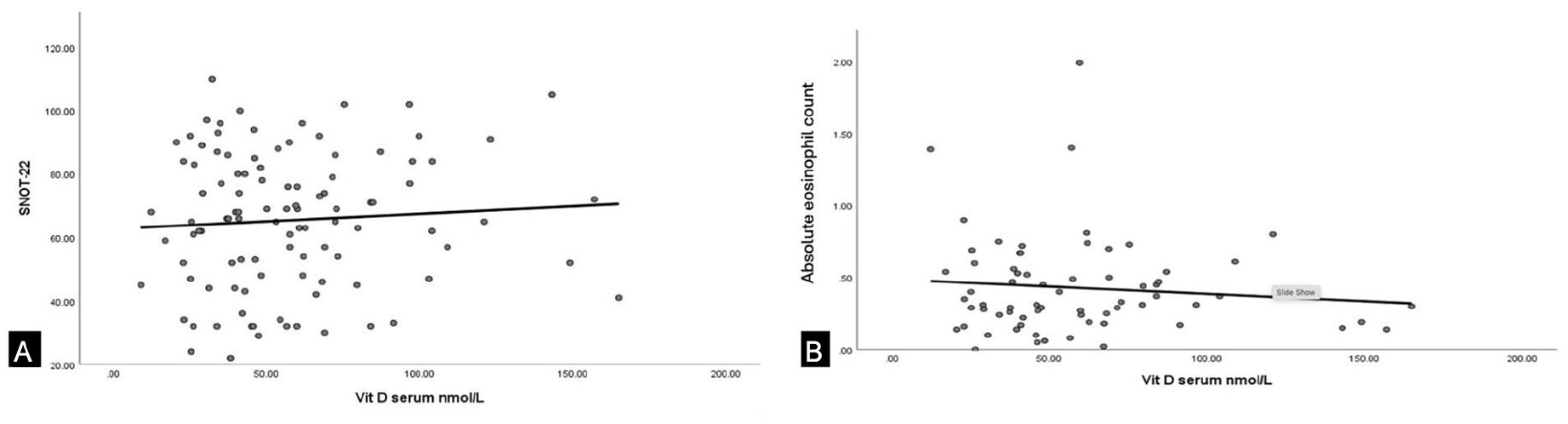
(A) Relationship between the SNOT-22 and the serum vitamin D level. (B) Relationship between the absolute eosinophils count eosinophils count and the serum vitamin D level.
Correlation Between Serum Vitamin D Level and Different Variables.
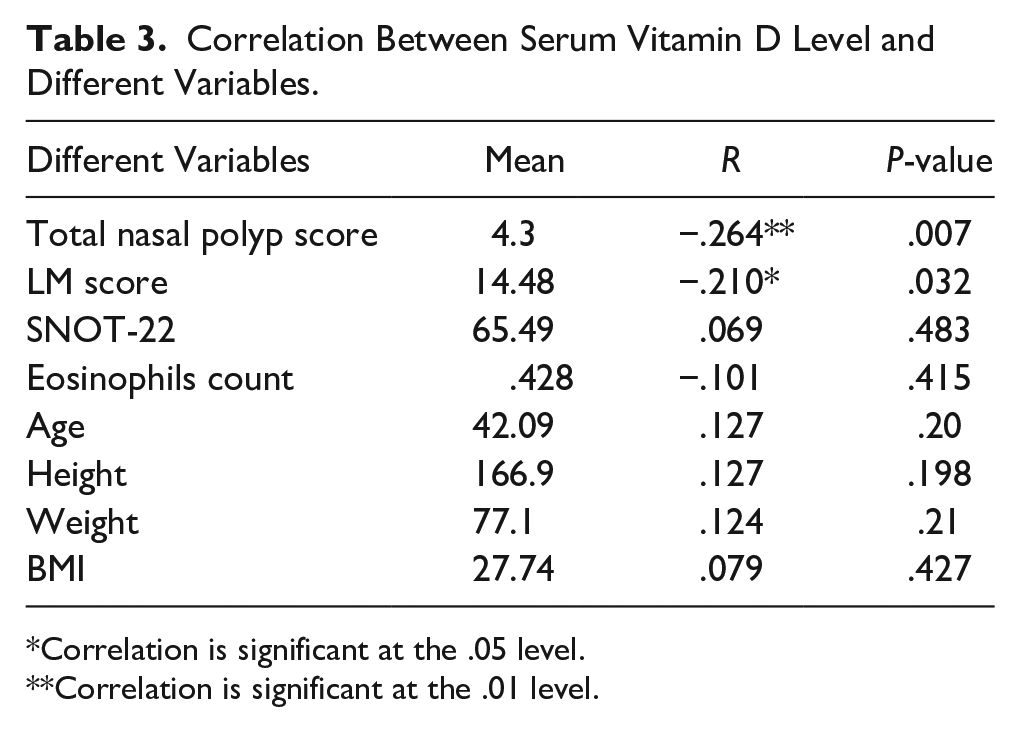
Correlation is significant at the .05 level.
Correlation is significant at the .01 level.
Discussion
CRS commonly occurs because of the complex interactions between the immune system and microbiota in the mucosal lining of the sinuses and nasal passages. The increased formation of microbiome colonies and subsequent immune system responses are most likely owing to local defects in innate and adaptive immunity.13,14 25-dihydroxyvitamin D3 reduces inflammation through multiple mechanisms, as it affects the innate and adaptive immune systems by switching the T-helper 1 (Th1)/Th17 response to a Th2/Treg less inflammatory profile. 6 Additionally, it reduces the production of multiple pro-inflammatory markers such as tumor necrosis factor α (TNF- α), and interferon-gamma (INF-g) in vitro. 7 The type 2 immune response is characterized by elevated levels of interleukin (IL)-4, IL-5, IgE, Staphylococcus aureus enterotoxin-specific (SE)-IgE, and eosinophil cationic protein (ECP), accompanied by elevation of eosinophils in the blood and mucosa in CRSwNP. 15 Moreover, eosinophilic type 2 inflammation in CRSwNP is associated with poor clinical outcomes, recurrence, and reduced olfaction and taste.15,16 The cure in this condition is rare and the current strategies focus on control and remission to enhance patient quality of life and reduce the disease burden.17,18
Although extensive research has been conducted on the involvement of vitamin D in the development of immunological illnesses such as inflammatory bowel disease and psoriasis, its role in CRS is not well established. Therefore, in this study, we investigated the relationship between serum vitamin D levels and CRSwNP severity, contributing to the growing body of evidence suggesting a role for vitamin D in the pathophysiology of CRSwNP.
However, the present study is among the few studies that have investigated the relationship between the severity of CRSwNP and serum vitamin D levels in a Middle Eastern population. Moreover, even though vitamin D deficiency is a global issue, it is particularly widespread in Middle Eastern countries, as in the present study setting (Saudi Arabia).19,20 Studies have shown that the prevalence of vitamin D deficiency in Saudi Arabia ranges from 72% to 80%, depending on the specific population studied, 19 In comparison with Western nations, where vitamin D deficiency affects approximately 41.6% of the United States population 21 and 40.4% of European populations 22 but are generally lower. Therefore, this could potentially lead to an overestimation of the presumed link, particularly in the absence of a control group.
In a recent meta-analysis that included 8 articles, despite the heterogeneity of their outcome assessment and inclusion criteria, the 8 articles showed a significant association between low-serum vitamin D levels and CRSwNP severity. 23 Moreover, a cross-sectional study in 93 individuals with CRSwNP by Zand et al. 24 showed a negative correlation between serum vitamin D levels and disease severity measured clinically (SNOT-22) and radiologically (LMS).
Similar results have been reported in multiple retrospective studies.25-27 Wang et al. 28 reported a significant inverse association observed between serum vitamin D levels and preoperative.
Eighty-eight patients with CRSwNP were measured clinically using the SNOT-22. However, no statistically-significant association was found between serum vitamin D levels and LMS. 28 Moreover, some authors have found promising results regarding the improvement of disease severity in this group of patients after sinus surgery and vitamin D supplementation.29-31 Our findings are consistent with these studies, and we found that as patients with CRSwNP with low serum vitamin D levels exhibited more severe forms of the disease, as evidenced by radiological staging (LMS) and polyp grading.
These findings align as well with other united airway diseases including bronchial asthma. The systemic impact of vitamin D on immune function may account for its potential influence on both upper and lower respiratory tract conditions. Moreover, a correlation has been identified between low vitamin D levels and an increased rate of asthma exacerbations. 32
Recent research indicates that there is a broader correlation between vitamin D deficiency and type 2 inflammatory conditions, particularly in allergic rhinitis (AR), in addition to CRSwNP. It is important to note that Kajal et al. 33 found that the prevalence of vitamin D deficiency was higher in patients with AR than in controls. Additionally, vitamin D levels were found to be inversely correlated with both symptom severity and essential type 2 inflammatory mediators (IL-4 and IL-13). 33
Additionally, a negative correlation was observed in present study between serum vitamin D levels and absolute eosinophil counts, although this relationship was not statistically significant. However, despite evidence from several studies indicating a correlation between reduced serum vitamin D levels and CRSwNP, contradictory results are still observed among different ethnic groups.25,34-36
Christensen et al. 37 reported no correlation between the nasal symptom score (NSS) and low levels of vitamin D. Nonetheless, a notable correlation was observed between the NSS and the expression of vitamin D receptor genes, indicating that dysregulation of these genes may occur independently of the levels of vitamin D in the blood and contribute to the development of CRS. In terms of vitamin D deficiency and the prevalence of CRS, in the present study, vitamin D mean levels were 57.9 ± 31.2 nmol/L, which is aligned with previously-published studies.24,26,38 Conversely, a study conducted in Korea showed that vitamin D levels in the CRSwNP group were 19.293 ± 7.035 ng/mL, which were higher than those in the control group. 39
Our findings also indicated some significant effects. Primarily, the correlation between low vitamin D levels and increased disease severity indicates that serum vitamin D levels could be used as a supplementary biomarker for assessing the degree of CRSwNP, thus augmenting the value of current diagnostic tools, such as endoscopy and computed tomography scans. Second, our results and those of previous studies imply that vitamin D may have therapeutic value in the treatment of nasal polyp-related chronic rhinosinusitis. Thus, the inverse relationship between vitamin D level and disease severity suggests that vitamin D supplementation may be beneficial. Jiao et al. 31 observed improved symptoms in patients with CRSwNP who received vitamin D supplements. However, more studies, including randomized controlled trials, are needed to confirm whether vitamin D supplements aid CRSwNP management.
In our study, disease severity was holistically assessed using several validated assessment instruments, including the total nasal polyp score, LM score, and SNOT-22. Moreover, our study included possible confounding factors such as demographic features and comorbidities.
Nonetheless, this study has some limitations. The small sample size could limit the statistical strength of determining minute impact sizes. Additionally, the lack of a control group prevented direct comparison of vitamin D levels between patients with CRSwNP and healthy individuals. Furthermore, as this was a single-center study conducted in Saudi Arabia. Therefore, our results may not be relevant to populations with different genetic backgrounds or environmental conditions.
These constraints necessitate alternative approaches for future research. Longitudinal studies are required to evaluate how treatment responses and vitamin D levels affect CRSwNP progression over time. Randomized controlled trials are needed to assess whether vitamin D supplements help prevent or control CRSwNP. Moreover, larger multi-center studies involving different populations would assist in confirming the generalizability of these results and investigating the possible environmental or genetic elements influencing the vitamin D-CRSwNP interaction.
Conclusion
According to our study, vitamin D deficiency or insufficiency is common in patients with CRSwNP. We found that low serum vitamin D levels were negatively correlated with the Lund-Mackay score and the total nasal polyp score, providing additional support for an association between low vitamin D levels and a greater severity of CRSwNP. These preliminary findings point to the potential value of vitamin D assessment in the clinical evaluation and management of CRSwNP. However, further studies are required to completely clarify the nature of this association and to determine whether vitamin D supplements could successfully treat or improve the symptoms of CRSwNP.
Footnotes
Data Availability Statement
The datasets used and/or analyzed from the current study are available from the corresponding author on reasonable request.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Considerations
This study was approved by the Institutional Review Board of King Saud University Medical City, Riyadh (No. E-22-7287), November 09, 2022.
Consent to Participate
Informed consent was obtained prior to study commencement.
Consent for Publication
Informed consent for participation in research and publication was provided by the participants.