
Abstract
Introduction
The nasal region is essential medically and socially because it is portrayed in frontal and midface views. There are several potential origins of nasal abnormalities, such as congenital deformities, severe trauma, or iatrogenic factors. Both primary rhinoplasty and secondary rhinoplasty can concentrate on the nasal alar region, a crucial location that houses vital structures. The size and shape of nasal alar malformations can vary for several reasons; also, some ethnic groups tend to have more noticeable or severe cases of these deformities. It has been difficult for rhinoplasty to repair this broad array of abnormalities. Much work has gone into finding ways to use new surgical procedures for better therapy and cosmetic restoration as they have become available. Studying the nasal alar architecture and the applicable surgical techniques is crucial to effectively curing the condition and restoring its aesthetic value.
Nose aesthetics and functionality are both impacted by anatomical abnormalities.1,2 During the pre-rhinoplasty evaluation, alar retraction and alar-columellar disproportion could be considered an aesthetic defect. Another possible cause of retraction is scarring from past surgeries or a weak nasal valve. A patient’s capacity to breathe may be impaired due to intranasal scarring or a flailing alar sidewall in instances of nasal valve instability. 3
A common consequence of primary rhinoplasty and secondary rhinoplasty is the retraction of the alar rim, also known as notching.4,5 Patients who have never had nasal surgery may also experience deformation or retraction of the alar rim. Most alar rim retraction cases occur because the lateral crura is surgically weakened, mal-positioned, or arched.
Determining the frequency of alar rim retraction is challenging. When planning a rhinoplasty, it is essential to consider alar abnormalities. The alar cartilage is crucial for the external nose shape and the patency of the nostrils. Distortion and rounding of the component caused the most visible nasal abnormalities after partial excision of the nasal alae. This led to flattening of the nostrils and poor definition and patency of the nasal sill. When children have their badly-damaged nasal bones openly reduced, they may experience nasal blockage and base broadening if the alar cartilage is removed in whole or in part. Two types of alar cartilage reconstructions exist: those that necessitate a full-thickness graft and those that can be achieved using cartilage in the surrounding skin, with the original alar rim being either the domes of the alar subunits or aerial flaps.3-5 A free-costal cartilage graft might be utilized when the alar cartilage or skin has sustained significant damage.1-3
A well-proportioned nose that meets the patient’s expectations results from rhinoplasty. The nose is expected to grow and develop acceptably after the initial surgery. So, it is essential to watch for asymmetries or deformities that might develop after surgery if the first procedure was not carried out right or if they happened naturally. Primary rhinoplasty aims to restore facial harmony by making the nose proportional to the rest of the face. Once the fundamentals of the nasal anatomy have been established, the focus can shift to the deformity associated with the projection and rotation of the nose. Nose components include skin, cartilage, soft tissues, and bone, further divided among the dorsum, alar, columella, and nose tip. Inadequate manipulation of one or more nasal components sometimes results in a combination of abnormalities displayed by patients presenting for subsequent rhinoplasty. Possible causes include a lack of knowledge about the required procedures or anatomical factors or an inadequate grasp of those factors. The rhinoplasty surgeon should be well-versed in various procedures for correcting joint alar rim abnormalities, including alar notching, flaring, and columellar retraction. Rhinoplasty might provide more consistent outcomes if modern methods and knowledge of the nose’s anatomy are better utilized.
During rhinoplasty operations, surgeons face particular difficulties in achieving a harmonious blend of form, structure, and function to correct alar abnormalities. However, with thorough preoperative evaluation, exacting surgical planning, and precise execution of procedures to restore alar integrity, these obstacles can be overcome.
We aimed to review cases with alar rim problems during the last 5 years and investigate the efficacy of pull-out sutures on the outcomes.
Materials and Methods
A retrospective study was conducted on patients with alar contour grafting and pull-out suture procedures between 2018 and 2023. Patient records and images, such as retraction or collapse, were evaluated before surgery. The average duration of follow-up after surgery was 26 months, but it may be as long as 5 years. The ethics comity approval was obtained before the study.
Operation Procedure
All cases were operated via the open approach. A trans-columellar incision was made at the narrowest part of the columella to connect the medial ends of the bilateral infra-cartilaginous incisions. The skin was elevated, and the distal osseocartilaginous framework of the nose was exposed. Then, the alar rim was observed, and the source of the abnormality was detected.
Intraoperative evaluation of the alar cartilages determined the graft size for alar contour correction. A width of 1.2 cm and a length of 2.5 cm are the bare minimums needed for alar contour grafts on both sides. To bridge the gap between the alar notching or depression, a typical alar contour graft was planned to be 4 to 6 mm wide and 2.5 cm long (Figures 1–6).
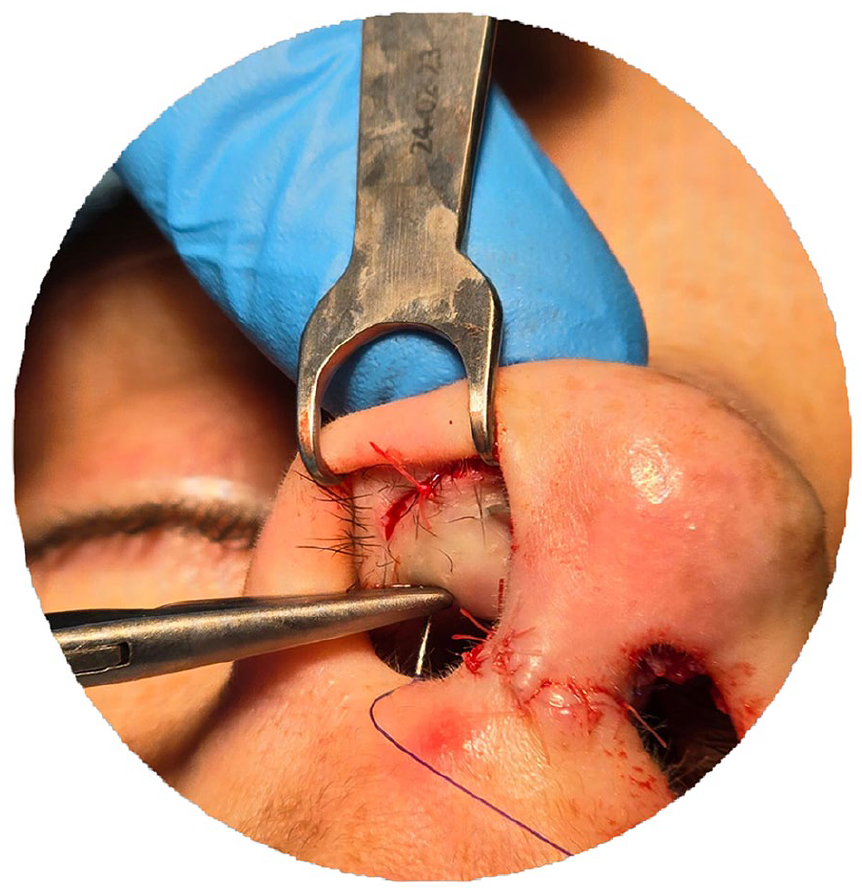
A 4/0 Prolene suture was inserted through the vestibular skin, and the alar cartilage or the graft was inserted along the alar cartilage.
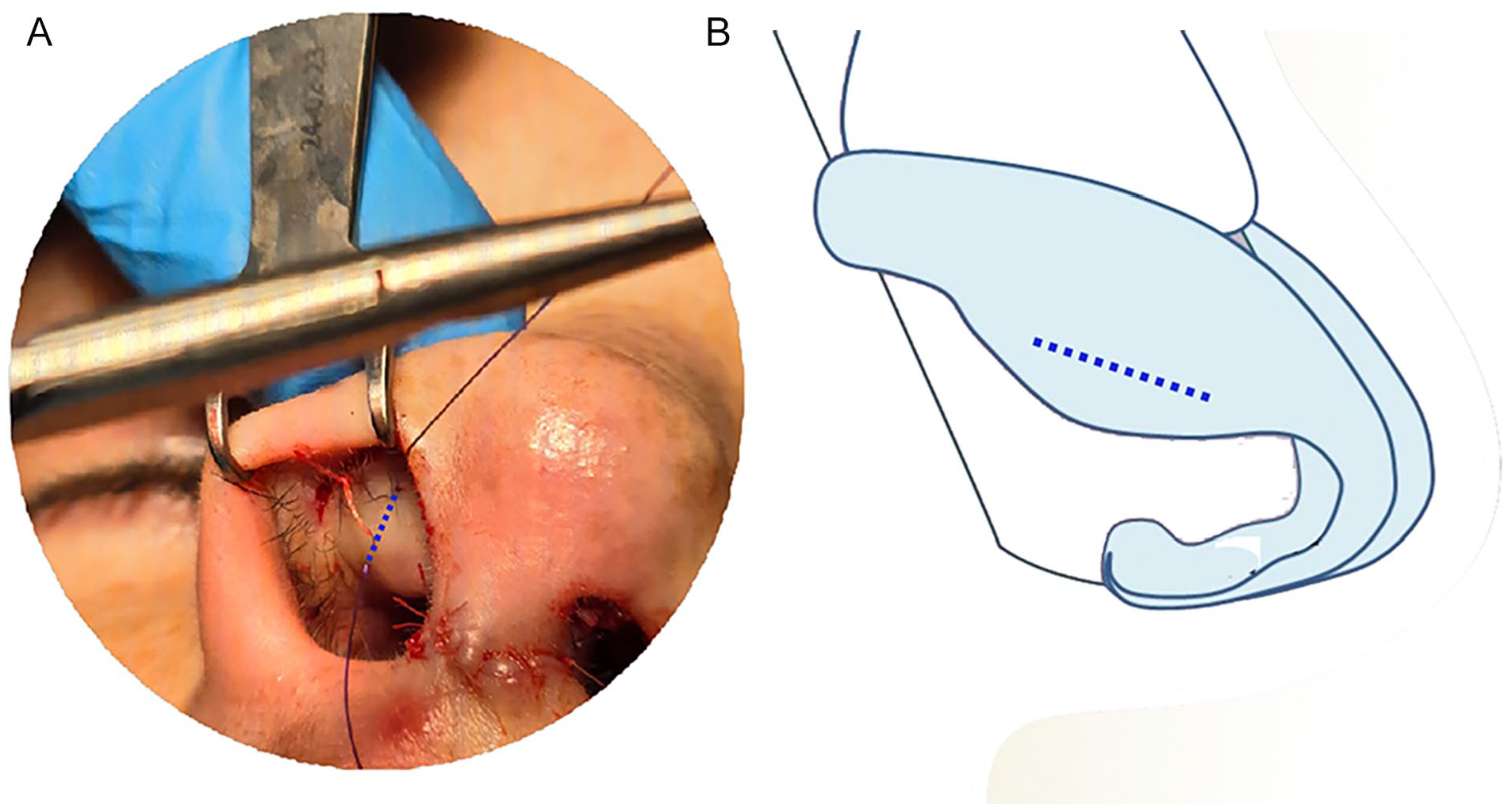
(A, B) The trace of the suture over the vestibular skin and the alar cartilage or the inserted graft.

Pulling out ends of the suture. Both ends of the suture will be fixed to the external splint to pull the graft outward and prevent the shrinking of the vestibular mucosa.

Left: Primary alar retraction lateral view. Right: Postoperative view.

Left: Alar retraction secondary to rhinoplasty frontal view. Right: Postoperative view.

Left: Alar retraction secondary to rhinoplasty lateral view. Right: Postoperative view.
Since it was in the exact surgical location of the septum, it was our preferred graft material. However, auricular cartilage was used if the septum cartilage was not adequate or inaccessible. The amount of cartilage required to span and repair the depressed area determines the final length. Carefully cut a pocket below the infra-cartilaginous incision using long, sharp Stevens’ scissors. The alar contour graft was inserted into this pocket. The dimensions of the alar notched area that needs to be covered by a straight cartilage graft segment are determined by its dimensions. When adequately inserted into this pocket, the notching on the alar rim was covertly fixed. The medial margin is secured with a 5-0 plain suture. A 4/0 Prolene suture was inserted through the vestibular skin, and the graft was inserted to elongate the alar cartilage as the pull-out suture. Then, both ends of the suture were fixed to the external splint to pull the graft outward and prevent the shrinking of the vestibular mucosa.
Preoperative and Postoperative Evaluation and Comparison
The distance between the alar rim and the long axis of the nostril was measured in millimeter both in preoperative and postoperative evaluation and noted.
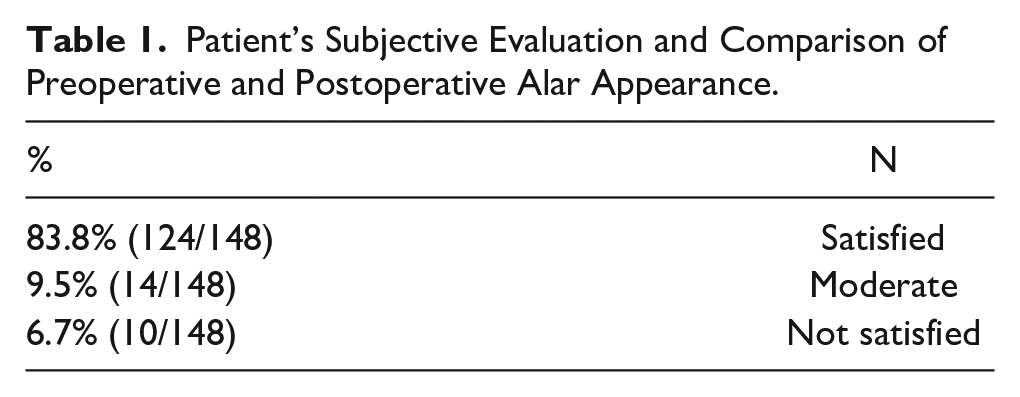
The patient’s subjective evaluation in preoperative and postoperative between 1 and 3 as 1: Satisfied, 2: Moderate, 3: Not Satisfied was done.
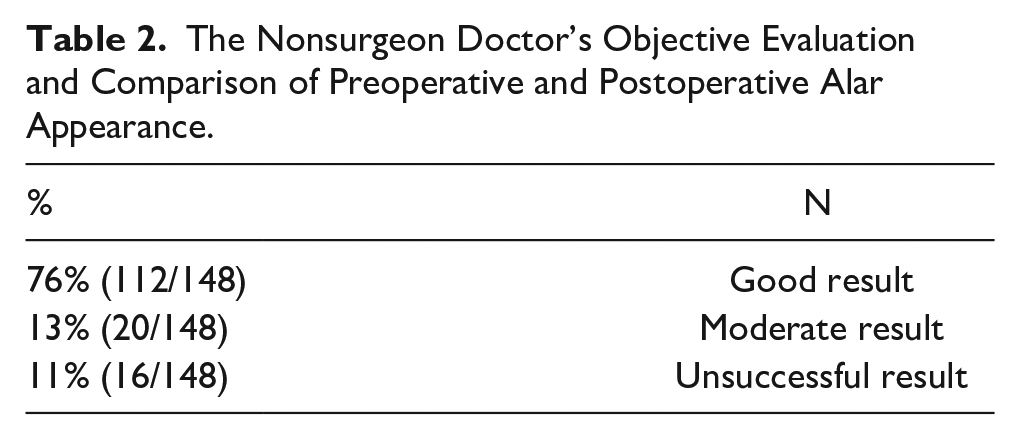
The objective evaluation in preoperative and postoperative between 1 and 3 done by the nonsurgeon doctor. As 1: Good result, 2: Moderate result, 3: Unsuccessful result was done.
Results
The study enrolled 148 patients, 120 females and 28 males, between the ages of 20 and 44. The distance measured between the alar rim and the long axis of the nostril varied between 3 and 5 mm, with an average value of 3.5 mm. Postoperatively, the exact measurement was performed. However, subjective and objective observational evaluation was preferred for comparison instead of calculating the difference in millimeter due to the minimal change in dimension but significant effects on the outcome (Tables 1 and 2). According to patient survey responses, 83.8% of patients (124/148) were satisfied, and 9.5% (14/148) had a moderate response, but 10 cases (6.7%) were not happy with the result.
Patient’s Subjective Evaluation and Comparison of Preoperative and Postoperative Alar Appearance.
The Nonsurgeon Doctor’s Objective Evaluation and Comparison of Preoperative and Postoperative Alar Appearance.
The observational evaluation of the surgeon was close to the patient’s subjective evaluation. We did not have any complications or infections.
Discussion
Many different things can lead to a deformity of the arches. One common reason for recurrence after corrective surgery is when non-dedicated tissue, such as skin, cartilage, or fascia, is interposed or when the defect is not adequately corrected. Some examples of effective treatments for such malformations are silicone prostheses, costal cartilage transplants, and autologous cartilage grafts taken from the nasal septum. It is possible to make the deformity worse following graft implantation if the procedure is not appropriate for the specific subtype of alar deformity. The outcome will be the same if the methodology is suitable, but the graft design needs to be revised. In addition, the graft material can necrosis, and the correction can be lost if the continuity between it and the surrounding tissues becomes slack over time. Besides graft survival, graft displacement due to scar tissue is another critical issue.3,5,6 So, the pull-out suture is crucial to prevent displacement and mucosal shrinkage.
Several surgical approaches can cause an irregular alar rim to develop. Alar recession for alar retraction and wide excision for alar notching are 2 procedures that can lead to under-resection of the alar rim, which can cause this condition. Here, the retraction-type deformity can be caused to move in 1 of 2 ways: vertically toward the face’s midline or in a cephalic manner. An uneven malformation of the joint, commonly seen with a notch on one or both sides, is known as the rat-tail deformity at the alar rim arcus. Overlapping the subdermal flap, which gathers remodeling granulation tissue in the alar rim subderma, might cause the rim to beveled as it causes overhanging round re-bordering. Resurfacing the beveled alar rim or sculpting a subperichondrial graft to fit the alar rim defect are 2 methods for correcting these abnormalities.3,6,7
Alar rim meta-plastics in rhinoplasty have been approached from many angles. The primary emphasis has been reshaping the cartilage at the alar rim, necessitating a sophisticated extensile method.
Due to the dead space and scarring caused by cephalic excisions of alar cartilages, alar retraction is an inevitable consequence of these procedures. Thankfully, the amount of retraction could be more visually and functionally noticeable with cautious excision. Alar rim retraction can also occur after local excision of the nasal sidewall area, such as skin cancer.
The clinical manifestation of alar retraction might occur in more severe cephalic excision. Retraction can be accelerated by removing intranasal mucosa and the skin of the alar vestibular region. The cephalic alar rim can be retracted due to vertical dome division or other cartilage-splitting methods in conjunction with cephalic alar excisions. Notching is encouraged in cases with concurrent excision of alar cartilage and caudal upper lateral cartilages or scroll resection.
Alar arching can occur unintentionally due to improperly-placed interdomal suturing, which can recruit the lateral aspect of the alar cartilage cephalic ally. Caudal alar cartilage excisions are rarely carried out because they induce notchings and abnormal alar shapes.
Too much alar excision, cartilage division, excessive alar sidewall mucosa excision, or excessive alar skin excision can all lead to acquired alar rim retraction. Overarching, frequently lengthy, and plunging alar cartilages or malposition of the alar cartilages are 2 potential causes of primary alar retraction.
A standard nasal architecture may also include alar retraction. The rim might take on an arched and snarled appearance due to the long lateral crura of the alar cartilages. A high arched ala and overdeveloped quadrangular cartilage might further amplify the amount of columellar display. Some tension noses have mild-to-moderate alar notching. It is also possible for alar cartilages positioned cephalically to display notching. On the other hand, some combinations can cause mild-to-moderate alar retraction in noses that otherwise seem ordinary.
Deformities that occur without skin alteration, faults with loss of alar cartilages but preservation of overlaying skin, and deformities combining both degrees are the 3 types of deformities proposed to be treated with alar reconstruction. It is essential to know that different regions have different skin thicknesses and quality to make the chosen treatments work better. The reconstructive approaches are evaluated by comparing the variations in defects, reconstruction methods, and anticipated results. The above mentioned will contribute to advancing reconstructive engineering, leading to more user-friendly and precise methods of repairing nasal alar deformities and other facial and body abnormalities.7,8
Ideally, the flaps should be triangular or parabolic, with an elevation ratio proportional to the incision length. Using the skin adjacent to the defect is preferable to make the most of bigger vessels instead of the skin farther away. While technically feasible, rearranging the tissues immediately surrounding the nose is preferable to flaps from the lower eyelids or forehead. Notable arteries include the superior frontal artery, the zygomatic and masseteric arteries, which exit near the mandible’s angle from beneath the platysma, and the supratrochlear and supra brow arteries, which start at the temples and swiftly travel to the scalp and forehead. The second option can help fix the area around the nose by acting as paranasal flaps. After removing basal cell carcinoma, the resulting alar defect is typically triangular and can be fixed using a median pedicle flap from the other side.7,8
It is crucial to consider the differences in skin texture across the alar, nose, and cheeks when deciding how to use local tissue to fix the defect. Histological examinations of the scalp, temples, and forehead have revealed many dermal ridges punctuated by massive capillaries and follicles. The skin is fragile and has a somewhat rough texture. When it comes to nose and alar repair, the ideal thickness of the skin is the same as that of the normal side of the nose. Because of the dense dermal ridges and follicles in the paranasal region, the scar was typically not visible on histological examinations or grafts taken from that region. Despite being relatively short, the pedicle tended to enlarge following detachment and had a thickness comparable to the anterior nares. Compared to the prior 2 areas, the nasolabial region’s skin is of lower quality, has uneven dermal ridges, and has a more complex vascular supply. Because of the high concentration of tight reticular fibers in the temporal region, the skin is noticeably stiffer than elsewhere. Following detachment, the top dermis atrophys and most hair follicles vanish, making the ridges undetectable. Repairing the alar using tissue from this location does not yield good results.
Overcorrection, under-correction, asymmetries, and surgical side effects are among the complications that might arise from correcting nostril alar deformities. Infection, scarring, leakage of fluid, ulcers, effused blood on the inside of the eye, infiltration of blood into a nearby area, necrosis at the location of the incision, and feelings of remorse are all possible side effects. It should be noted that remorse and scarring are irreversible. A possible irreversible consequence of any surgical operation is regret. Thorough explanations of surgical adverse effects and complications are required. The focus should be on preventing complications, as most adverse effects of nasal alar deformity treatment can be corrected with subsequent surgery.7,8
In conclusion, the level of satisfaction with respiratory and olfactory parameters modified by rhinoplasty is influenced by gender and preoperative satisfaction. Age, treatment-related complaints about the tip region’s appearance, and presurgery happiness all affect how happy a patient is with the aesthetic parts of their nose that have been altered by rhinoplasty. The discussion is on the potential consequences of the second discovery for bettering septorhinoplasty screening, counseling, and satisfaction results.8,9
The goal is always to improve the artistry and skills to an acceptable level since the quality of a given outcome is a mix of performing skill, surgical methods, and artistry. However, patients are still experiencing an increasing number of poor outcomes or complications, and the number of complex cases that test the limitations of existing reconstructive alternatives or implants is on the rise. Creating methods or tools to address these challenges is frequently driven by urgency.9,10
Because secondary alar rim notching is associated with more significant scarring, a longer and somewhat broader alar contour graft is expected to fix the deformity. Crossing the defect and inserting the alar contour graft into a lengthy tunnel just above the alar rim is essential in correcting the deformity. Another advantage of alar contour grafting is correcting collapsed external nasal valves. This happens when the scar tissue is freed from the space between the alar contour graft and the caudal margin of the lateral crura.9,10
Yang and Shi 11 reported that “PLLA facial fillers are a safe and effective treatment for nasal alar retraction, presenting no embolism risk.” Because it is new and less experienced, this treatment needs to be performed with attention. Besides, it needs to be performed on a regular base.
Conclusion
Postoperative alar retraction may occur due to over-resection of the inner mucosa of the nose or the lower lateral cartilages. Cartilage and mucosal grafts are helpful tools to correct this deformity. Pulling the alar rim’s caudal end with a suture prevents the alar mucosa’s shrinkage and the alar rim from retracting. The same suture can also help correct retracted alas.
Footnotes
Acknowledgements
None.
Author Contributions
Oguzhan Oguz: Planning, designing, literature survey, data collection, and active intellectual support. Tarik Yagci: Planning, designing, writing, literature survey, and active intellectual support. Zeynel Ozturk: Planning, designing, literature survey, and active intellectual support.
Availability of Data and Materials
All data for this study is presented in this paper.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethics Approval
Ethics committee approval was taken from Bilecik Seyh Edebali University (Date: December 5, 2023; Number: 8).
Informed Consent
There is no need for informed consent because the data were evaluated retrospectively.