
Abstract
Background:
Despite the growing literature on racial disparities in the utilization of total laryngectomy (TL), and survival following the treatment of laryngeal cancers, there is a paucity of research in TL cohorts evaluating disparities in the immediate postoperative setting.
Methods:
In a national multi-institutional cohort, TL cases between 2010 and 2021 were identified using relevant Current Procedural Terminology (CPT) codes. Logistic regression analyses investigated the association between race/ethnicity and adverse outcomes within 30 days postoperatively.
Results:
This study consisted of 1493 patients who underwent TL with or without radical neck dissection. Black patients underwent free flap and pedicled flap reconstruction more frequently than their counterparts (P = .023) and exhibited a 1.532 times higher odds of surgical complications (P < .001).
Conclusions:
There are increased rates of surgical complications in Black patients undergoing TL. Given the limited oncologic and socioeconomic variables available through National Surgical Quality Improvement Program, future study of disparate postoperative outcomes in this population is recommended.
Introduction
Laryngeal cancer accounts for approximately 20% of all head and neck cancer and is associated with high morbidity and lifelong adverse effects in speech and swallowing. 1 In 2024, there will be approximately 12,650 new diagnoses and 3880 deaths due to laryngeal cancer in the United States. 2 Over the last 2 decades, the incidence of this disease has decreased by 55%, from 5.00 to 2.26 per 100,000 people; however, due to a stable mortality rate, there has been a relative increase in case fatality. 1 Apart from these trends in survival, laryngeal cancer treatment is regarded as highly morbid, with a high prevalence of acute and chronic swallowing dysfunction, 3 tracheostomy and/or feeding tube dependence, 4 and voice impairment5,6 following treatment with primary surgery or chemoradiation. As such, there has been a substantial interest in larynx-preserving treatment modalities (eg, radiation and/or chemotherapy) that improve functionality and quality of life while maintaining comparable oncologic outcomes. 7
While overall survival rates between larynx sparing and preserving modalities are comparable, there is a long history of racial and ethnic disparities in health care that affect laryngeal cancer care including stage at presentation and utilization of total laryngectomy (TL).8,9 Black patients are more likely to present with advanced-stage disease and are more likely to undergo more invasive treatment for laryngeal cancer than other racial or ethnic groups. 8 Additionally, Black patients are more likely to receive primary TL and are more likely to undergo adjuvant radiation therapy following TL.8,9 Despite these trends in aggressive treatment approaches, the 5-year overall survival for Black patients is significantly lower, even when accounting for age, primary treatment, nodal status, and tumor grade. 9 Previous studies have established race as a predictor of hospital length of stay following TL.10,11 However, there has not been a study exploring the impact of race and ethnicity on adverse postoperative outcomes in this population.
Given the consistent evidence of ethnic and racial disparities in laryngeal cancer treatment and TL utilization, we aimed to assess the impact of race and ethnicity on postoperative complications in patients undergoing TL.
Methods
Database
We evaluated 30-day postoperative outcomes for patients undergoing TL across race and ethnicity in a national, multicenter cohort using the National Surgical Quality Improvement Program (NSQIP). NSQIP is a nationally-validated, risk-adjusted, outcome-based program maintained by the American College of Surgeons to measure and improve the quality of surgical care. 12 This retrospective cohort study utilized the NSQIP database from the year 2011 through 2021.
Cohort Selection
Patients undergoing TL from over 600 hospitals across the United States were selected using CPT codes 31360 (TL without neck dissection), 31365 (TL with radical neck dissection), 31390 (pharyngolaryngectomy with radical neck dissection without reconstruction), and 31395 (pharyngolaryngectomy with radical neck dissection with reconstruction). Several exclusion criteria were applied to maintain a cohort with minimal confounders. Only otolaryngology cases were selected due to the inadequate representation of other specialties in the cohort. Similarly, inpatient status was selected for the same reason. Since race was our main variable of interest, cases with missing values, and racial/ethnic categories that represented less than 1% of the total cohort, were excluded to maintain sufficient power. Cases with outliers in body mass index (BMI), operation time, and total hospital length of stay also were removed. Information on cancer stage, prior treatments such as chemoradiation, and disease extent was not available in the NSQIP database.
Variables of Interest
Race/ethnicity was divided into 4 categories: White, Black or African American, Asian, and Hispanic. Other variables included the use of reconstruction modalities, and patients were categorized as receiving primary closure, free flap reconstruction, or pedicled flap reconstruction These were identified using the following CPT codes: 15756, 15757, and 15758 for free flap; 15732, 15733, 15734, 15736, and 15740 for pedicled flap. Cases without pedicled or free flap CPT codes were designated as primary closure (Figure 1).
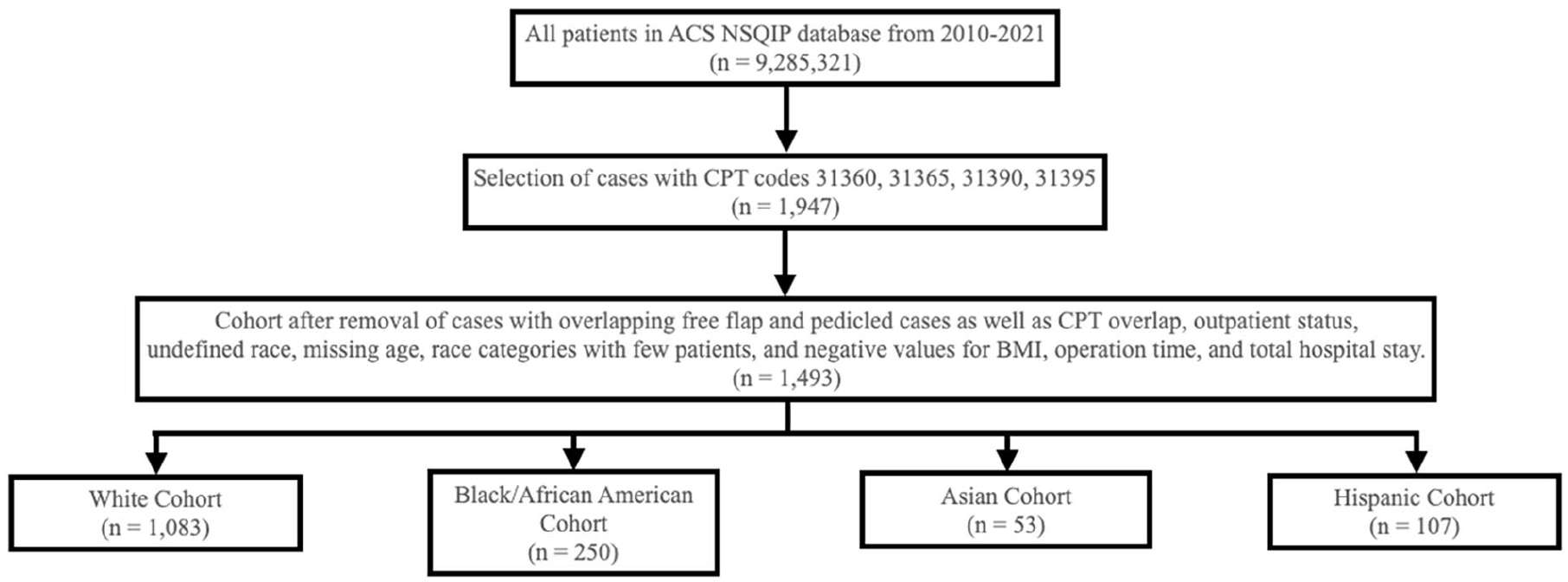
Inclusion and exclusion flowchart.
Outcome variables were created to analyze a broad range of complications. The variable “Any complications” was defined as having any surgical or medical complication. Surgical complications were defined as having at least one of the following less than 30 days post-op: superficial surgical site infection (SSI), deep SSI, organ/space SSI, wound dehiscence, or a blood transfusion within 72 hours from the time when surgery started. Medical complications were defined as having at least one of the following less than 30 days post-op: stroke/cerebrovascular accident (CVA), myocardial infarction, pneumonia, deep vein thrombosis, unplanned intubation, ventilation >48 hours post-op, sepsis, urinary tract infection, pulmonary embolism, septic shock, or cardiac arrest. Reoperation was defined as any unplanned return to the operating room within 30 days of the initial surgery. The binary variable “Still in hospital >30 days” was used to identify hospital stays extending beyond a month. Additionally, the continuous variables “total length of stay” and “operation time” were used to measure the duration of hospitalization and the length of the surgery, respectively.
Statistical Analysis
Univariate analysis was performed to evaluate the variance between race categories for every demographic variable, comorbidity, and outcome. Variables within the univariate analysis that displayed a P value of less than .2 were included as covariates in further multivariable regression analysis. Nonsignificant variables were excluded systematically from the final models. To address potential multicollinearity, all outcome variables (eg, surgical complications, medical complications, operation time, length of stay) were included as covariates in the regression models. For instance, when looking at the variable “surgical complications,” the variable “medical complications” was used as a covariate in the model. This approach was used to identify whether any relationships between outcomes could inflate the results. Binary logistic regression was used to analyze categorical variables, while linear regression was employed for continuous variables such as operation time and total hospital length of stay. Significance was defined as an alpha of less than .05. All statistical analyses were run using the SPSS statistical software version 29.0.0.0 (IBM, Armonk, NY).
Results
Demographics and Co-Morbidities
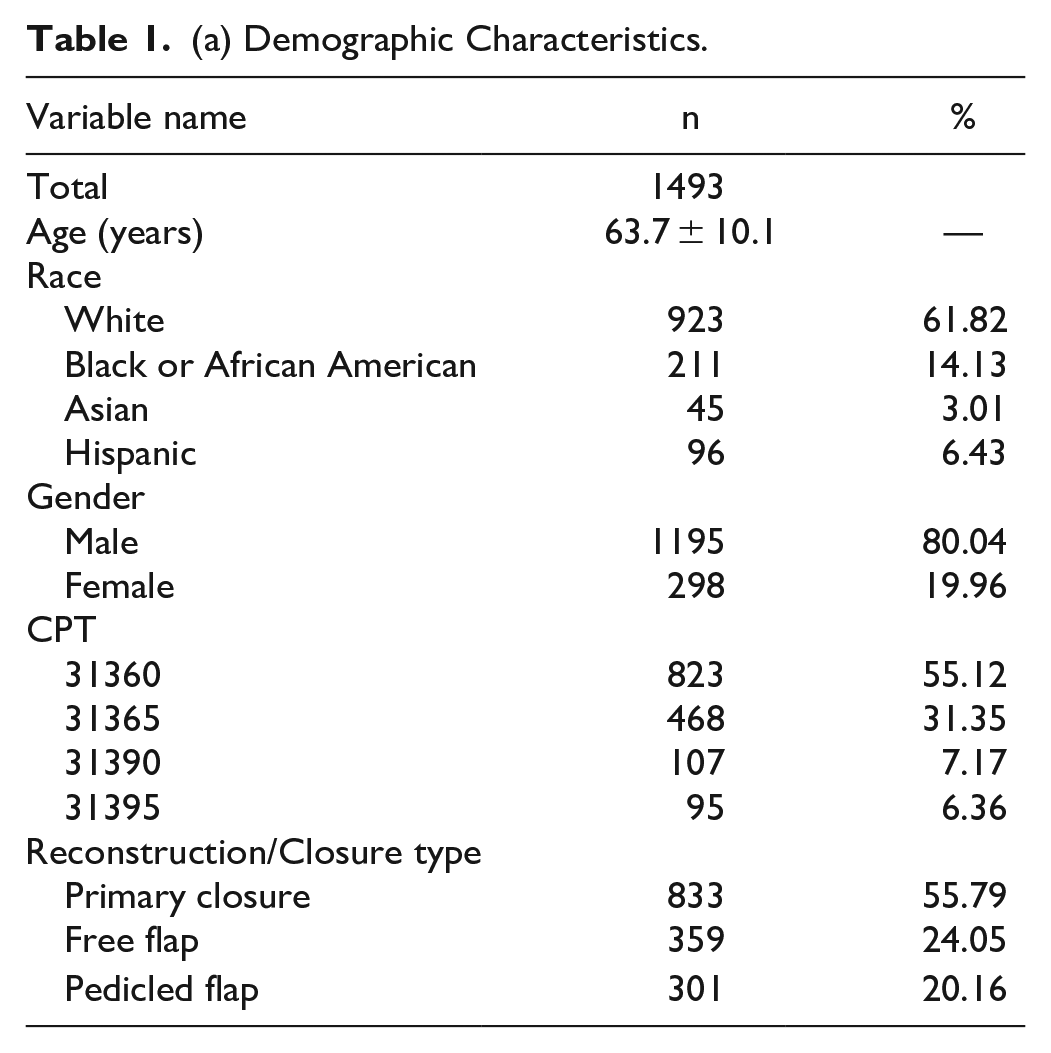
The study included 1493 patients who underwent TL, with the majority being male (80.04%). The average age was 63.7 years (SD = 10.1). The demographic composition of the study cohort was predominantly White (61.82%), followed by Black or African American (14.13%), Hispanic (3.01%), and Asian (6.43%). The most common procedural code was 31360 (TL without neck dissection), accounting for 55.12% of the cases (Table 1(a)).
(a) Demographic Characteristics.
(b) Comorbidity Characteristics.
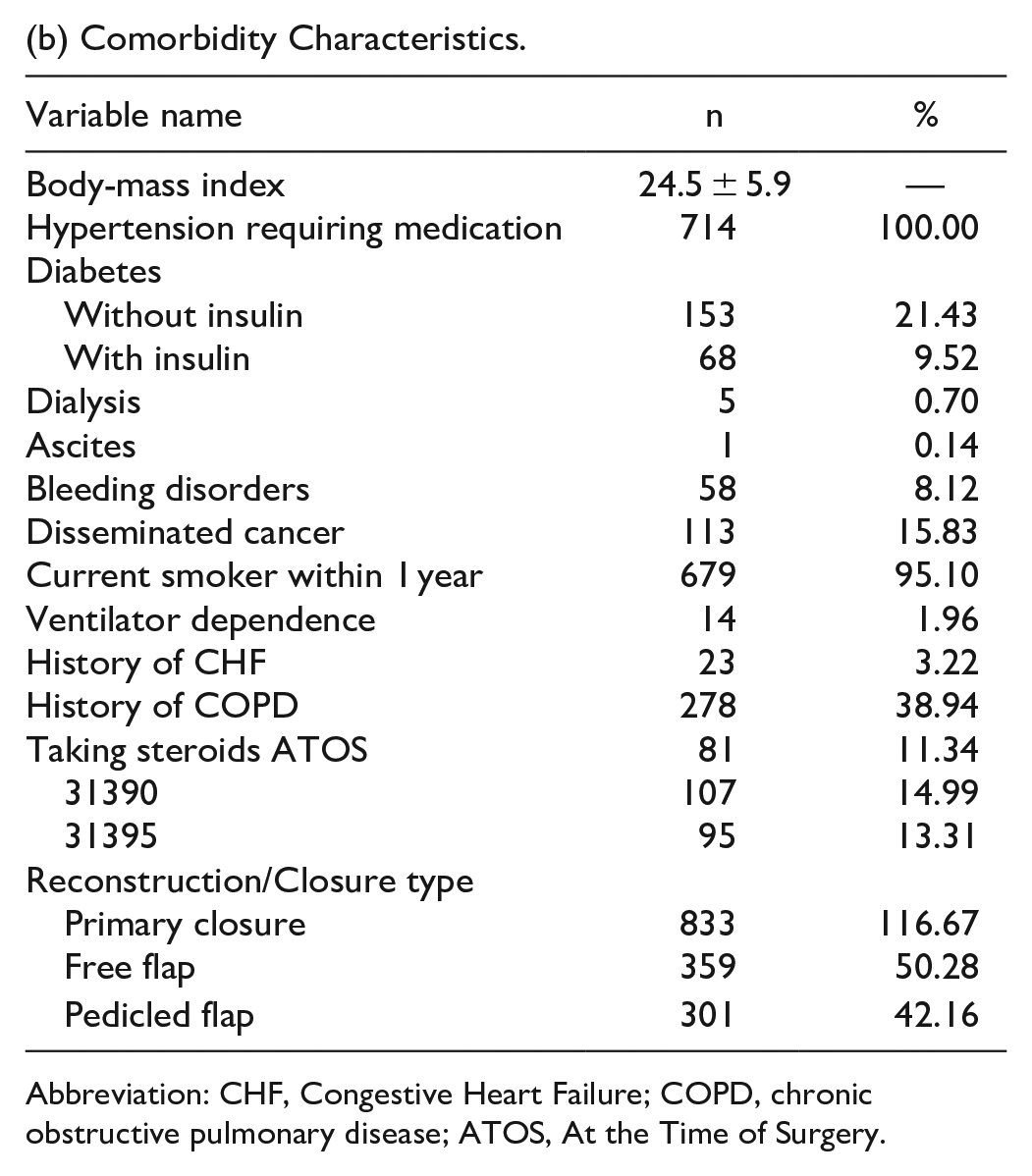
Abbreviation: CHF, Congestive Heart Failure; COPD, chronic obstructive pulmonary disease; ATOS, At the Time of Surgery.
(c) Outcome Descriptives.
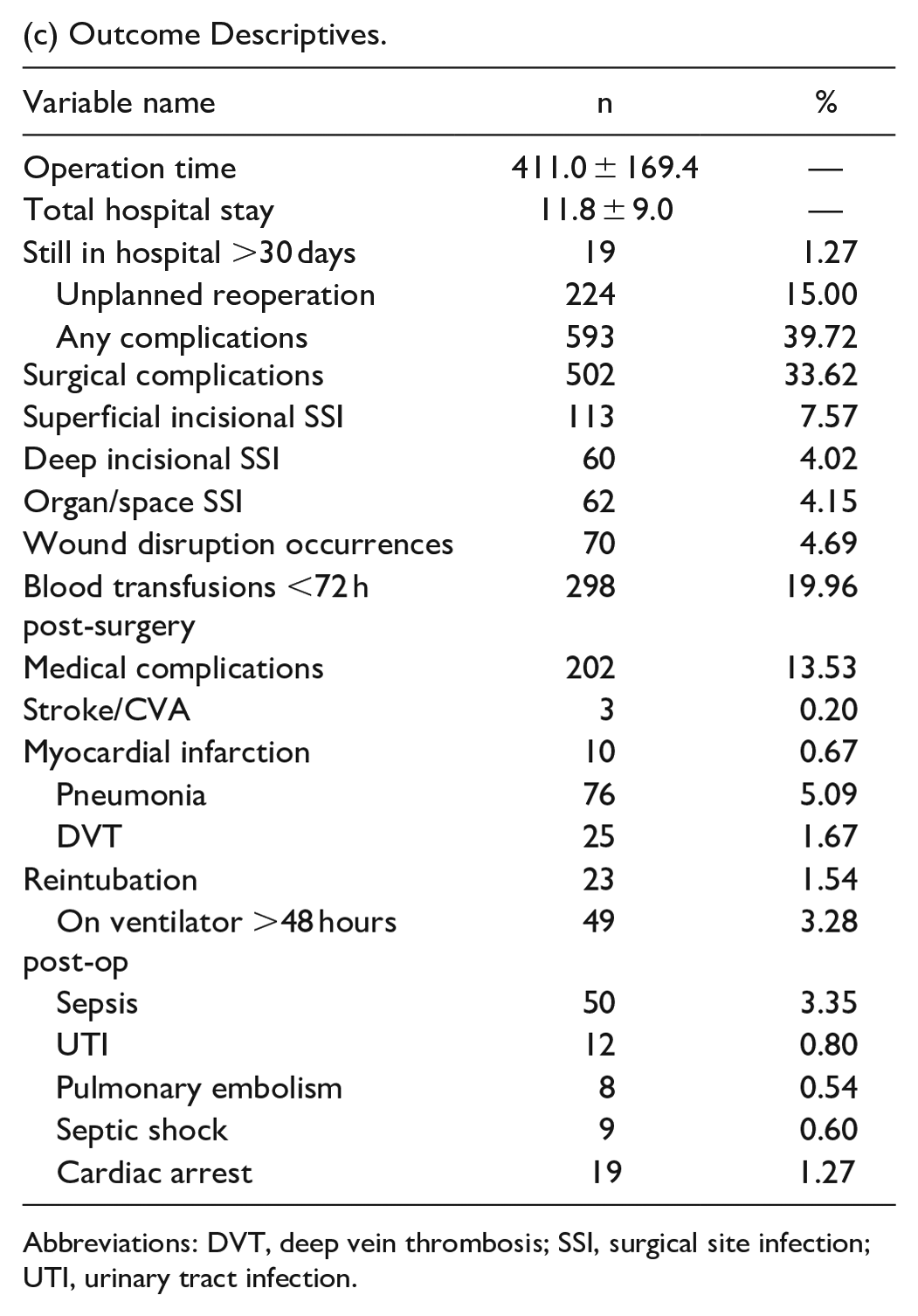
Abbreviations: DVT, deep vein thrombosis; SSI, surgical site infection; UTI, urinary tract infection.
The average BMI was 24.5 (SD = 5.9), and nearly half of the patients (47.82%) had hypertension requiring medication. The cohort had a substantial proportion of current smokers (45.48%) and patients with a history of chronic obstructive pulmonary disease (18.62%). The average operation time was 411 minutes (SD = 169.4), and the average total hospital stay was 11.8 days (SD = 9.0). About 39.72% of patients experienced any complication (surgical or medical), with surgical complications occurring in 33.62% of cases (Table 1(b) and (c)).
Univariate Analysis
Univariate analysis showed significant differences in several variables across racial groups. Hispanic patients had the highest prevalence of primary closure, while Black patients were more likely to have free flap reconstructions; however, stage at the time of TL is unavailable through this dataset. Black patients also had significantly-higher rates of hypertension and were more likely to be current smokers within 1 year than other groups. Differences in postoperative complications were notable, with Black patients experiencing the highest percentage of any complications (48.80%) and surgical complications (43.20%). Blood transfusions within 72 hours post-surgery were most prevalent among Black patients (31.20%) (Table 2). The following variables had a P < .2 on univariate analysis and were therefore included in all of the following regression models: age, race/ethnicity, BMI, smoking status, hypertension, diabetes status, type of surgical reconstruction (primary closure, free flap, pedicled flap), operation time, and total hospital length of stay.
Univariate Analysis of Demographic, Comorbidity and Postoperative Outcome Variables Across Race/Ethnicity.
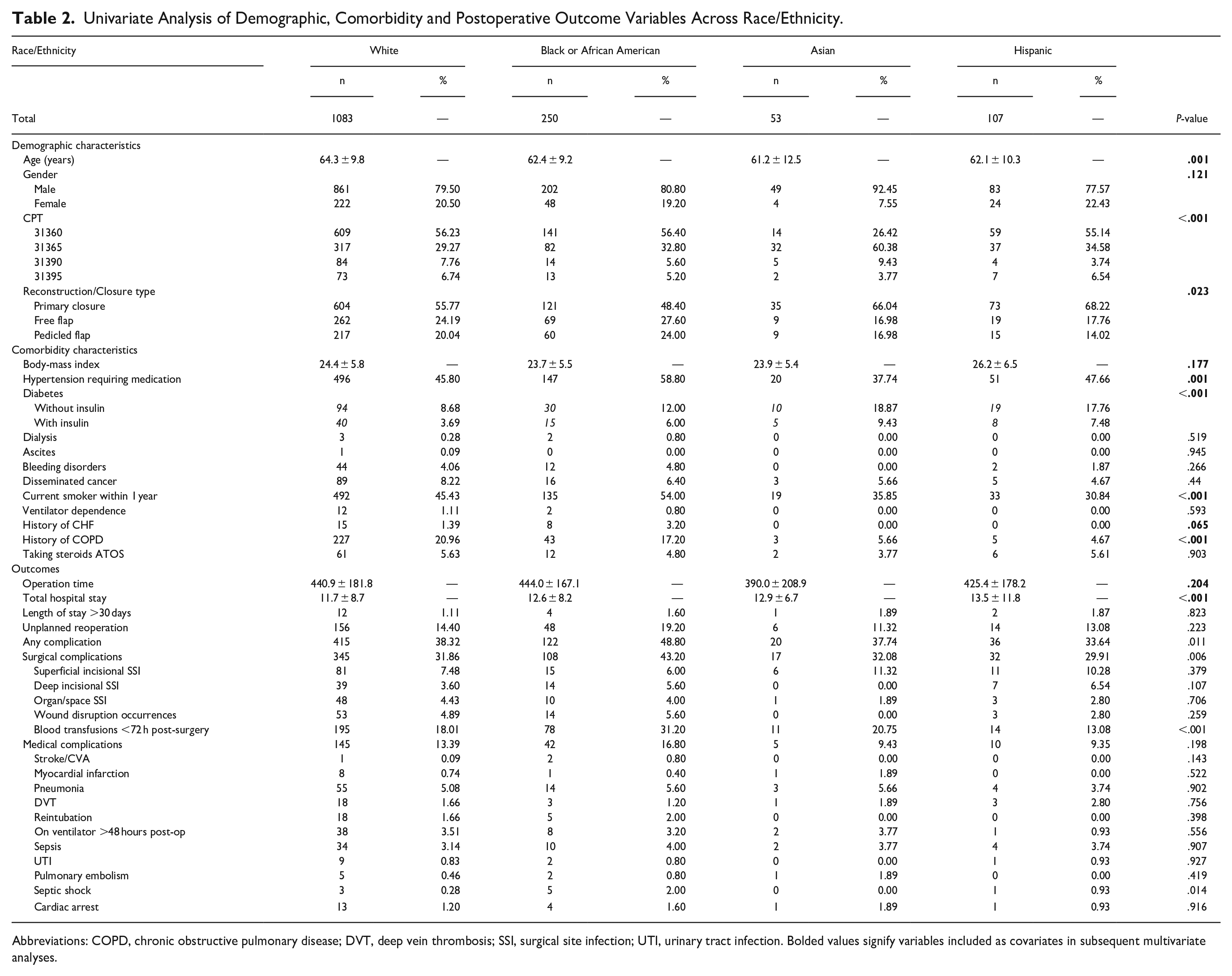
Abbreviations: COPD, chronic obstructive pulmonary disease; DVT, deep vein thrombosis; SSI, surgical site infection; UTI, urinary tract infection. Bolded values signify variables included as covariates in subsequent multivariate analyses.
Logistic Regression Analysis
Logistic regression analysis adjusted for the aforementioned demographic and clinical variables, along with other outcome variables that were not the primary variable of interest for that model. These analyses showed that, after controlling for confounders, Black patients had significantly-higher odds of any postoperative complications [odds ratio (OR) = 1.489, 95% confidence interval (CI): 1.108-2.001, P = .008] and surgical complications (OR = 1.532, 95% CI: 1.13-2.077, P = .006) than White patients. Black patients also had higher odds of perioperative blood transfusions (OR = 1.865, 95% CI: 1.326-2.624, P < .001). Hispanic and Asian patients did not show significant differences in complication rates compared with White patients. No significant findings were seen regarding reoperations or having a hospital stay >30 days (Table 3).
Logistic Regression Analysis of Key Binary Outcomes Across Race/Ethnicity.
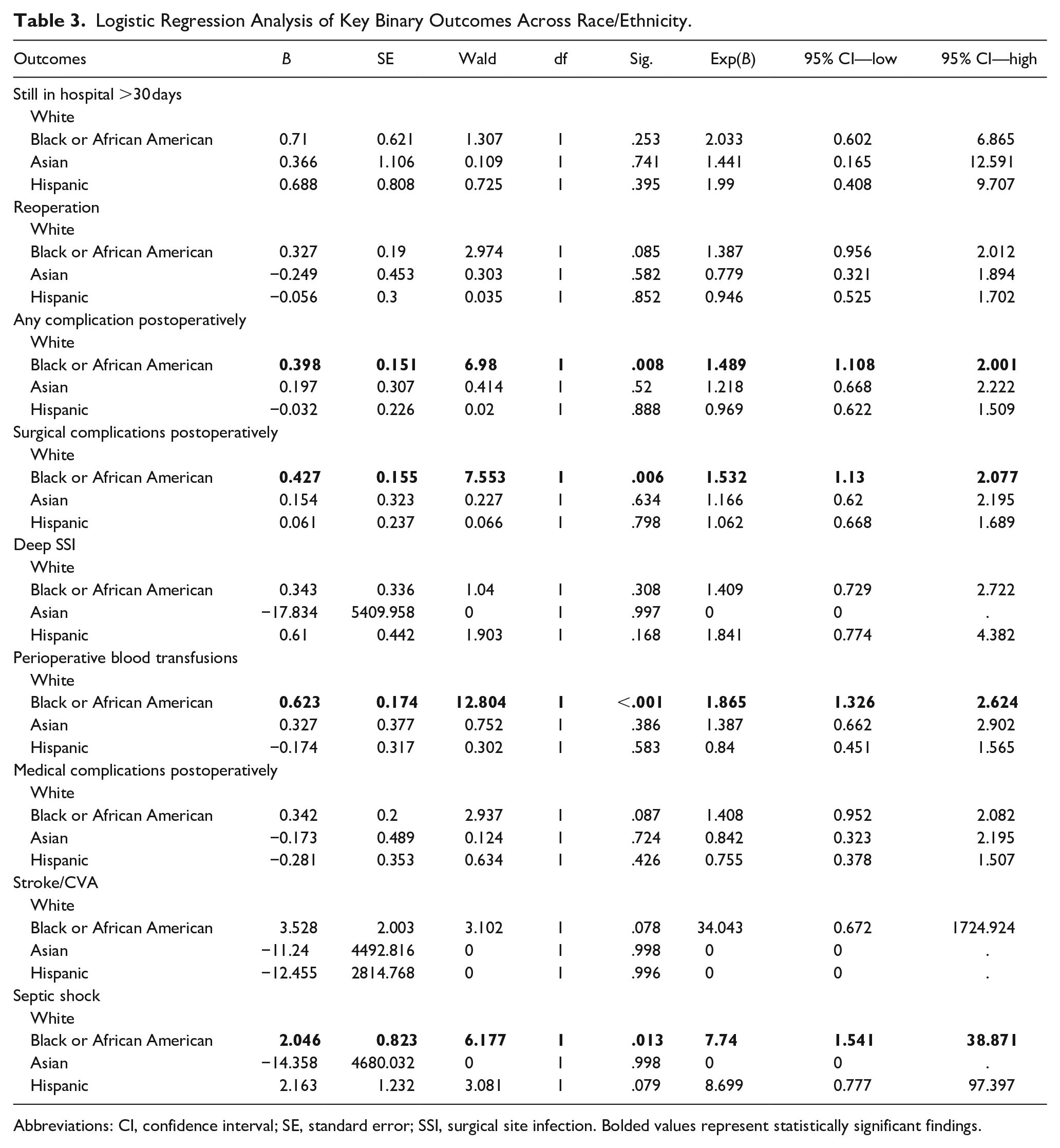
Abbreviations: CI, confidence interval; SE, standard error; SSI, surgical site infection. Bolded values represent statistically significant findings.
Linear Regression Analysis
Two continuous variables were analyzed in this study: operation time and total length of hospital stay. Similar to logistic regression, demographic and clinical variables with a P < .2 on univariate analysis, along with other outcome variables that were not the primary variable of interest for that model, were included in each model. Black patients had an operation time averaging 23.359 minutes longer than White patients after controlling for covariates, although this was marginally significant (P = .063). Asian patients had significantly-shorter operation times than White patients (P = .012). Hispanic patients had significantly-longer total hospital stays by approximately 2.39 days than White patients (P = .008) (Table 4).
Linear Regression Analysis of Continuous Postoperative Outcomes Across Race/Ethnicity.
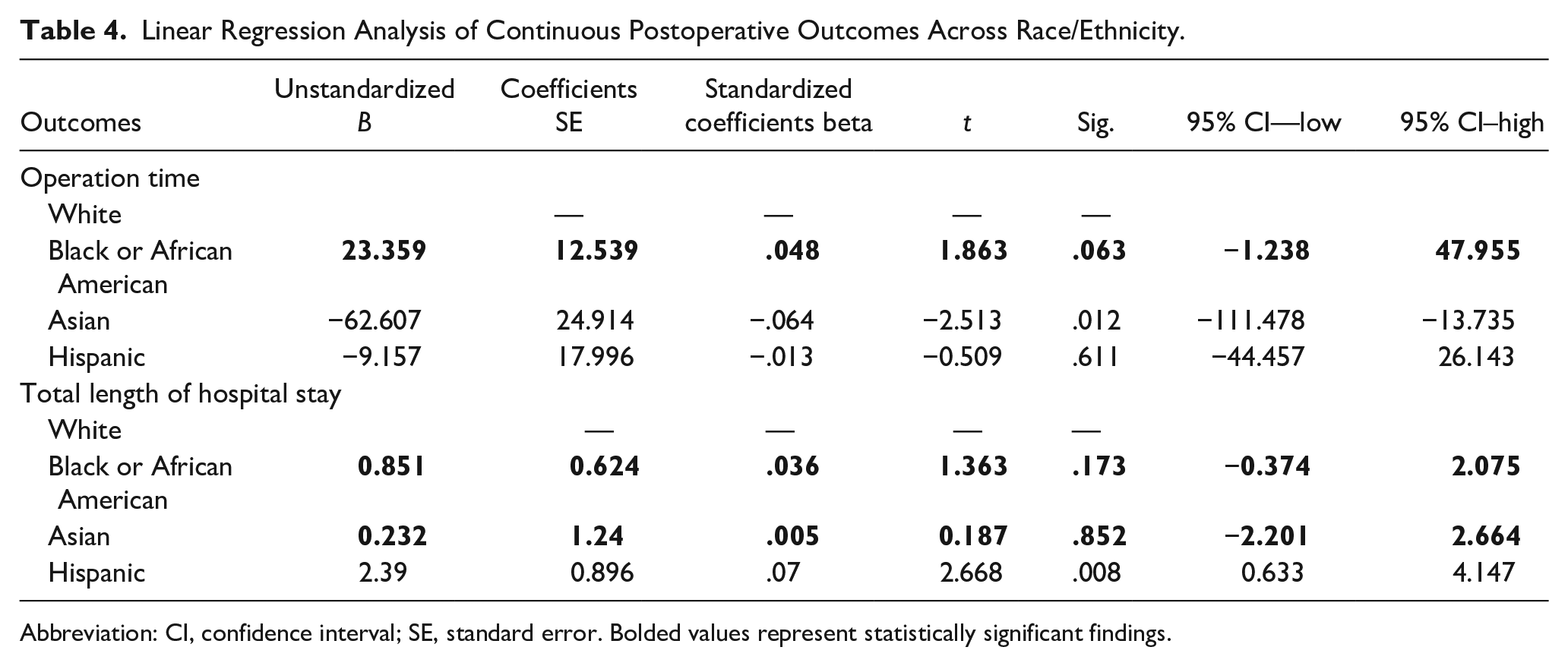
Abbreviation: CI, confidence interval; SE, standard error. Bolded values represent statistically significant findings.
Discussion
To our knowledge, this is the first study employing the NSQIP database for the analysis of race and ethnicity on perioperative outcomes following TL. Our analyses reveal significant differences among racial groups, notably that Black patients face higher odds of surgical complications within 30 days. These findings are consistent with previous literature demonstrating adverse outcomes in racial and ethnic minority patients following laryngeal cancer treatment.8,9,13 In this study, we attempted to ascertain existing differences in 30 day postoperative complication rates between race groups to determine whether disparate postoperative morbidity is an additional contributing component to racial inequity in laryngeal cancer care.
There are several factors that may contribute to the disparity in complication rates across race. First, there is an established difference in surgical decision making with Black patients being treated more often than White patients with TL for early-stage disease (T1/T2) even after controlling for stage at presentation and tumor grade.8,9 Differences in surgical management of laryngeal cancer extend to reconstruction, for which Black patients in our cohort received free flap or pedicled flaps more frequently than other racial and ethnic groups on univariate analysis (Figure 2). This may be explained partially by the established disparities in stage at presentation, which necessitate more extensive surgical resections requiring reconstructive techniques as opposed to primary closure. 13 Since Black patients have a greater likelihood of receiving triple modality therapy (surgery, chemotherapy, and radiation), it is also possible that flap utilization is more often needed due to the impact of radiation therapy (RT) on tissue integrity, limiting the ability to obtain primary closure following TL if performed as salvage surgery.14,15 Overall, there is limited assessment of racial or ethnic disparities across rates of primary versus salvage TL, and we found no studies evaluating disparities in reconstruction utilization following ablative head and neck surgery.
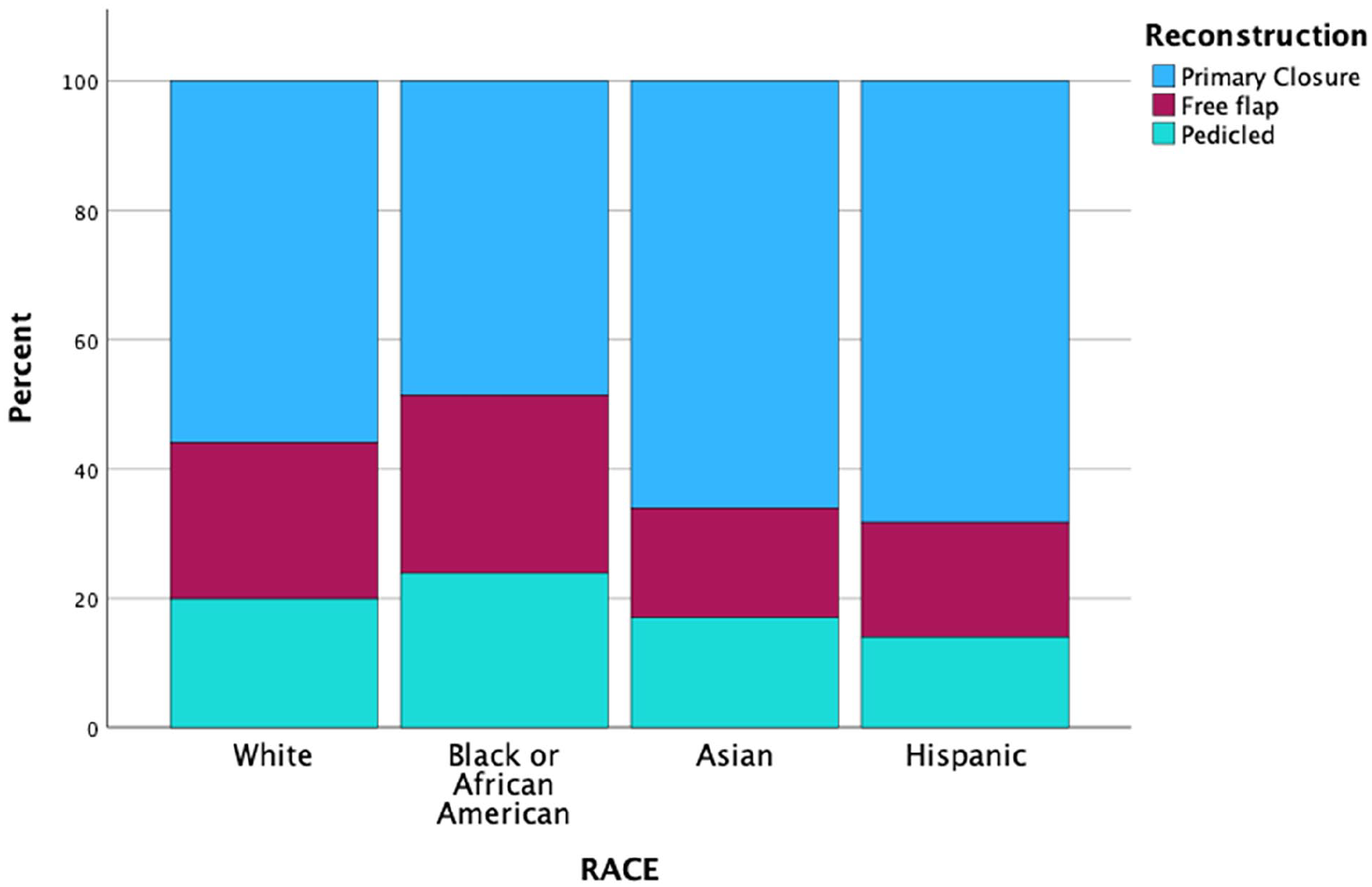
Distribution of reconstruction type by race.
Tobacco use also may play a role in increased surgical complications as Black patients in our cohort reported higher rates of smoking within 1 year prior to surgery (P < .001). The impact of continued tobacco use following diagnosis of head and neck cancer on postoperative prognosis is well-established in the literature.16,17 In Hatcher et al, current smokers are over 6 times more likely to experience complications following surgically-treated head and neck cancer. 18 Differences in preoperative tobacco cessation rates might act as a secondary driver of the racial disparity observed in this population. Nevertheless, after accounting for the contribution of reconstructive type/microvascular surgery, tobacco use, and other comorbid conditions, we have found that race is an independent predictor of adverse perioperative outcomes following TL.
In addition to clinical implications of disparate rates of head and neck reconstruction and surgical complications, there are also considerable financial impacts. Flap utilization following TL is a predictor of extended length of stay and subsequently increased inpatient hospitalization costs. 19 These increased costs are especially worrisome as nearly one third of cancer survivors report financial difficulty, which increases the likelihood of delaying or forgoing additional medical care. 20 Racial and ethnic minority groups experience these financial challenges more often than majority cohorts. 20 In this respect, we postulate that the choice of flap reconstruction and the clear disparities in perioperative outcomes might also translate to longer inpatient stays, greater financial strain, and potential loss to follow-up for Black patients following TL. Future prospective study of this pathway is required to understand the relationship between race and postoperative care in total laryngectomees.
Beyond financial implications and the individual burdens of 30-day postoperative complications, short term outcomes during the inpatient course following TL may extend to long-term prognosis. In a recent study by Boukovalas et al, the authors found that postoperative complications after TL are an independent risk factor for decreased overall survival and disease-free survival, compared with cases without complications. 21 Racial disparities in perioperative complications might play a role in the established trends in overall survival for laryngeal cancer patients, which disproportionately impact survivorship in Black patients. 9
Limitations
Although our study provides insight into disparities across racial and ethnic identity in patients undergoing TL, we acknowledge several limitations that are inherent to the ACS-NSQIP database. First, we lacked detailed information on extent of tumor and treatment plan such as stage at presentation, disease extent, and prior treatment, which may be modifying factors and cannot be measured using this database. While we evaluated “disseminated disease” in a univariate analysis and utilized CPT codes for head and neck reconstruction as a proxy for primary tumor size, the inability to control for oncologic variables limits the generalizability of these findings. Thus, primary, salvage, and functional TL cannot be differentiated. Second, we lacked information on patients’ socioeconomic and insurance status, which have been shown to correlate with race. For example, it is possible that Black patients treated within ACS-NSQIP hospitals have better socioeconomic status than other patients who receive care at lower quality hospitals.22,23 Despite these limitations, we conducted a rigorous assessment of racial disparities in postoperative outcomes following TL, using all relevant predictors identified on univariate analysis. While variables in NSQIP are limited from an oncologic standpoint, the value of a higher powered, national, multicenter cohort in detecting these preliminary disparities in perioperative outcomes is a valuable component of our understanding of racial disparities in total laryngectomees.
Future Directions
Despite limitations in controlling for oncologic factors, these results align with literature in other surgical specialties employing NSQIP for the analysis of perioperative disparities and reconstruction utilization across race/ethnicity.24 -27 Leveraging a national, multi-institutional cohort unveils pronounced racial inequity following TL, encouraging future prospective assessment of postoperative complications while accounting for all variables of interest including insurance status, hospital characteristics, primary tumor size, primary tumor location, stage, history of radiation therapy, and primary versus salvage TL. While the analysis of disparities in this setting is an invaluable part of the discussion on the treatment of laryngeal cancer, we encourage future study of disparities after TL that intentionally evaluate trends in health utilization, patient satisfaction, functional status, and quality of life. Given the known impact of sociodemographic predictors on speech rehabilitation after TL 28 and the influence of race/ethnicity on malnutrition, 29 mental health burden and substance use in patients with head and neck cancer, 30 it is reasonable to assess longitudinal health-related outcomes in racial and ethnic minorities following TL.
Beyond identifying where disparities exist, we suggest the application of these data to guide prospective interventions aimed toward improving outcomes following laryngeal cancer treatment, and post-TL. Cyberski et al draw attention to the fact that Black patients with laryngeal dysplasia or early-stage laryngeal squamous cell carcinoma (SCC) are less likely to be treated and more likely to be lost to follow-up. 31 To avoid subsequent use of morbid treatment and resulting perioperative disparities, adequate management of premalignant conditions and timely referral to an otolaryngologist is recommended strongly, especially in racial minority groups.
Given the notable disparities relating to surgical care in this cohort, we also recommend potential interventions for inpatient clinical pathways and patient care coordination. Hanna et al demonstrated the efficacy of a quality improvement pathway in reducing readmissions rates and length of stay resulting in a 14.5% cost reduction for hospitalization following TL. 32 A dedicated nurse navigator in otolaryngology aids the receipt of timely-treatment recommendations and has reduced socioeconomic disparities in patients with cleft lip/palate.33,34 The integration of clinical pathways and nurse navigators could be similarly valuable in total laryngectomees, to aid in monitoring and minimizing adverse outcomes following surgery, providing education for appropriate postoperative care, and coordinating follow-up visits for surveillance and allied health professions.
Conclusions
We evaluated the impact of race and ethnicity on postoperative complications in patients undergoing TL. We found increased odds of surgical complications and use of free flap or pedicled flap reconstruction in Black patients undergoing TL using the NSQIP database. Due to the absence of oncologic information such as stage and treatment history, and limited availability of information about additional socioeconomic drivers of health disparities, we encourage prospective work in this population. Further study is needed to determine conclusively whether race is an independent predictor of postoperative outcomes following TL and to establish effective methods of racial disparity reduction for laryngectomees.
Footnotes
Author Contributions
All authors contributed to the study conception and design. Tatiana Ferraro, Abdulla K. Ahmed, and Weston L. Niermeyer were responsible for material preparation, data collection, and analysis. All authors revised and approved the final manuscript. Dr Punam Thakkar, Dr Arjun S. Joshi, Dr Robert T. Sataloff supervised all research activities.
Data Availability
On request.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethics Considerations
Ethics approval is not required as the ACS-NSQIP database is a deidentified database; therefore, this study is exempt from George Washington University School of Medicine and Health Sciences Institutional Review Board.
Statement of Informed Consent
Informed consent for information published in this article was not obtained as the ACS-NSQIP database is a deidentified database.