
Abstract
Introduction
Foreign bodies in the pharynx are encountered in otolaryngology practice. Sometimes, these foreign bodies, if sharp, can pierce through the pharyngeal mucosa and become completely lodged in the soft tissues of the neck. 1 Patient manipulation, muscle contraction, and tissue reaction may contribute to the migration. 2,3 If not being treated properly, migrating foreign body may cause life-threatening complications such as penetration of vessels, deep neck infection, or retropharyngeal abscess. Removal of migrating foreign bodies through the transoral approach surgery under laryngoscope can be effective and minimally invasive. Herein, we summarize the clinical characteristics of migrating pharyngeal foreign bodies and share our experience and discuss key surgical techniques, aiming to improve the success rate of the removal of foreign bodies.
Clinical Study
We retrospectively evaluated 7 patients with migrating pharyngeal foreign bodies, who undergone the removal of foreign bodies by transoral approach surgery under laryngoscope at our institution. Once identified, the following data were collected: symptoms, time of onset, examination methods, buried sites of foreign bodies, methods of removal, and clinical outcomes.
Surgical Procedure
The patients should be positioned supine and undergo tracheal intubation under general anesthesia. A direct rigid laryngoscope is inserted to examine the pharynx for mucosal lacerations, points of purulent discharge, granulation tissues, or hidden foreign bodies, which are known as “signs.” If the foreign bodies are lodged in the oral pharynx, the Davis mouth gag can be used to expose the oral pharynx. Microscope or endoscope is particularly helpful in showing these signs. If it is unable to identify the “signs,” preoperative computed tomography (CT) scan can serve as a road map for localizing the foreign body. Anatomical landmarks, such as thyroid cartilage, cricoid cartilage, epiglottic cartilage, or hyoid bone, can be used as a guidance, followed by vertical or transverse incision of the pharyngeal wall, for further exploration of the foreign body. CO2 laser or radiofrequency coblation can be used to incise the pharyngeal wall along the signs. Blunt dissection is performed, and meticulous exploration using forceps allows for the identification and secure extraction of any encountered foreign bodies. If transoral removal of foreign bodies fails, the transcervical approach surgery will be attempted.
Data Analysis
Statistical analysis was performed using SPSS 19.0. Data were expressed as the mean ± standard deviation.
None of the work involved the use of animal or human participants. This was a retrospective medical chart review, and the patients were not identified.
Results
All the 7 patients presented chief complaints of foreign body sensation with progressive odynophagia or a painful enlarging mass in the neck. Among these patients, indirect laryngoscopy or flexible laryngoscopy did not reveal any foreign bodies. Six patients presented a clear history of foreign body ingestion. One patient gave the probable history of foreign body ingestion. CT scan or ultrasonography was performed for foreign body identification. Transoral approach surgery under laryngoscope was attempted in all cases, with the assistance of radiofrequency coblation or CO2 laser to make a mucosal incision.
Five foreign bodies were removed successfully by transoral approach. The transoral removal of foreign bodies failed in 2 cases, in which the foreign bodies were removed by transcervical approach subsequently. The total follow-up duration was at least 1 month. Significant complications were not observed. The mean age was 62.85 ± 11.32 years. The mean time from onset to confirmed diagnosis was 13.00 ± 10.00 days. The mean time of surgical time was 2.51 ± 0.90 hours. The mean length of hospital stay was 5.71 ± 2.56 days. Patient demographics are summarized in Table 1. Typical cases are illustrated in Figures 1 and 2.
Patient Demographics.
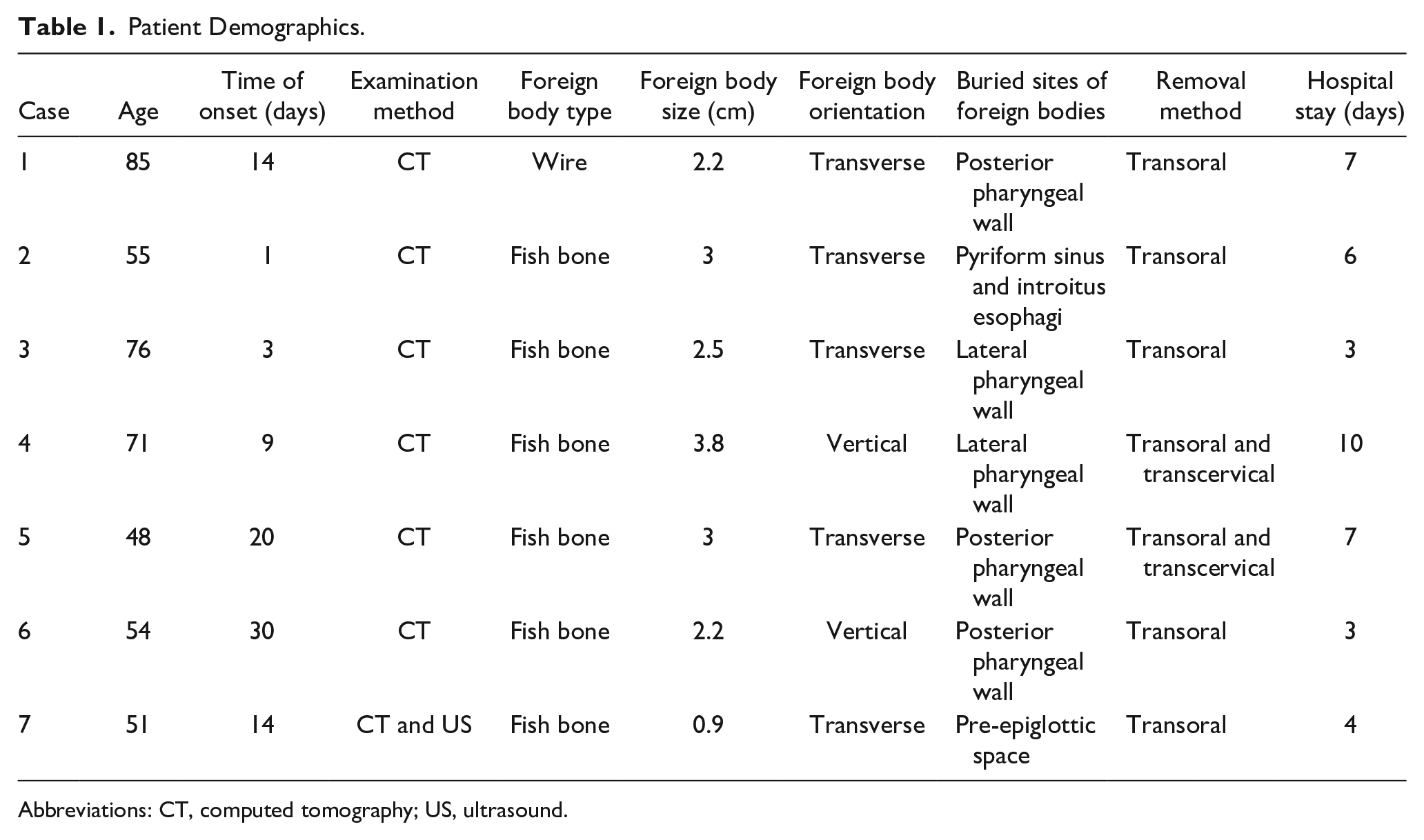
Abbreviations: CT, computed tomography; US, ultrasound.
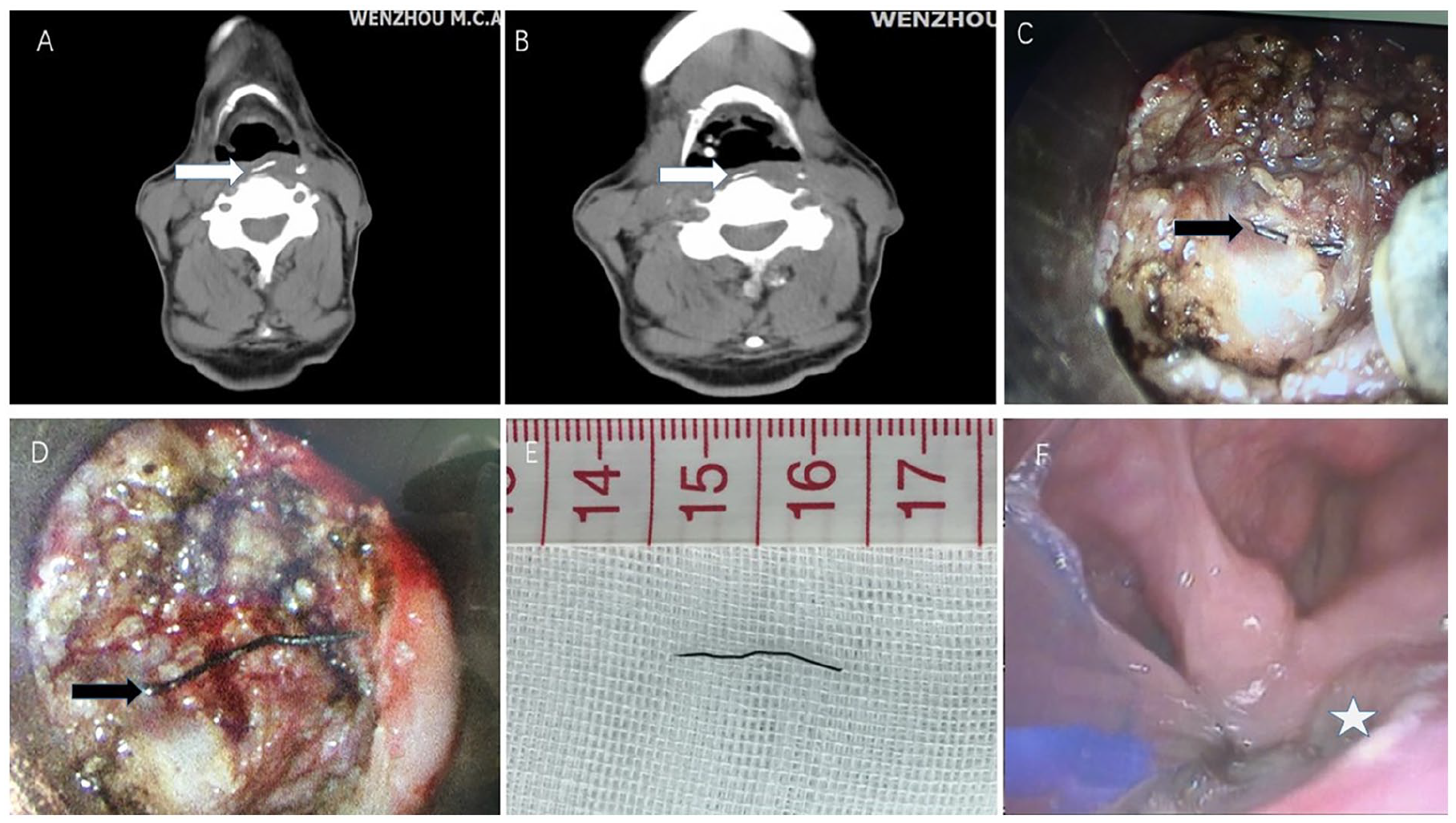
A 85-year-old man with migrating pharyngeal foreign body. (A, B) The transverse CT scans showed a linear radiopaque density (marked with an arrow), completely embedded in the bulging of the posterior pharyngeal wall. The foreign body was horizontally oriented. (C, D) Radiofrequency coblation was used to incise the pharyngeal wall along the bulge. The foreign body (marked with an arrow) was found after blunt dissection and adequate debridement of purulence and affected tissues. (E) A wire-like foreign body, 1.8 cm in length. (F) Laryngoscope examination 5 days after surgery showed the incision healed well (marked with a star). The blue object was nasogastric feeding tube. CT, computed tomography.
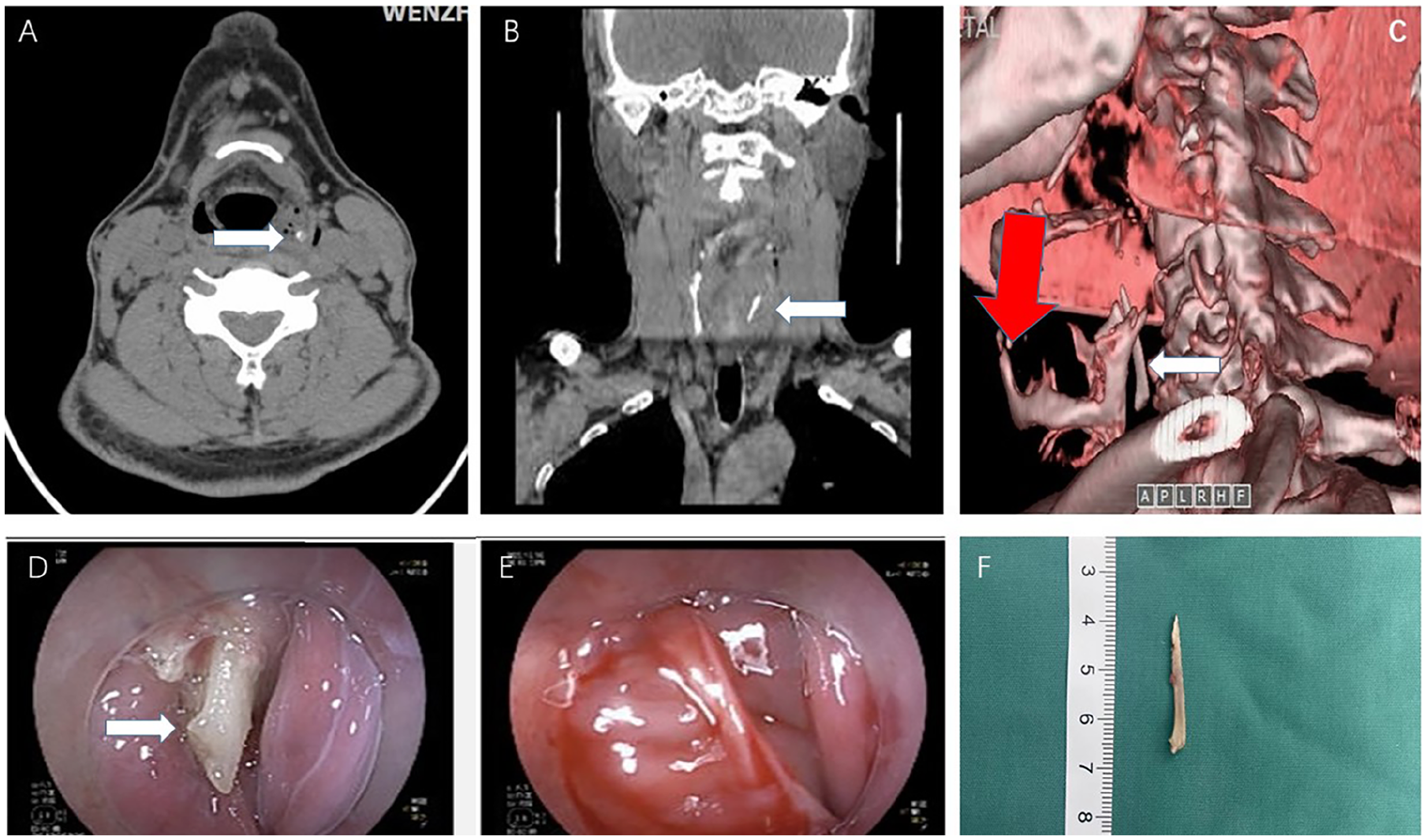
A 55-year-old man with migrating pharyngeal foreign body. (A, B) The transverse and coronal CT scans showed the foreign body (marked with an arrow) embedded in left pyriform fossae and upper esophagus. (C) The CT three-dimensional reconstruction showed the foreign body (marked with an arrow) was close to the inner side of thyroid cartilage (marked with a red arrow). (D) Gastroscopy revealed a fish bone (marked with an arrow) pierced the mucosa of introitus esophagi. (E) The removal of the foreign body failed. The foreign body disappeared during the repeated gastroscopy examination. (F) The foreign body (3.0 cm in length) was removed by transoral approach surgery via rigid laryngoscopy under general anesthesia. CT, computed tomography.
Case Report 1
A 85-year-old man presented to the otorhinolaryngology department with a chief complaint of sore throat and subsequent dysphagia for 14 days. He gave a history of foreign body ingestion prior to the onset of the symptoms. Examination showed bulging of the posterior pharyngeal wall. No foreign body could be visualized under flexible laryngoscopy. CT scan of the neck showed a linear radiopaque density, around 1.8 cm in length, completely embedded in the bulging of the posterior pharyngeal wall. Transoral approach surgery via rigid laryngoscopy under general anesthesia was performed. Radiofrequency coblation was used to incise the pharyngeal wall along the bulge. Blunt dissection was performed to access the retropharyngeal space and prevertebral space. A wire-like foreign body, 2.2 cm in length was found and removed following adequate debridement of purulence and affected tissues. Postoperative period was uneventful. The patient had resolution of his symptoms after the procedure and was fed by nosal gastric feeding for 5 days. He was discharged 7 days after the surgery.
Case Report 2
A 55-year-old man presented to the otorhinolaryngology department with a chief complaint of foreign body sensation for 1 days. He gave a history of fish bone ingestion prior to the onset of the symptom. Flexible laryngoscopy revealed bulging of the left pyriform fossae with pooling of saliva. But no foreign body could be visualized. CT scan of the neck showed a linear opacity at the left pyriform fossae and upper esophagus. Gastroscopy under local anesthesia revealed a fish bone pierced the mucosa of introitus esophagi. But the removal of the foreign body under gastroscopy failed, because the patient was unbearable to the procedure. No foreign body was found during the repeated gastroscopy examination. A repeated CT scan showed the foreign body still existed but pierced completely through the esophageal wall. Transoral approach surgery via rigid laryngoscopy under general anesthesia was performed. Radiofrequency coblation and CO2 laser were used to incise the posterior wall of the left pyriform fossae. A fish bone was found and removed following debridement of purulence. His symptom of foreign body sensation alleviated in immediate postoperative period, and the patient was fed by nosal gastric feeding for 9 days and was discharged asymptomatically.
Discussion
Pharyngeal foreign bodies are usually intralumenal. There has been rare documentation of foreign bodies penetrating the pharyngeal wall and migrating into the soft tissue of the neck. 4 A study by Remsen et al reviewed a series of 321 cases of penetrating foreign bodies, 43 cases were found extraluminally. 5 Sharp and linear foreign bodies such as a fish bone are more prone to perforate the wall of the pharynx and cause extraluminal migration subsequently. In our cases, all the foreign bodies are fish bones or wires. The migration of ingested foreign body is caused by the contraction of the hypopharyngeal and cricopharyngeal muscles during swallowing. Transversely-oriented foreign bodies are more likely to penetrate. This occurred in our cases too. Migrating foreign bodies could be lodged in the oral cavity, oropharynx, hypopharynx, or cervical esophagus. Patients may be asymptomatic initially, but present with foreign-body sensation, pharyngalgia, dysphagia, or swelling of the neck eventually. Migrating foreign bodies can introduce harmful bacteria to the soft tissue of the neck and cause parapharyngeal or retropharyngeal abscess. Infection can spread into the mediastinum through the anatomical cervical fascial planes and lead to mediastinitis. 6 A sharp foreign body might penetrate the major blood vessels and lead to life-threatening complications. 7
A thorough endoscopy, CT scan, or ultrasonography of the neck are the gold standard for diagnosis. 8 CT scan, especially three-dimensional reconstruction, can serve as a roadmap, which will reveal the size and orientation of foreign body, as well as its relationship with other vital structures. Contrast-enhanced CT is useful in cases with abscess. In our study, 1 patient got abscess in the pre-epiglottic space, but the CT scan did not reveal any foreign body, which was confirmed by preoperative ultrasound subsequently.
The position of the foreign body may change during surgery. Therefore, C-arm or handheld doppler ultrasound probe can be used to localize foreign body intraoperatively, if the foreign body is not found where it is seen in preoperative imaging. Janet W. Lee 9 reported the use of intraoperative, real-time ultrasound to guide endoscopic extraction of the foreign body, which allowed quick, safe treatment and prevented the need for a transcervical approach and its potential morbidities. The finding of edema, laceration, or granulation formation under endoscopy should arouse suspicion of migration, which can also serve as landmarks of hidden foreign bodies during surgical interventions. Hence, a careful preoperative endoscopy is extremely important. Laryngoscopic removal is possible if foreign body is partially migrated and embedded. 10,11
Potential methods for foreign bodies removal include transoral approach and transcervical approach surgery. The advantages of transoral approach surgery are the better cosmetic outcome and the lesser injury of great vessels and cranial nerves. The disadvantages of transoral approach surgery are poorer exposure and more difficulties of foreign body localization. Nien-Hsuan Ho 12 thought, for foreign bodies with complications, such as deep neck infection, hematoma formation, or that are close to great vessels and vital organs, an external approach surgery was more recommended. If there is concern for complications, such as vascular injury, the transoral approach surgery does not provide the opportunity to address and control these potential problems. As far as considering the proper method for migrated foreign bodies removal, it depends on how far from the lumen the foreign body has migrated into (less than 1.0 cm). But, if the foreign body is too deep into the mucosa or it is too close to major blood vessels, the transcervical incision will be recommended. Some researchers 12 recommended endoscopic approach surgery to remove foreign bodies, which were partially intraluminal and vertically oriented. However, in our study, all foreign bodies are complete extraluminal, of which, 5 were horizontally oriented and 2 were vertically oriented. But only 1 removal attempt failed in patient with horizontally-oriented foreign body. Foreign body removal under local anesthesia is always unbearable for most patients. During our surgery, we used a rigid laryngoscope to explore the pharynx, under general anesthesia. Limited dissection with a CO2 laser or radiofrequency coblation is safe and helpful in cases with edematous mucosa and granulation formation, which may obscure the foreign body. Transverse or vertical mucosal incision was initiated according to the orientation of foreign body. For horizontally- or diagonal oriented foreign bodies, we suggest making crossed mucosal incisions to increase the chances of encountering the foreign bodies. Therefore, massive mucosal damage was avoidable sometimes. Inflammation tissue and pus always indicate a foreign body in close proximity. Radiofrequency coblation has advantages of less or no hemorrhage. CO2 laser can provide more precise incision. Fish bone will always present as a black point under the microscope when it is burned by laser. Meticulous exploration using forceps allows for identification and secure extraction of any encountered foreign body.
The CT scan should be repeated, especially when one procedure fails or the clinical presentation changes. 13 In case 2, gastroscopy under local anesthesia revealed the fish bone, but the removal failed. A repeated CT scan showed changed position of foreign body. In our study, transoral remove of foreign bodies failed in 2 cases, in which the laryngoscopic exploration had lasted for at least 1 hour. Then, transcervical approach was attempted in the same period surgical operation. Therefore, repeated CT scan was not applied during the surgery. The foreign bodies were removed successfully in the end, and the 2 patients recovered uneventfully.
In our series, the CO2 laser or radiofrequency coblation was used to incise the pharyngeal wall, which have huge advantages in providing a more precise incision and a clear surgical field. To the best of our knowledge, there are few literatures reporting the use of CO2 laser or radiofrequency coblation for the management of migrating ingested foreign body in the pharynx, through transoral approach under laryngoscope.
The accurate intraoperative localization of the foreign body is always the difficulty and key point of the surgery, which is also the limitation of our study. We utilized edema, laceration, and granulation formation as the landmarks of hidden foreign bodies. But in some cases, they were inconspicuous. Baba et al 14 used intraoperative real-time ultrasound to measure the distance from the forceps to the foreign body, which can also guide the mucosal incision. In another literature, the foreign body was retrieved under ultrasound guidance, without mucosal incision or endoscopic visualization of the foreign bodies. But the ultrasound also has limitation in localizing an entirely-extraluminal foreign body, thereby increasing the risks associated with neck exploration. 9 In our further study, we would like to improve the accuracy in localizing the foreign body.
Herein, we have summarized some key points on surgical approach choosing and surgical procedure, although our series is too small to show major technical innovations. (1) The transoral approach surgery is recommended in patients with completely-migrated foreign body, which proximal distance is less than 1.0 cm from the lumen. If the foreign body is too deep into the mucosa or it is too close to major blood vessels, the transcervical incision will be recommended. (2) CT 3-dimensional reconstruction can distinctly display the shape and location of foreign body and show its relationship with anatomical landmarks, such as hyoid bone, thyroid cartilage, or cricoid cartilage, which will play an important role in making mucosal incision. To the best of our knowledge, there are few reports of CT three-dimensional reconstruction in extraluminal parapharyngeal foreign body removal with transoral approach. The use of C-arm or handheld Doppler ultrasound probe is also recommended if the foreign body is invisible during surgery. (3) As for foreign bodies, which are horizontally- or diagonal oriented, we suggest making crossed mucosal incisions to increase the chances of encountering the foreign bodies. Pay attention to edema, laceration and granulation formation during entire procedure. (4) The main reasons for the failure of transoral removal of foreign bodies are inaccurate localizing and improper initial mucosal incisions.
Conclusions
Transoral approach surgery for the removal of migrating pharyngeal foreign bodies under rigid laryngoscope is possible, which can be effective and minimally invasive with the assistance of radiofrequency coblation or CO2 laser. Careful radiological evaluation and endoscopic evaluation before surgery are essential. Certain endoscopic findings and anatomical landmarks are useful in localizing the foreign bodies. If the foreign bodies cannot be revealed after meticulous endoscopic exploration, transcervical incision is strongly recommended.
Footnotes
Acknowledgements
The authors thank all members of the Department of Otolaryngology, The First Affiliated Hospital of Wenzhou Medical College, for their invaluable help.
Data Availability Statement
The data that support the findings of this study are available from the corresponding author upon reasonable request
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was jointly supported by the National Natural Science Foundation of China under Grant No. 82171144.
Ethical Statement
This study did not involve animals or human participants. No patients were identified.