
Abstract
Ingested foreign bodies occasionally migrate to the paraglottic space. The external transcervical approach is almost always required to extract completely embedded foreign bodies. We report a case of an ingested fishbone embedded in the paraglottic space, which was successfully removed through transcervical exploration of the paraglottic space via the posterolateral approach. The posterolateral approach is safe and effective for the removal of foreign bodies completely embedded in the paraglottic space.
Introduction
Airway foreign bodies are one of the most common otorhinolaryngological emergencies. Laryngeal foreign bodies are rare and account for less than 4% of all foreign bodies; foreign body migration into the paraglottic space is even rarer. A review of the English medical literature revealed only 4 cases of foreign body migration to the paraglottic space.1-4 We report a case of migration to the paraglottic space of an ingested foreign body, which was successfully removed through transcervical exploration of the paraglottic space via the posterolateral approach.
Case Presentation
A 51-year-old female presented to our otolaryngology department with persistent pharyngalgia 11 days after accidental ingestion of a fishbone. She did not have hoarseness, dyspnea, or dysphagia. She was treated with intravenous fluids for 1 week at a local hospital, but her symptoms did not improve. Subsequently, she developed face and neck redness and swelling, for which she was referred to our hospital. The patient had hypertension for more than 20 years that was well-controlled with medications.
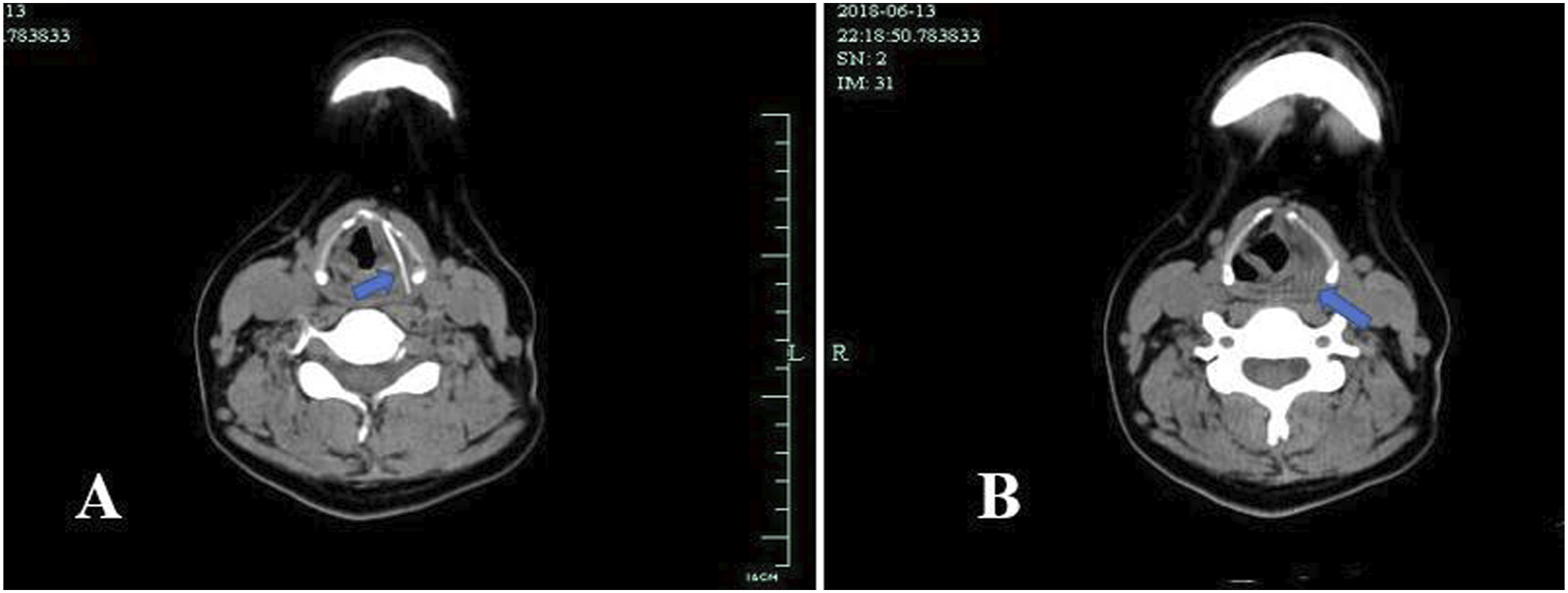
Cervical palpation revealed mild neck swelling. Laryngostroboscopy showed a markedly swollen left-sided false vocal cord, aryepiglottic fold, and pyriform fossa, and normal vocal cord mobility (Figure 1). However, the foreign body was not visualized in the pharynx or larynx. Computed tomography (CT) of the neck revealed a 3.6 cm linear foreign body that was completely embedded in the left paraglottic space and marked edema of the surrounding soft tissue (Figure 2). Direct laryngoscopic examination using an endoscope failed to visualize the foreign body. Laryngostroboscopy showed markedly swelling of false vocal cord, aryepiglottic fold, and pyriform fossa on the left side, and the vocal cord mobility was normal. Computed tomography scan of the neck revealed a linear object of high density completely embedded in the left paraglottic space (A), with surrounding soft tissue marked edema (B).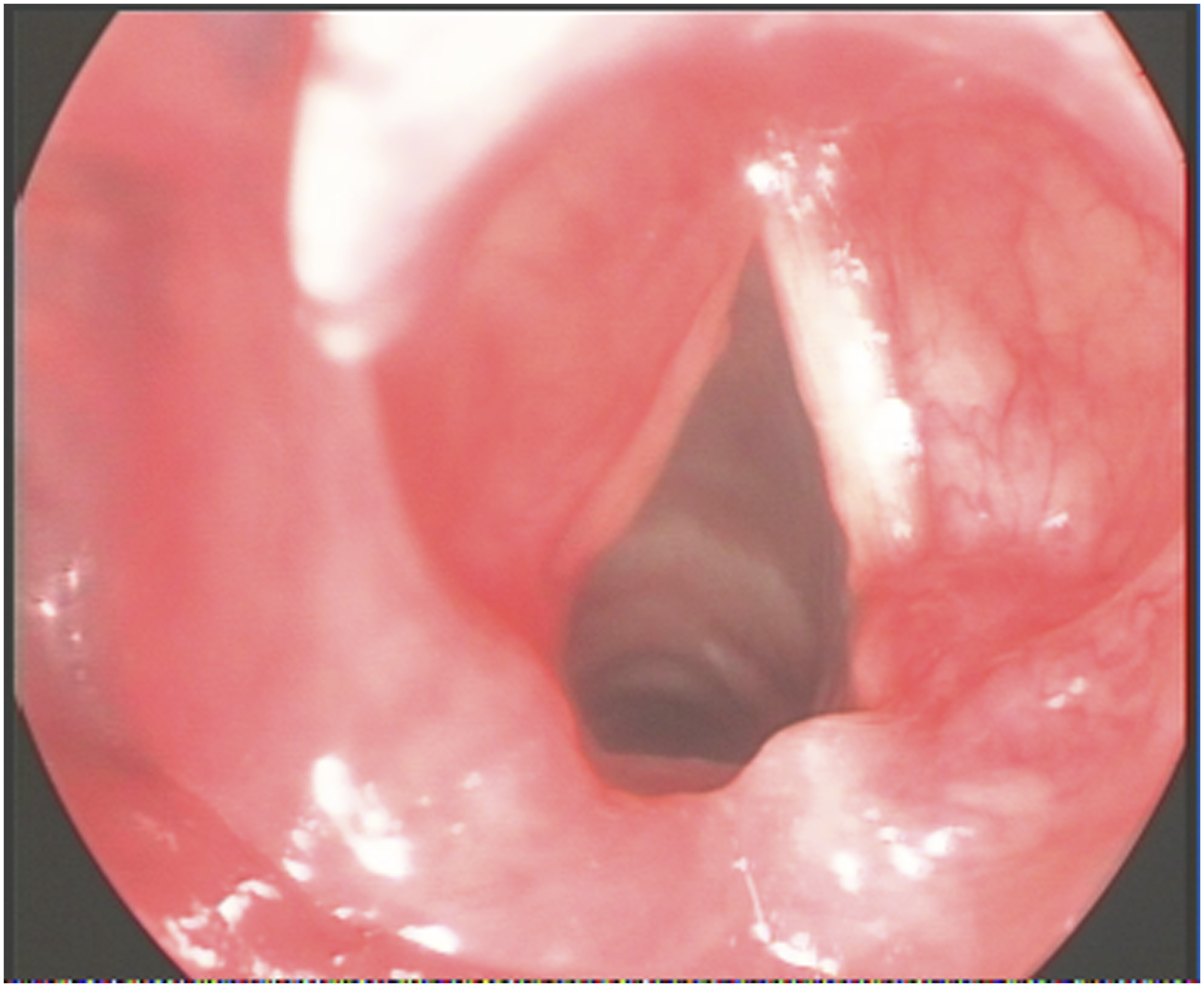
Transcervical exploration was performed using the posterolateral approach. A platysma myocutaneous flap was raised to expose the strap muscles, and the lateral margin of the left strap muscles was dissected to expose the hypopharyngeal constrictor. The hypopharyngeal constrictor was detached to expose the posterolateral margin of the thyroid cartilage. The thyroid cartilage was approached from the medial side to access the left paraglottic space, which revealed the foreign body. Thereafter, the foreign body was successfully retrieved (Figure 3). The fishbone was successfully extracted.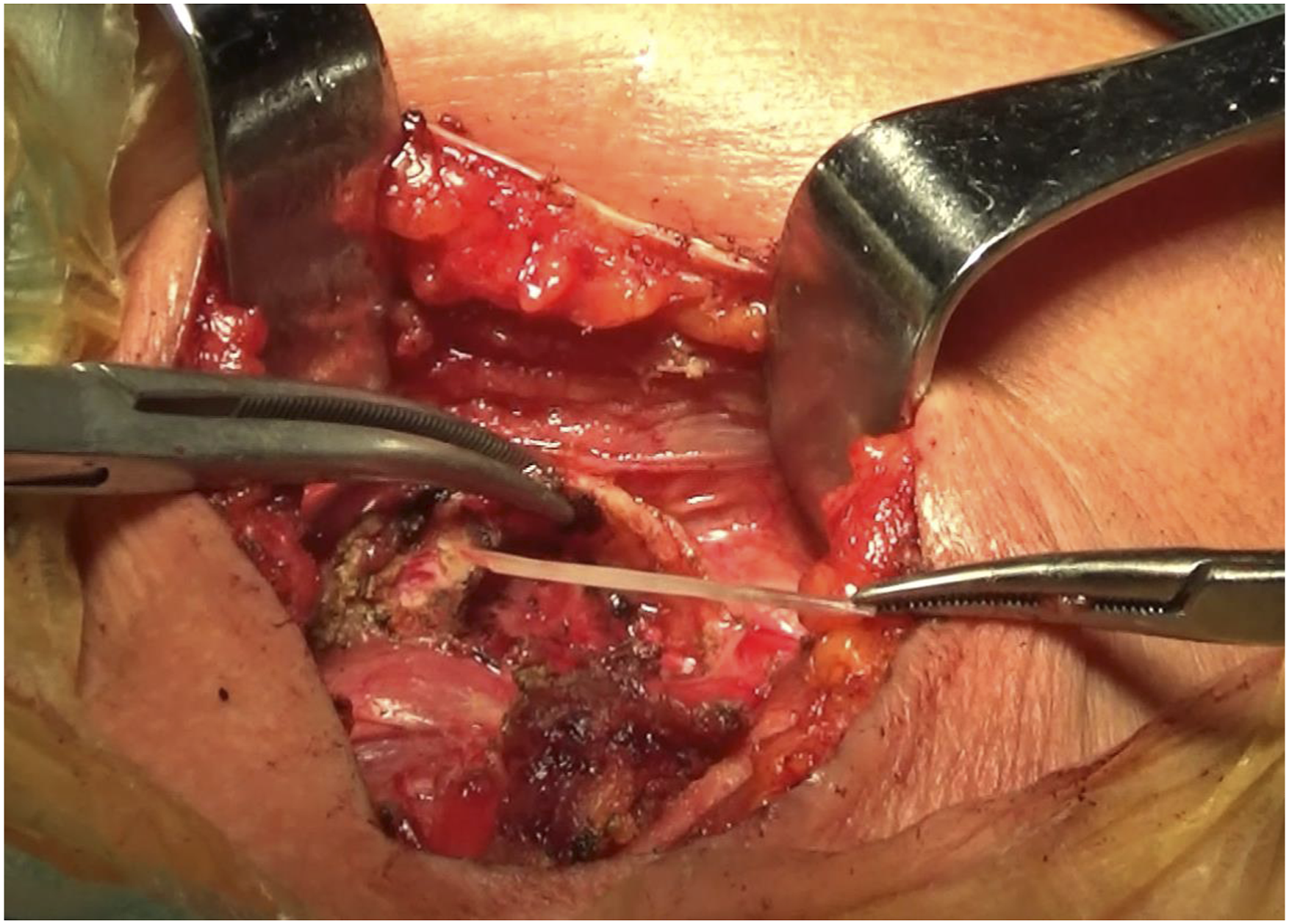
The patient had an uneventful postoperative recovery and was discharged on the seventh postoperative day. She did not have any residual swallowing difficulty and her voice returned to normal. Computed tomography of the neck was repeated after 1 month and was normal (Figure 4). Computed tomography scan of the neck was reexamined and no abnormality was found.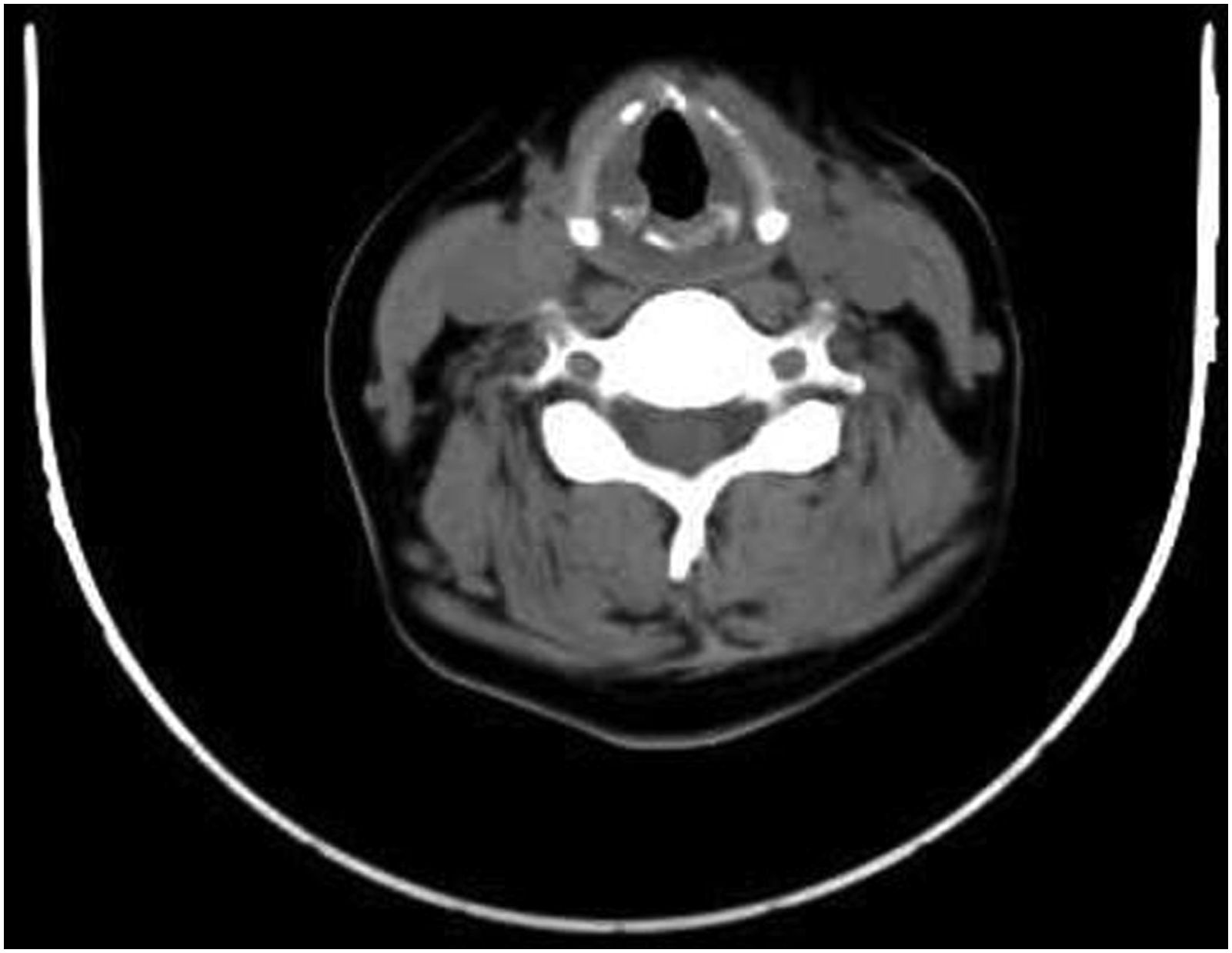
Discussion
We searched the MEDLINE database for English medical literature using the search terms “intralaryngeal” OR “endolaryngeal” OR “larynx” OR “paraglottic space” AND “foreign body”.
Migration of an Ingested Foreign Body into the Paraglottic Space Reported in English Medical Literature.
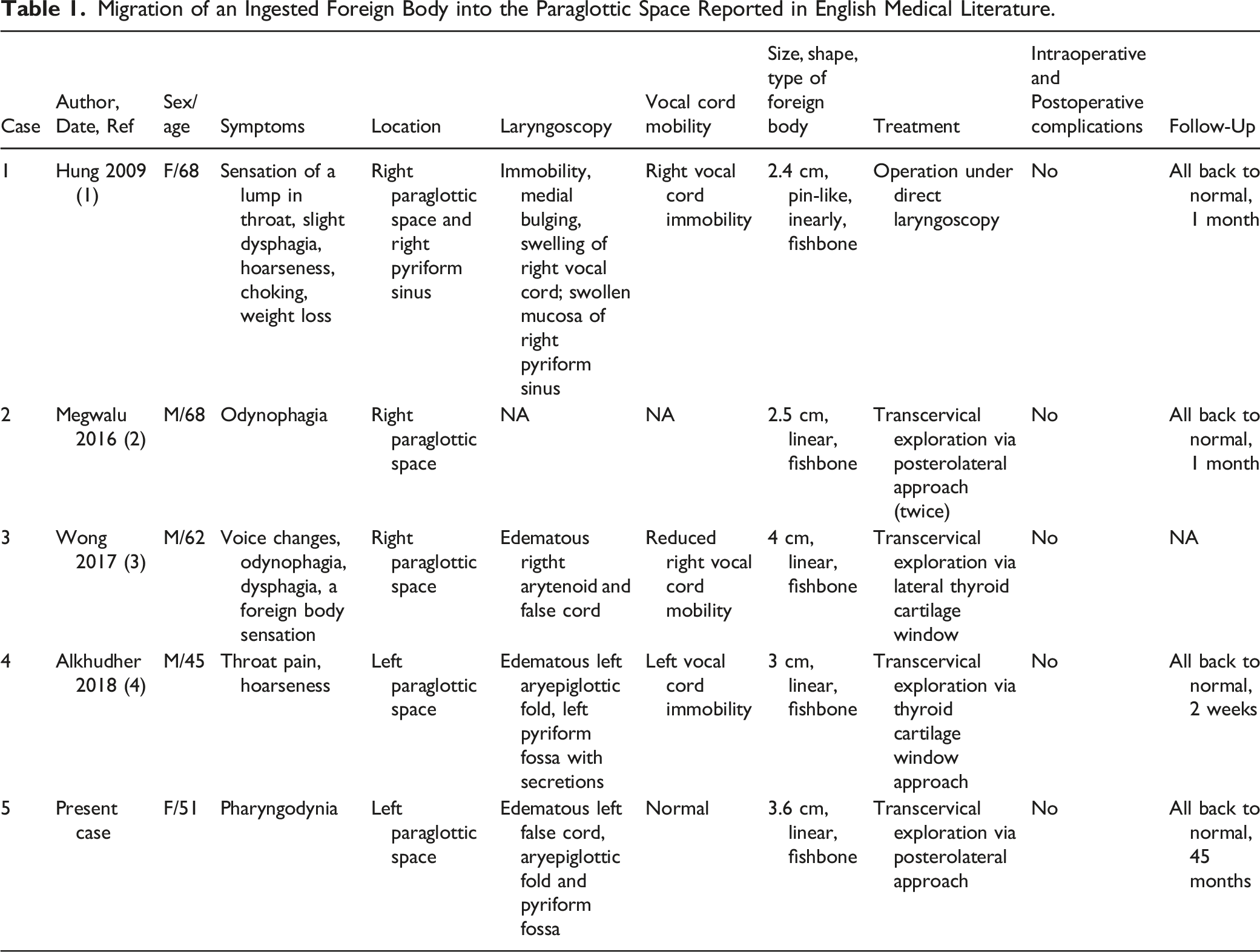
Most laryngeal foreign bodies can be removed using endoscopic techniques. Hung et al 1 used the endoscopic approach to remove an ingested fishbone embedded in the paraglottic space; in that patient, the fishbone was impacted in the lateral wall of the pyriform sinus and could be seen via direct laryngoscopy. However, completely embedded foreign bodies may not be visualized by endoscopy and should be removed using the transcervical approach. Transcervical exploration techniques for the paraglottic space include thyrotomy of the lateral thyroid cartilage, thyroid cartilage window, and anterior laryngofissure, and posterolateral approaches.2-5 Unlike the other approaches, the posterolateral approach does not damage the laryngeal frame or mucosa of the larynx and pharynx, so there is less trauma and fewer complications. In 2016, Megwalu et al 2 first reported the posterolateral approach for removal of a foreign body from the paraglottic space; however, the first removal attempt failed and the patient required reoperation. In comparison, we successfully removed the foreign body during a single operation using the aforementioned technique, which allowed precise preoperative and intraoperative localization of the fishbone.
Conclusions
Foreign bodies are rarely embedded in the paraglottic space. In completely embedded foreign bodies, an external transcervical approach is almost always required. The posterolateral approach is a safe and effective option for foreign bodies that are completely embedded in the paraglottic space.
Footnotes
Acknowledgments
We would like to thank for the support by Scientific Research Fund of Zhejiang Provincial Education Department (NO. Y202045601).
Author Contributions
BYY and GM designed and wrote the article. CZ reviewed the references and made the Figures. CHC collection of clinical data and made the table. CZZ and GY analysis of the data. ZSH revision of the article.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by Scientific Research Fund of Zhejiang Provincial Education Department (NO. Y202045601).
Informed Consent
Written informed consent was obtained from the patient for the publication of any potentially identifiable images or data included in this article.