
Abstract
Introduction:
The basis of dorsal preservation rhinoplasty goes back to the late 19th and the early 20th centuries. In that era, pioneers such as Drs. Goodale, Lothrop, and Cottle were prominent surgeons who reported on this technique. Currently, there has been a renewed interest of this technique that stems from the nasal anatomy and an interest in less destructive techniques. In this review, we discuss examples of the contributions of those surgeons, which represent some of the earliest experiences in this field.
Methods:
We reviewed several journals from the late 19th and early 20th centuries as detailed in the references section. We collected the related publications on closed reduction techniques performed by Drs. Goodale, Lothrop, and Cottle.
Results:
The publications on closed reduction techniques by Drs. Goodale, Lothrop, and Cottle described similar thought processes and techniques comparable to current dorsal preservation rhinoplasty techniques. The thought processes of these 3 renowned rhinoplasty surgeons appear to be very much relevant today.
Conclusions:
Although there has been recent resurgence in dorsal preservation rhinoplasty techniques due to anatomical and functional aspects of the nose, the basis of dorsal preservation rhinoplasty goes far back to more than 100 years ago.
Introduction
Rhinoplasty has evolved over generational epochs often associated with landmark publications and the simultaneous popularity of revolutionary surgical techniques. 1 As the early closed approach for rhinoplasty reached its pinnacle of influence, the open approach gained popularity. 1 The basis of the closed technique (now known as the dorsal preservation rhinoplasty) originated in the late 19th and the early 20th centuries. Pioneers such as Joseph Goodale, Oliver Lothrop, and Maurice Cottle were prominent surgeons in that era who reported on this technique.2-4 As time passed, the authors have noted that the work of Goodale and Lothrop may have been overlooked and forgotten over time. This manuscript outlines their important contributions to rhinoplasty in this current “reinvigoration” of preservation rhinoplasty. In this current day and age, there may be an important Renaissance period of preservation rhinoplasty techniques that may be relevant.
Despite aesthetic and functional results with an open rhinoplasty technique, minor revisions and major secondary rhinoplasties persist. 1 However, recently, major advances have occurred in our understanding of nasal anatomy, and how it relates to nasal aesthetics and surgical techniques. Two of the most interesting are the composition of the soft tissue envelope, including the nasal ligaments and the osseocartilaginous vault. 1 Notably, changes in the soft tissue envelope may significantly affect the result of rhinoplasty over decades.
The nasal ligaments have long been overlooked yet they are critical for both functional and aesthetic reasons.1,5 Anatomical dissections have shown convincingly that the bony hump is in reality a thin “bony cap” which can be easily rasped away while preserving the underlying cartilaginous vault.1,6 In addition, the keystone area is in reality a semimobile chondrosseous “joint” which can be converted from convex to straight by resecting its underlying cartilaginous septal support.1,7 This development in the understanding of nasal anatomy may have led to reemergence of closed reduction techniques when the rhinoplasty surgeon performs nasal reduction while preserving the dorsum of the nose. In this study, we review those 3 aforementioned surgeons, discuss examples of the related work they have done in this field, and draw parallels to their relevance to this current day in rhinoplasty techniques.
Joseph Lincoln Goodale, MD, was an active member of the American Laryngologic Association from 1889 to 1936 and honored as an emeritus fellow since. 2 Joseph Lincoln Goodale was born on January 22, 1868 at Saco, Maine. He was interested in throat diseases, bacteriology, immunology, and respiratory disease among other areas. He was the son of Professor George Lincoln Goodale (1839-1923) who was an important member in his state and was interested in fruit growing, arboriculture in general in addition to being a physician. 8
Dr Goodale studied at Portland Medical School (1889-1890). He then joined the second class at Harvard Medical School in 1891 and graduated in 1893. In 1893-1894, he studied medicine at Wurzburg, Berlin, Heidelberg, and London. 9 For the next 2 years he was with the Massachusetts Board of Health and because of his studies in bacteriology became interested in the first production on a mass scale of diphtheria antitoxin. 2 He also became an assistant physician for diseases of the throat in Massachusetts General Hospital in 1895 and 1896 and held a similar position in Boston Children’s Hospital. He became instructor in Laryngology in Harvard Medical School in 1908. He practiced medicine in Boston as a specialist in throat diseases. 9 He was elected to the American Laryngological Association in 1898 and was its president in 1916. Dr Goodale was a fellow of the American Academy of Sciences. 2
One of Goodale’s areas of interest was the correction of nasal deformities that resulted from congenital abnormalities or trauma and other acquired diseases. He was among the first surgeons who published on the endonasal correction of nasal deformities that set the stage for the development of the current dorsal preservation techniques.
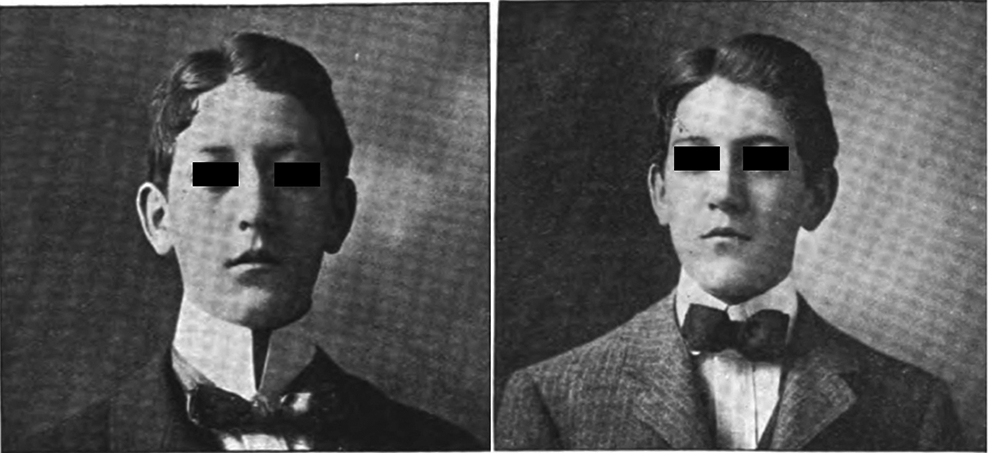
In 1899, he published a paper entitled “A new method for operative correction of exaggerated Roman nose.” In this study, he described endonasal correction of the nasal deformity, thereby avoiding violating the skin covering the vault of the nose. In that procedure, he removed a portion of the septum along its superior margin. Next, he described depression of the bony bridge of the nose. This maneuver was achieved using a small saw introduced through the left nostril. The articulation of the nasal and maxillary bones were approached through from below upward. This procedure was repeated on the right side. A few “gentle taps” upon the nasal bones were applied to break the frontal articulation and depress them until they came into contact with the upper margin of the septum. With the depression of the nasal bones, a ridge appeared on either side, formed by the maxillary bone along the line of the nasal articulation. This was corrected by “2 or 3 light blows, with a protected mallet,” fracturing the maxillary bone, he noted as being very thin. The procedure took about 40 minutes. Goodale described the results as satisfactory (Figure 1). 10
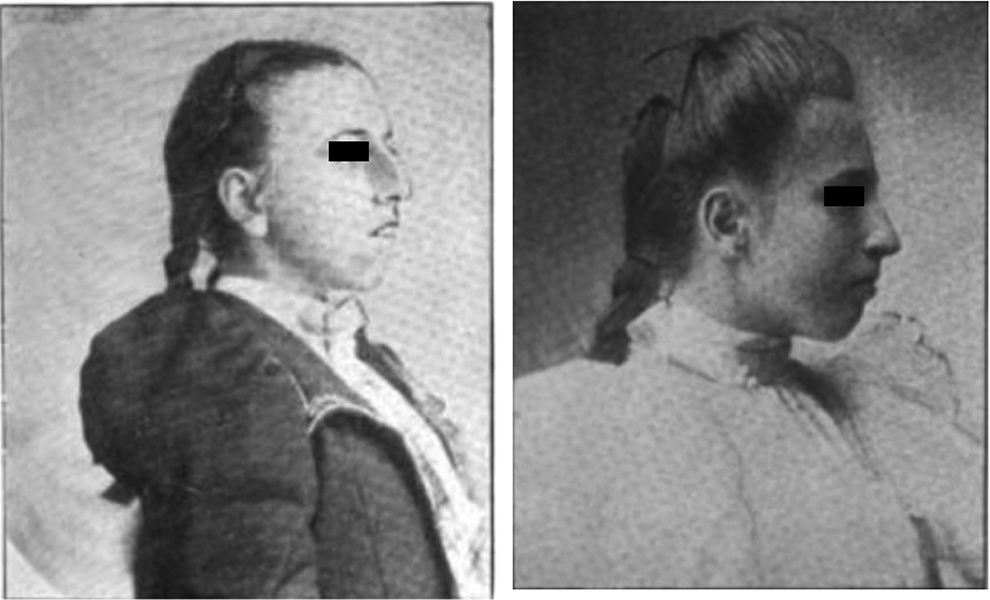
(Left) Preoperative. (Right) Postoperative. Reproduced with minor modifications from Goodale. 10
In 1900, Dr Goodale published “On the correction of old traumatic depressions of the nose by subcutaneous plastic operation.” He reported 2 cases in this study. The first was a 25-year-old male who had a depression of the nasal bridge at the middle of the superior outline of the triangular cartilage. That depression resulted from a septal abscess that was preceded by a fall on the nose a year prior. He corrected the deformity by resecting a quadrangular piece of septal cartilage and lifting it upward subcutaneously until the external depression was filled out. The transported flap was held in place by gold plated pins thrust through it and the adjacent septum on each side in an anteroposterior direction (Figure 2). 11
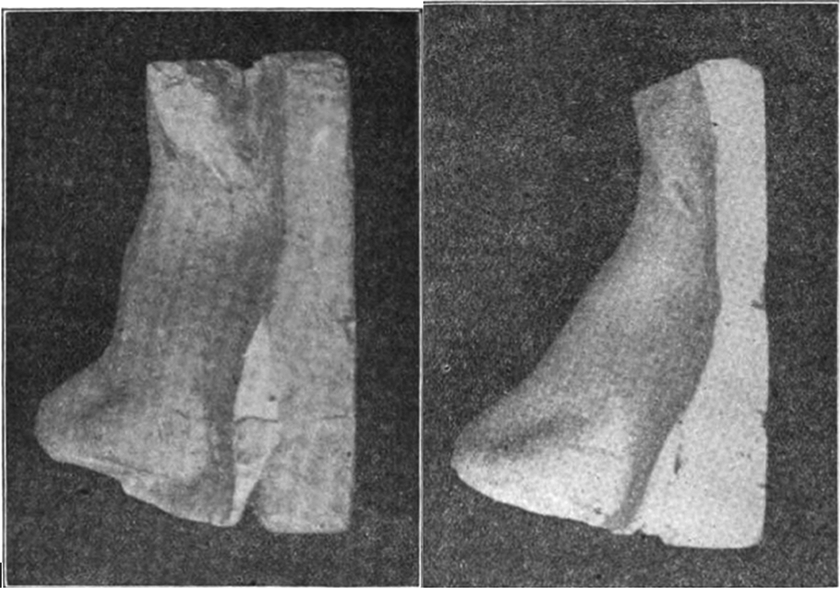
(Left) Photograph from plaster cast of nose taken before the operation. (Right) Photograph from plaster cast of nose taken 6 weeks after the operation. Reproduced from Goodale. 11
The second case was a 17-year-old male who sustained a nasal trauma resulting in a symmetrical depression of the nasal bones from fracture along their lines of union with the frontal and maxillary bones. On internal examination, Goodale described the triangular cartilage as physiologically “normal” but that there was a long spur on the right side at its junction with the vomer. During the operation, the spur was reduced from below upward leaving the mucous membrane of its superior surface intact. A “slender” knife was then used through the right nasal passage and a broad sweeping incision made between the upper surface of the nasal bones and the overlying skin, thus forming a subcutaneous chamber between these 2 structures. The spur was then rolled upward, still adherent by its mucous membrane to the septum, and after some loosening of the membrane to afford the “necessary slack,” was carried into the “chamber prepared for it.” The skin of the bridge was thus lifted from the nasal bones by the spur. The spur was held in position by a suture through its mucous membrane from one side of the nose to the other. An external splint was applied. The patient had satisfactory results 8 months after the procedure (Figure 3). 11
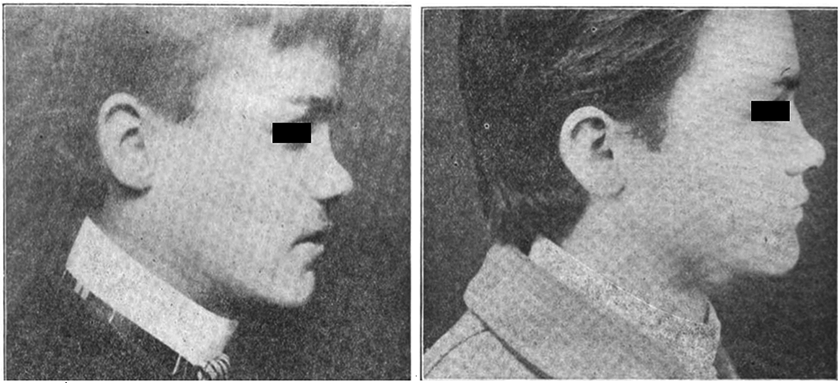
(Left) Preoperative. (Right) Postoperative. Reproduced with minor modifications from Goodale. 11
In 1901, Goodale published “The correction of old lateral displacement of the nasal bones.” In this study, he reported a series of 22 cases. The technique was based on the procedure described earlier when he corrected a Roman nose. First, he divided the septum into a “narrow upper strip” connected with the bridge of the nose and a large inferior portion attached to the floor of the nose using endonasal technique. The next step was to free the nasal bones from their lateral attachments to the frontonasal processes of the maxillary bone. A small saw was used through the nasal passage and the articulation of the nasal and maxillary bones sawn through from below upward. The procedure was done on both sides and the nasal bones were freed from their articulations, with the exception of their attachment to the frontal bone. One or 2 careful taps with a mallet on the convex side of the displacement usually suffice to loosen the frontonasal articulation, rendering it possible to carry the nasal bones into the median line. An external splint was always used (Figure 4). 12 He was satisfied with the results (Figure 5). 12
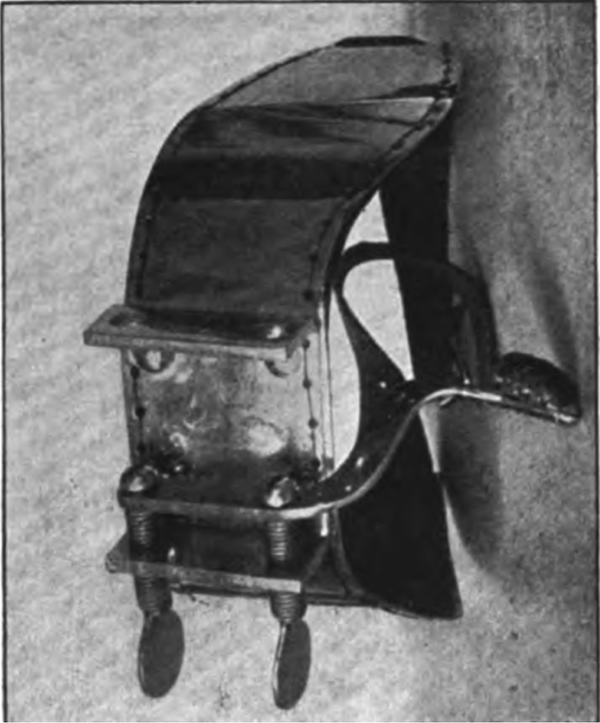
An external nasal splint devised for one of Dr Goodale’s patients. Reproduced from Goodale. 12
(Left) Preoperative. (Right) Postoperative. Reproduced with minor modifications from Goodale. 12
Goodale retired from active practice in 1938 and became interested in the management of a large apple orchard on his estate in Ipswich, Massachusetts. He passed on November 5, 1957. For the last few years, he lived with his son, Robert L. Goodale. 2
Oliver Ames Lothrop, MD, was born May 8, 1880, and was a graduate of Harvard Medical School in 1908 and younger brother of Howard Augustus Lothrop, surgeon-in-chief Boston City Hospital. Early in his career, Dr Lothrop served as Assistant Otologist at Massachusetts General Hospital. He graduated from Massachusetts Eye and Ear Infirmary in 1911 and served as an associate surgeon there until 1929 under Chief Harris P. Mosher, MD. He later become chief of the Ear, Nose, Throat Surgery at Newton-Wellesley Hospital until his retirement from active staff in 1946. He passed on May 12, 1963.13,14
His early work in 1910 consisted of defining the anatomy of the septum in relation to its surrounding structures in detail, while advocating submucous resection for “septal deflections” in all cases of dysmorphic nasal obstruction. 3 While it remains unclear if Lothrop had a relationship with Goodale, both he and Mosher similarly created a technically unique approach consisting of a high subdorsal septal excision, vault mobilization, and impaction to attenuate the nasal hump. These are outlined in his 1914 article “An operation for correcting the aquiline nasal deformity. The use of a new instrument. Report of a case.” 15
As it relates to preservation rhinoplasty, Lothrop described his technique as follows: (1) An incision was created down one side of the columella. (2) Submucous elevation was performed along both sides of septum under the nasal bones with mucoperichondrial elevation to the desired level beneath the nasal bones. (3) The cartilaginous septum was then resected as necessary for reconstruction of the bridge along with aesthetic resection of the perpendicular plate of the ethmoid. (4) Bony cuts were next made along the ascending process of the superior maxilla and nasal bone of one side as to facilitate a triangular shaped resection. This process was then repeated on the opposite side. (5) A lateral ostectomy was performed with the acute angle toward the frontal-nasal suture. (6) The nasal bones are fractured at the frontal-nasal suture allowing mobility and subsequent impaction of the bony structures in line with the previously fashioned septal cartilage.
A case report of the operation of patient G.J., a 30-year male medical student reported the following operative plan (Figures 6 and 7). The operation in total took a total of 40 minutes with improved functionality and three-eighths of inch nasal shortening. 15
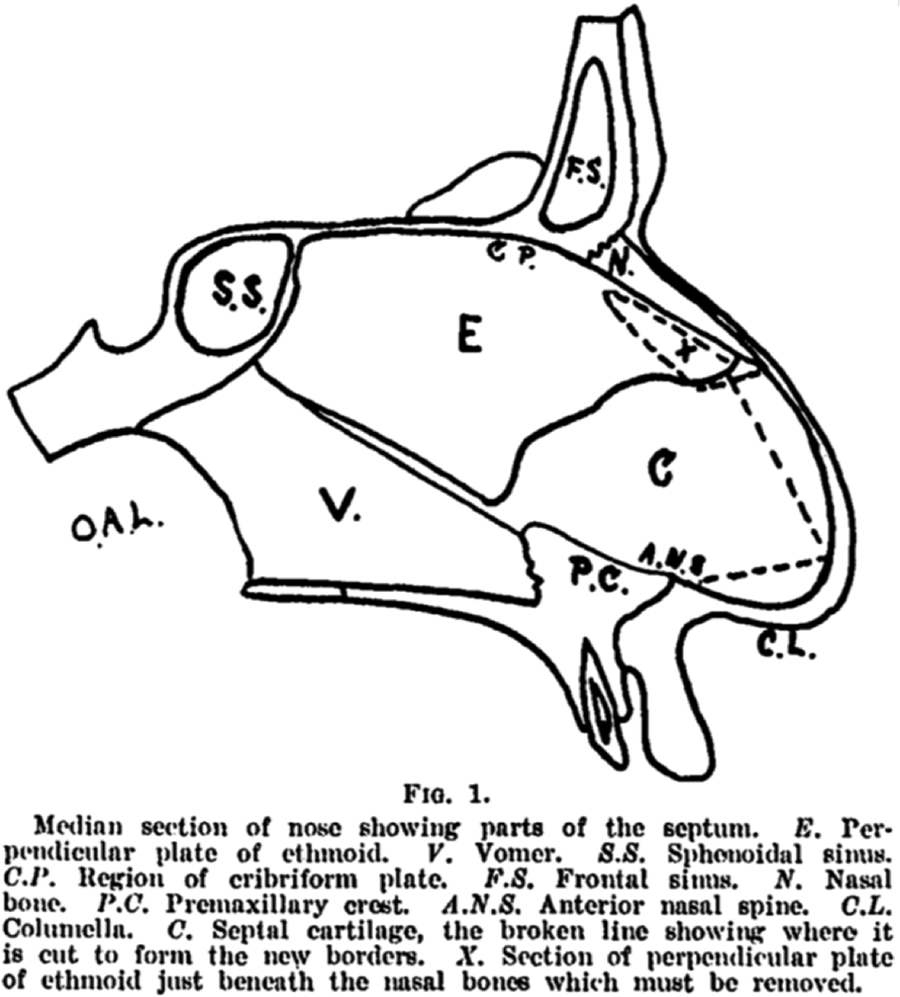
Medial septum with dotted lines defining cartilaginous septal resection and perpendicular plate ethmoidal resection. Reproduced from Lothrop. 15
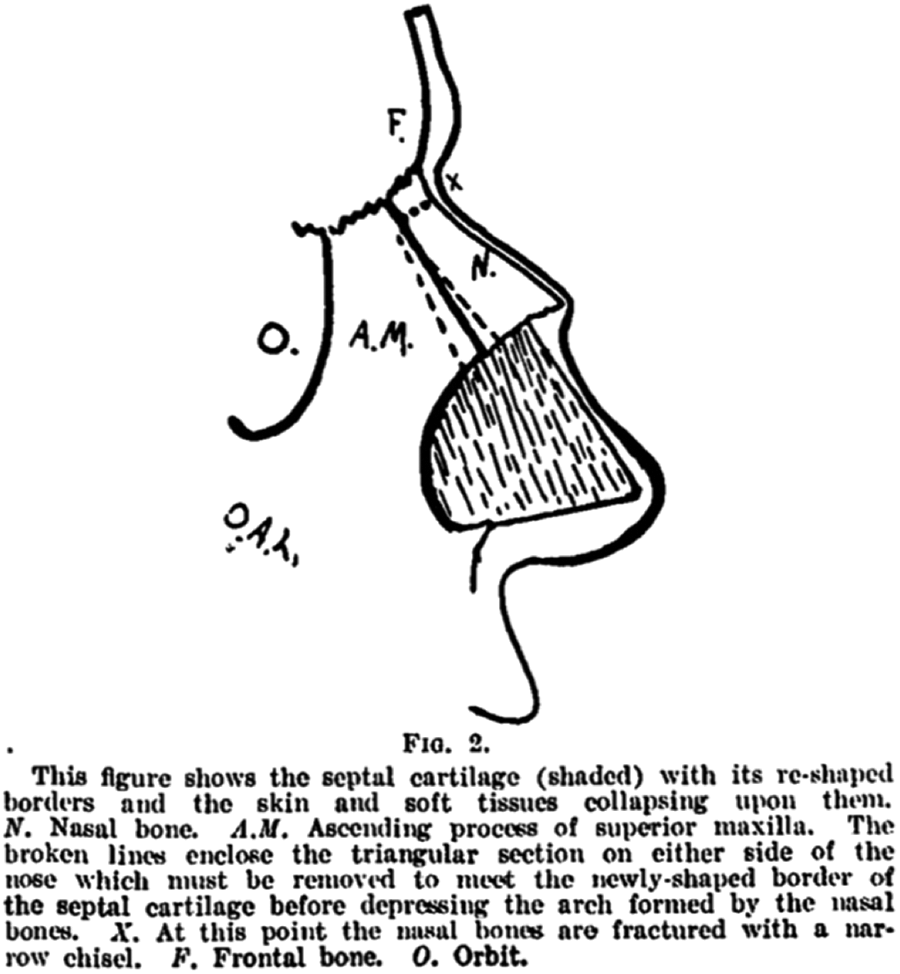
Dotted lines show triangular bone removed on either side of the nose to meet the newly shaped cartilaginous septum. “X” defines the point of nasal fracture. Reproduced from Lothrop. 15
Lothrop would expand on his characterization, thorough understanding of septal anatomy, and submucous resection within the realm of septal surgery implementing a scapula bone graft for traumatic or infective septal deformities. The case of patient J.J.B., a 21-year-old male (Figures 8 and 9) with suspected traumatic nasal injury is described as follows: (1) submucous resection of the septum, (2) resection of the vertebral border of the left scapula, (3) an incision halfway between the tip and columella to create a subdermal passageway along the bridge to the distal bony septum, (4) the distal nasal bones were rasped, and periosteum elevated. (5) The bone graft was positioned under the periosteum to the level of the frontal sinus proximally but before the nasal tip distally. The graft firmly affixed itself the underlying structures within 4 weeks. 16
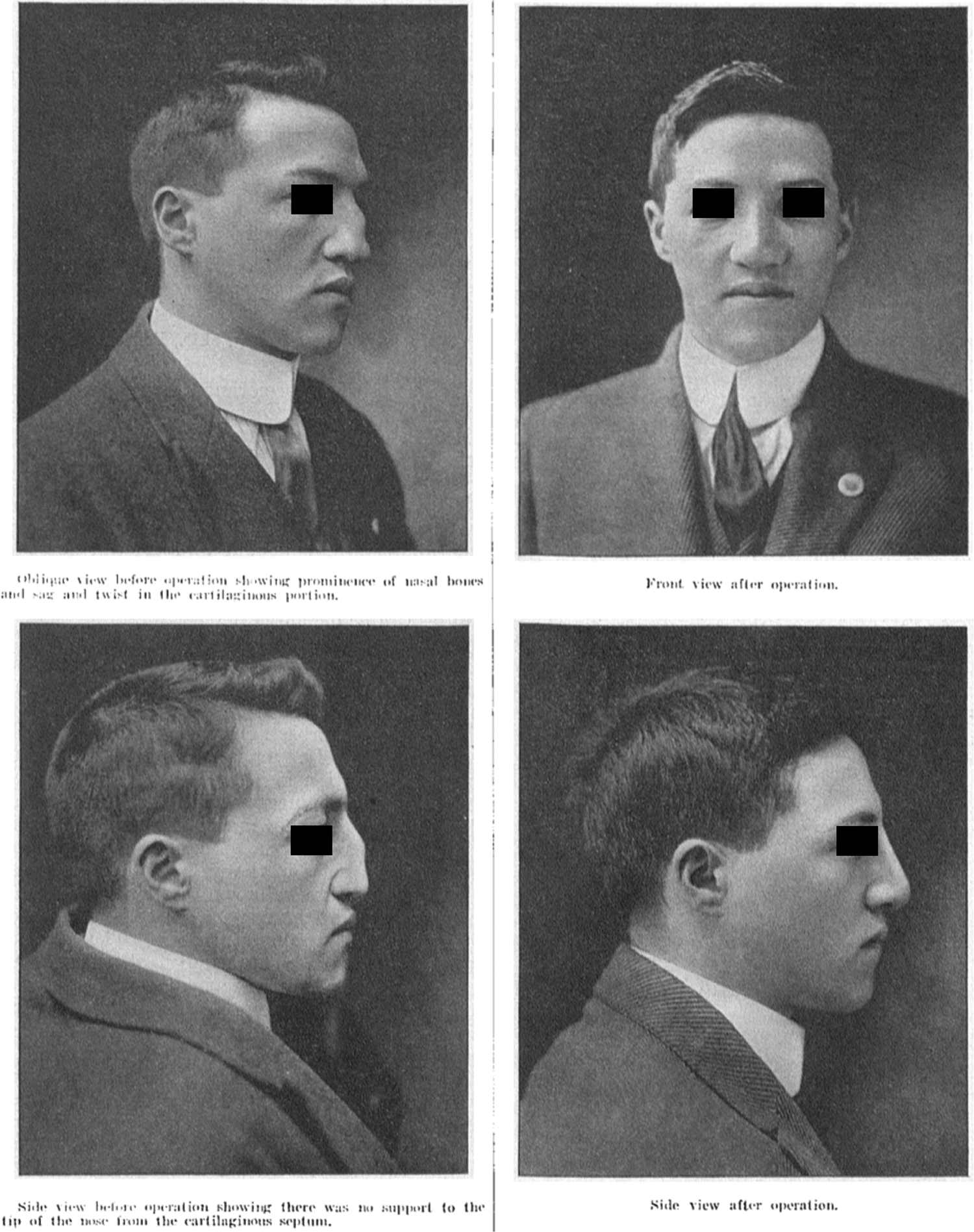
(Left column) Preoperative photos. (Right column) Postoperative results following scapula graft. Reproduced with minor modifications from Lothrop. 16
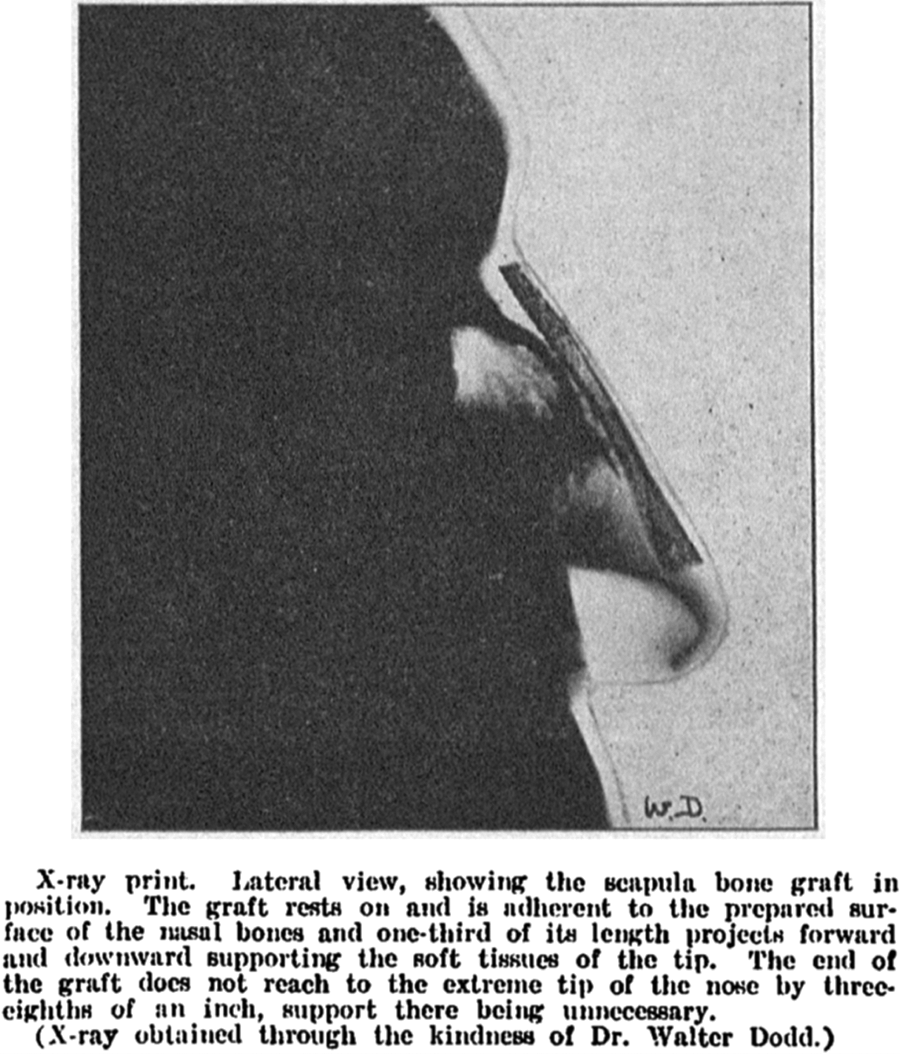
X-ray following scapula bone graft. Reproduced from Lothrop. 16
Maurice H. Cottle was born in England in 1898, immigrating to France in his youth, and finally moved to Chicago. He become Chief of Otolaryngology at Chicago Medical School and director of rhinology and rhinomanometry at Illinois Masonic Hospital and Medical Center for over 50 years. He was an integral part in the resurgence of the practice of rhinology and rhinological surgery in the mid-20th century following a brief loss in popularity decades prior. As the founder of the American Rhinological Society in 1954 and later the International Rhinologic Society in 1965, he was well-known by both peers and pupils as a principled investigator know to emphasize the importance of surgery as means of first, restoring appropriate nasal physiology, prior to consideration of aesthetic correction. 17
His work would be influenced by Jacques Joseph, who was known for his hump removal via V-shaped excisions and triangular excisions for nose shortening, Freer’s description of submucous resection of the nasal septum, and Mosher’s method of correcting lateral deformities of the nasal bone via external osteotomies with emphasis placed on manipulating the ascending process of the maxilla along with the septal cartilages. He would also consider the contributions of both Goodale and Lothrop to rhinological surgery important in reference to intranasal lateral osteotomies and the functional importance of the inferior turbinates, respectively.17,18
In his “Corrective surgery of the external nasal pyramid and the nasal septum for restoration of normal physiology,” Cottle characterizes Fomon’s approach to the external nasal pyramid, which arguably may be considered a foundational element to the Cottle’s “push down” operation, as influenced chiefly by deformities of nasal function. He first describes uncovering both the bony and cartilaginous vault, trimming of the caudal septum, breaking the “spring of the bony vault,” and trimming the upper lateral cartilages. For septal deformities, he describes left and right mucosal flaps, removal of both bony or cartilaginous deformities, and the replacement of any anterior septum to counteract the contracture noted during healing. In his conclusion, he stated, “Extensive pyramid and septal surgery may be combined when definitely indicated if provisions are made for attaching the septal mucosa to its anterior abutments.” 4 Importantly, with these observations and his paper on the maxilla-premaxilla approach, he recognized the importance of preserving the nasal dorsum and alongside its anatomical relationships. 19
Following these observations, he would expand this approach in 1954 in his “Nasal roof repair and hump removal” paper 4 where he noted the complete mobilization of the nasal pyramid in conjunction with lateral and transverse osteotomies allowing for a downward fracture or “push down,” closure of the valve area, and preservation of the upper lateral cartilages. The operation is described as follows: (1) A right hemitransfixion incision exposing the caudal septum and unilateral submucoperichondrial undermining and elevation to the level of the ethmoid and vomer creating a columellar pocket. This process was similarly performed on the opposite side creating a right and left septal flap. (2) A vertical septal strip is removed at the bony-cartilaginous junction. An inferior strip of cartilage or ethmoid may be removed at this point to facilitate the descent of the nasal dorsum. (3) Subperiosteal lateral osteotomies are then made via vestibular or alar incisions followed by fracturing of the lateral laminae eliminating the dorsal hump. (4) A transverse osteotomy from lateral to medial from inner canthus to the nasofrontal angle via a stab incision allowing for mobilization and rotation of nasal bones. (5) “Push down” of the nasal pyramid.20,21 Cottle also describes a Group 7 rhinoplasty group in which the surgeon makes every attempt “in doing the septum and the pyramid work to avoid injury or excision of any piece of tissue that can be spared to the end that function can be retained.” 22 He also describes a conservative “push-down” technique when necessary in this article.
Relevance of Original Preservation Rhinoplasty Techniques for Today
As with any new technique in medicine, there is a period of enthusiasm that is usually tempered with observation and caution.23,24 This holds true for the recent preservation rhinoplasty resurgence in Europe and the United States. In a recent article, authors noted the recurrence rate of dorsal prominence following preservation rhinoplasty techniques. 23 In this article, 63 of 520 patients experienced a recurrence of their dorsal prominence within 4 months (12%). 23 Clearly, having patients return within months after having a procedure with the initial cosmetic concern demonstrates the need for more understanding of what these procedures require for long-term results. Besides dorsal prominence recurrence, other risk factors such as cerebrospinal fluid leak due to the proximity of the ethmoid plate to the skull base, step-off deformities of the radix (due to the need to be able to “pushdown” the entire nasal dorsal framework into the maxilla), incorrect patient selection (patients with long nasal bones), and supratip depression. The proponents of preservation rhinoplasty state that dorsal preservation is only one form of preservation rhinoplasty. Indeed, there may be merits in other forms of cartilaginous preservation rhinoplasty techniques such as total cartilage preservation techniques in order to supplant more traditional columellar and alar strut grafts from other endogenous sources (septum, ear). In carefully selected cases (such as the broad, wide nose that is markedly deviated), preservation rhinoplasty techniques offer benefits to a patient over classic reduction/reconstruction grafting techniques.
Conclusions
As seen in these 3 preeminent rhinoplasty surgeons, their thought processes and techniques more than 100 years ago may be relevant today. Nonetheless, the rhinoplasty surgeon has a plethora of techniques from which to base their intraoperative plan upon, and careful patient selection continues to be paramount.
Footnotes
Authors’ Note
Joel Lee and Senan Abdul-Hamed are cofirst authors.
Acknowledgments
The authors would like to acknowledge authors Goodale and Lothrop for the use of their figures under the public domain.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.