
Abstract
Introduction
Malignant peripheral nerve sheath tumors (MPNSTs) are rare tumors that develop from peripheral nerve sheath cells, including Schwann cells and fibroblasts. They account for approximately 5% to 10% of all soft-tissue sarcomas,1,2 MPNSTs in the head and neck region represent approximately 2% to 6% of all head and neck sarcomas, 3 and account for 12% to 19% of all MPNSTs, 4 the infratemporal fossa is a rare site for MPNSTs. 5 MPNSTs originating from the trigeminal nerve are extremely rare, with only a few documented cases in medical literature, also these tumors are known for their aggressive nature, and often carrying a poor prognosis. 3 About 50% of MPNSTs occur in patients with neurofibromatosis type 1 (NF1), about 10% have a history of radiation, and 30% are mostly sporadic. 1
We reported a case of a 19-year-old female complaining of constant facial pain and paresthesia, further investigations revealed a lesion located at the infratemporal fossa, treated with surgical resection, intra-operation noticed that the lesion involved the mandibular branch of the trigeminal nerve, and the pathological examination and immunohistochemistry findings show high-grade MPNST.
Case Presentation
A 19-year-old female presented to the Otolaryngology clinic with a 6-month history of left-sided facial pain that has not responded to medication. She also reported experiencing paresthesia on the same side. The patient did not exhibit facial paralysis or swelling. Her medical history does not include any neoplastic conditions or exposure to radiation. In addition, she is a non-smoker and does not consume alcohol. There is no family history of tumors or hereditary diseases.
On examination, there was a left-sided facial paresthesia at the third trigeminal nerve (V3) area with no evidence of weakness on examination of motor branches of V3, the rest of cranial nerves, optical, oral, endonasal, and neck examinations were normal. The rest of the physical examination is within normal.
Computed tomography with contrast was done, showing a left-sided lesion located in the infratemporal fossa, extending from the skull base to the level of the ramus of the mandible without any signs of bone erosion (Figure 1).
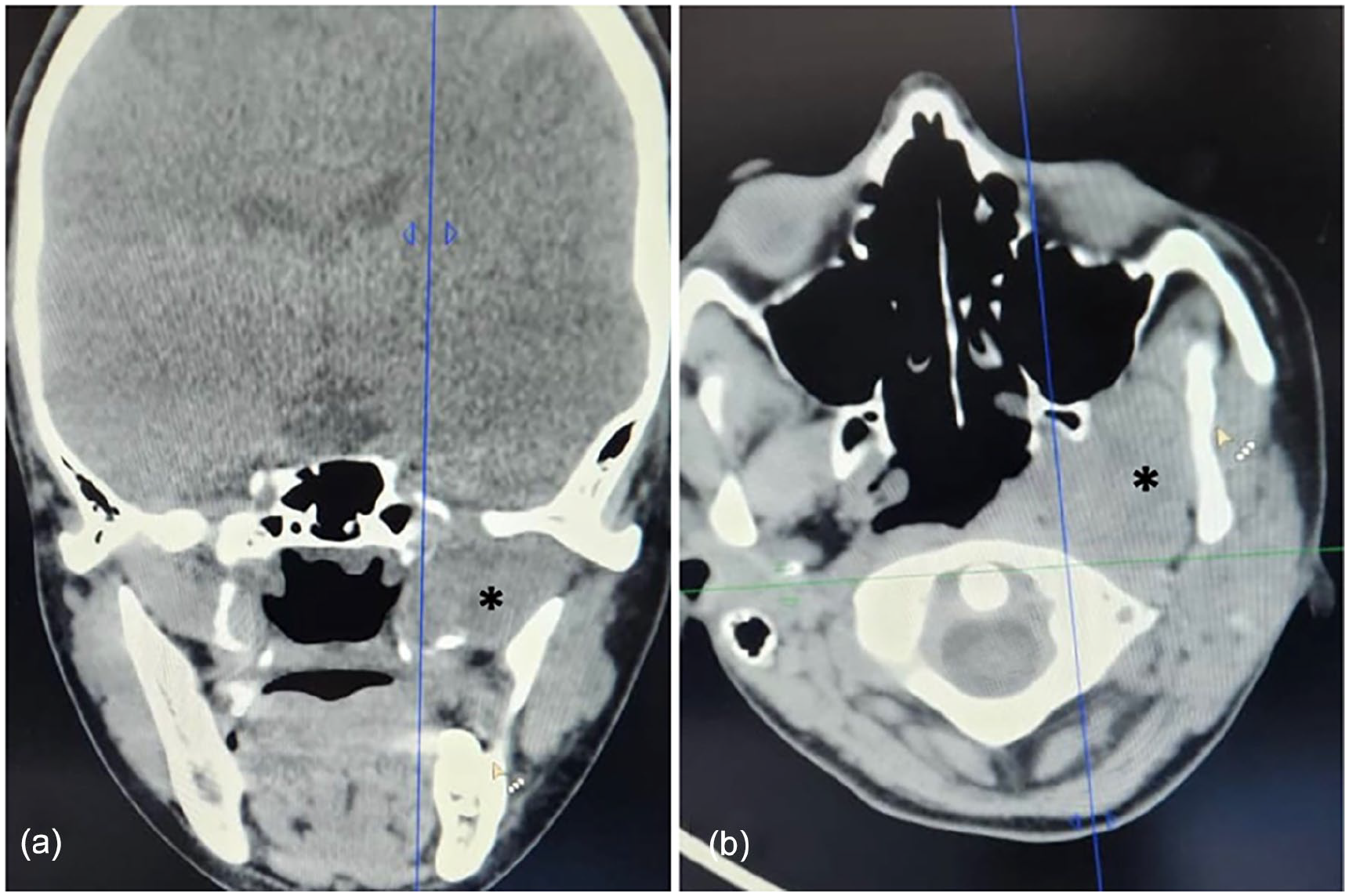
Coronal (a) and Axial (b) computed tomography showed a left-sided infratemporal lesion (asterisk).
Magnetic resonance imaging (MRI) with contrast was performed, showing a left-sided infratemporal lesion measuring 3 × 3.5 cm in transverse section and approximately 4.3 cm in length. The lesion exhibited low signal intensity on T1-weighted images and natural signal intensity on T2-weighted images. It extended through the foramen ovale, expanding it, and appeared as a small lesion in contact with the left Meckel’s cave at the base of the left middle cranial fossa, measuring about 1.5 × 1 cm (Figure 2).
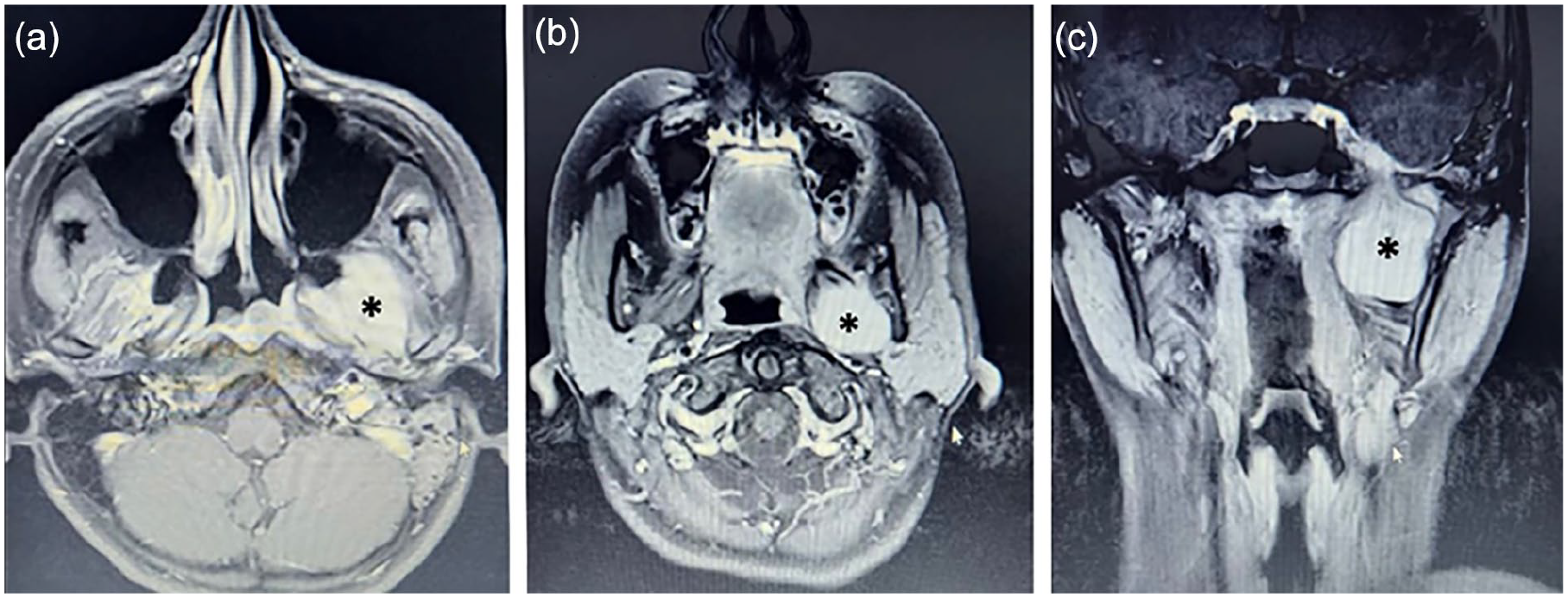
(a) MRI—axial T2-weighted image showing an infratemporal fossa lesion with natural signal intensity (asterisk), (b) axial contrast-enhanced T1-weighted image MRI, and (c) coronal contrast-enhanced T1-weighted image MRI showing an infratemporal fossa lesion (asterisk). MRI, magnetic resonance imaging.
The decision for surgical resection was made, under general anesthesia, the mandibular swing approach was done to access the infratemporal fossa, intraoperative, a capsulated lesion upon the mandibular branch of the trigeminal nerve with soft tissue attachments, the tumor was dissected from the attachments with foramen ovale and the intracranial portion was isolated and then was resected totally with the tumor, safety margin was 1 cm.
Histological examination showed grade spindle cell sarcoma; hypercellularity with high mitotic activity, and nuclear pleomorphism, the adjacent nerves show tumor transformation (Figure 3); the surgical margins could not be evaluated due to surgical fragmentation, however, focally close to the tumor, the immunostains were performed and showed positive S100 protein marker and Ki67 marker: labels >50% of cell, this finding showed high-grade MPNST.
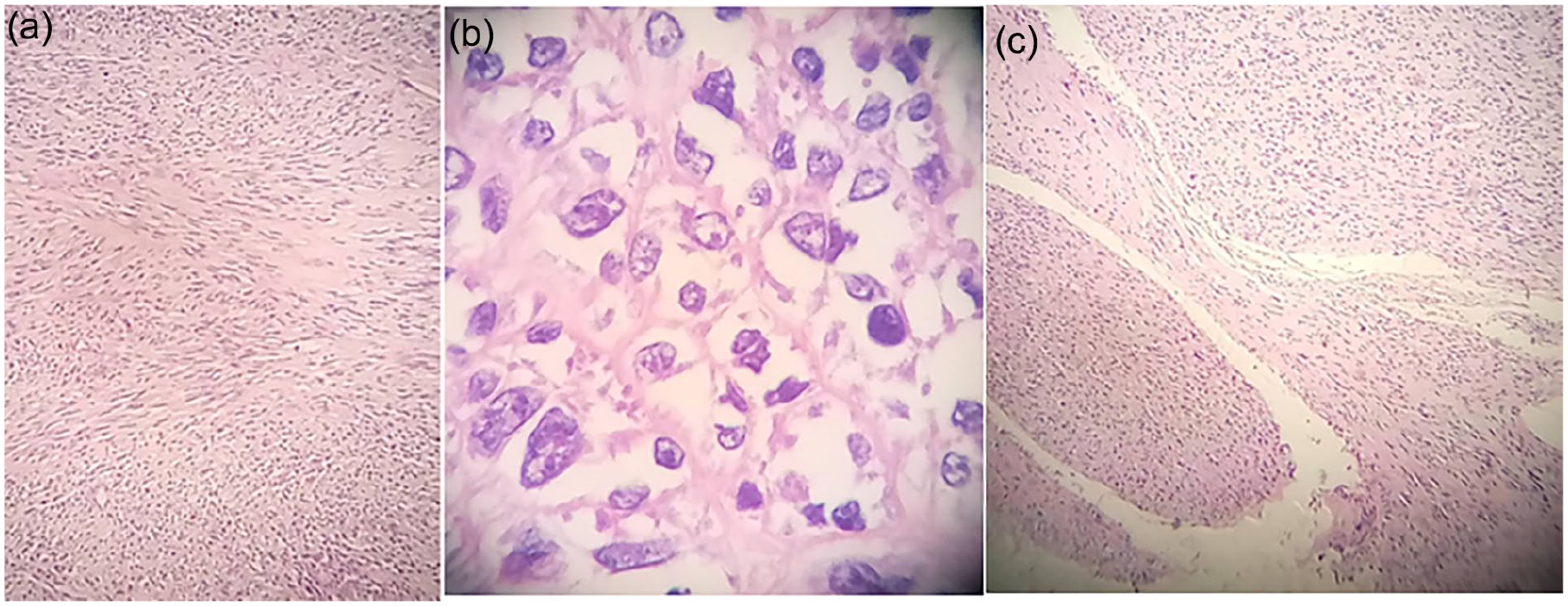
The histological microphotograph consists of MPNST. (a) and (b) show a high-grade spindle cell carcinoma and (c) show nerve involvement. MPNST, malignant peripheral nerve sheath tumors.
The patient was referred to an oncologist for initiation of radiotherapy. However, there was a delay of approximately 2 months before treatment commenced. During this period, a new MRI imaging study was conducted, revealing a local recurrence in the left Meckel’s cave. Subsequently, the patient underwent a second surgery by a neurosurgeon and was then referred for radiation therapy.
Discussion
MPNSTs refer to malignant tumors of the peripheral nerve sheath cells that originate from Schwann cells and fibroblasts. 1 A sarcoma is classified as an MPNST when it meets one of the following criteria: originates from a peripheral nerve, arises from a preexisting benign nerve sheath tumor (neurofibroma), or shows Schwann cell differentiation upon histological examination. 6
MPNSTs typically impact individuals aged between 20 and 50 years, with no specific gender predilection. 7 However, Schmidt et al observed a higher incidence of trigeminal MPNSTs in male patients, with a tendency for left-sided lesions. 3 Approximately 50% of MPNST cases are associated with NF1, while around 10% are linked to prior radiation exposure, and the remaining 30% are predominantly sporadic. 1 While the presence of neurofibromatosis (NF) significantly elevates the risk of developing MPNSTs overall, it is noteworthy that its influence on MPNSTs involving cranial nerves remains inconclusive. 3 This article describes a case of a 19-year-old female with left-sided MPNST involved in the V3 and located at the infratemporal fossa with a negative history of NF or radiation exposure.
MPNSTs can manifest with a diverse array of symptoms. 3 Ma et al reported that pain was the predominant symptom among patients with a history of NF1, whereas a rapidly growing mass was the primary complaint in those without NF1. 5 In addition, Schmidt et al noted that a significant proportion of patients with trigeminal MPNSTs presented with altered facial sensation and/or facial pain distributed along the affected division area. Moreover, weakness in the mastication muscles was observed in several cases. 3 Our patient has suffered from facial paresthesia and pain along the V3 area without any sign of muscle weakness or facial swelling.
The diagnosis of MPNSTs requires pathological analysis of biopsy specimens but there are various methods available to aid in the diagnosis of MPNSTs. 3 MRI is commonly used to evaluate soft tissue sarcomas, MRI images of MPNST revealed a low signal in T1WI and a strong signal in T2WI. Unusual signs, such as invasion of fat planes, heterogeneity, ill-defined margins, and edema surrounding the lesion, have been associated with MPNSTs. 1 On the other hand, high-resolution computed tomography scanning is also considered effective for imaging as it reveals the pushing borders of the tumors, rather than the invasive character of malignancy. 7
Primary MPNSTs are typically treated with surgical resection as the recommended treatment, aiming for complete removal with clear margins 8 followed by postoperative radiotherapy. 3 Microscopically, MPNSTs have a variety of morphologies that are not specific for diagnosis but aid in differential diagnosis. Immunohistochemistry analysis is based on the diagnosis of exclusion. S-100 is a crucial marker for Schwann-associated tumors, yet its reliability in MPNSTs is limited, with a positivity rate of only 50% to 60% due to inconsistent Schwann cell differentiation. The Ki67-labeling index is essential for the assessment of NF1 patients, Ki67 levels of 2% to 5% are seen in ordinary and atypical neurofibromas, while levels of >10% may indicate MPNSTs. 1 MPNSTs generally have a poor prognosis. Studies indicate that the 5-year overall survival rate hovers around 50% to 60%, with a median survival time of 6 years for patients with MPNST. 1
Conclusion
MPNSTs in the head and neck region may manifest with nonspecific symptoms. Persistent symptoms that do not improve should prompt further investigation for an underlying issue. MPNST diagnosis is challenging, often requiring a combination of clinical, pathological, and immunohistochemistry studies. Treatment of MPNSTs remains difficult. Total surgical resection is considered the most effective treatment, often supplemented with adjuvant radiotherapy.
Footnotes
Author Contributions
M.A.: validation, writing – review and editing, visualization, methodology, software, writing – original draft, formal analysis. L.K.: validation, formal analysis, writing review and editing. A.A.: supervision, writing – review and editing, project administration.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval
Written informed consent was taken from the patient for publication of this article.