
Abstract
Introduction
Researching web resources on health-related topics has become quite common, and YouTube is a very popular platform as it provides information both visually and audibly. However, since videos can be uploaded to this platform by anyone and there is no need for preliminary review, conformity, or reliability approval, patients may access incorrect information. As a result, various reliability and quality scales have been developed. DISCERN, modified DISCERN, Journal of the American Medical Association (JAMA), Global Quality Score (GQS) are commonly used scales for both video content producers and professional videos uploaded for educational purposes.1-3 More specific scales such as LAParoscopic surgery Video Educational GuidelineS (LAP-VEGaS) and Instructional Videos in Otorhinolaryngology by YO-IFOS (IVORY), which only evaluate the quality and reliability of educational videos, have been discovered recently, and the number of studies in this area is quite limited.4,5
The LAP-VEGaS scale, which was published in 2018, is valid for all laparoscopic surgical procedures and has been used to evaluate the quality and reliability of videos of many operations such as the gastrectomy, thoracoscopic lobectomy, and hysterectomy.6-8
The IVORY guideline, which was published in 2020, provided recommendations to produce surgical videos specifically for educational purposes in otolaryngology.
The most performed surgical procedure for the treatment of epiphora due to nasolacrimal duct obstruction is dacryocystorhinostomy (DCR). Endonasal endoscopic DCR (EE-DCR) and external DCR are the 2 basic forms of DCR. The success rate has increased to 80% to 95%.9,10 This increase has been attributed to the development of endoscopic skills and the introduction of medical devices such as endoscopes and illuminators.10,11 The success rate of EE-DCR depends on anatomical factors (lacrimal sac size, nasal cavity size, presence of nasal septum deviation, middle turbinate hypertrophy), duration of the disease, surgeon experience, and skill level.12-14 Variables that can be improved among these factors are experience and surgical skill.
Video-based surgical training has been shown to be educationally beneficial. 15 Therefore, surgical videos are highly viewed in preparation for otolaryngology surgeries. In terms of DCR, there is no previous study with the IVORY scale. We aimed to evaluate DCR training videos useful for clinical practice with these 2 current scales and to determine the correlation between these 2 scales.
Methods
Evaluation of the General Characteristics of the Videos
Videos were searched on the YouTube website (http://www.youtube.com) on June 1, 2024, with the keywords “endoscopic dacryocystorhinostomy, endoscopic DCR.” The “most viewed” filter was used to determine videos that reached the most people, and 61 videos that were viewed over 1000 times were included in the study. Videos that were not in English had limited access, had repetitive versions, and were shorter than 1 minute were not included in the study. URLs of all videos that met the inclusion criteria were recorded, and all preliminary searches were reviewed separately by 2 experienced otolaryngologists.
The number of days since the videos were uploaded to YouTube, their duration (seconds), upload source, total number of views, number of likes, number of dislikes, and number of comments were evaluated. Like rate was calculated as the number of likes/[number of likes + number of dislikes]; view rate was measured as the number of views/number of days since the video was uploaded; and video power index was assessed as [like rate × view rate]/100.
Evaluation of Videos According to the LAP-VEGaS
The LAP-VEGaS was used to assess each video. The 9 items are evaluated and scored on a scale of 0 (not present) to 2 (presented completely). 4 Supplemental Table 1 shows the items of LAP-VEGaS scoring system. This score is used to classify videos into low (0-6), medium (7-12), and high (13-18) educational quality groups.
Evaluation of Videos According to the IVORY
The quality of the videos and whether they were suitable for surgical training were evaluated according to the IVORY. Two different scoring systems were used for the IVORY grading assessment. The first (IVORY-1) was an assessment consisting of 21 items and scored out of 42 points. In the IVORY-1 scoring system, B section item 9, D section items 13, 14, and 17 were removed from the original IVORY grading system, and items 20 to 25 were added to section E, which assessed the suitability of surgical steps in the organ-specific section. Items 20 to 25 of section E were used in the IVORY-2 scoring system. Six items, including the order and appropriateness of surgical steps, were evaluated out of 12 points. Supplemental Table 2 shows the items of IVORY-1 and IVORY-2.
Section B, item 9 (there is no standardized peer review process for uploading videos to YouTube), Section D, item 13 (the patient’s placement and position were standard), Section D, item 14 (the surgical instruments used in standard EE-DCR procedures are well defined), and Section D, item 17 (there was no pathology material during the EE-DCR) were excluded.
Section E of the IVORY guidelines includes recommendations specific to otology, functional endoscopic sinus surgery, airway surgery, vocal cord surgery, plastic surgery, and cosmetic surgery only. Therefore, we modified Section E according to the surgical steps described in the article titled “Endoscopic Dacryocystorhinostomy” in Cummings Otolaryngology Head and Neck Surgery. 16
The total score obtained was graded from A to F according to the academic grading system of the United States. 17 Since our aim was to evaluate the videos for continuing medical education, 2 experienced otolaryngologists independently evaluated the videos according to the newly introduced IVORY grading system. In case of disagreement, a consensus grading result was determined after extensive discussions.
Statistical Analysis
SPSS version 27.0 (IBM Corp., Armonk, NY, USA) was used for statistical analysis. Descriptive data were presented as numbers (percentage), medians, and minimum–maximum (min–max) values. The distribution of the data was evaluated with the Kolmogorov–Smirnov test. For a normally distributed data, the comparison between the 2 groups was made with the Mann–Whitney U-test. The Spearman correlation analysis was performed for non-parametric numerical variables. Linear regression analysis was used for parametric numerical variables. P < .05 was considered statistically significant.
This study was prepared in accordance with the principles of the Declaration of Helsinki and does not require ethics committee approval because it does not include studies on patients or animals.
Results
Basic Characteristics of Videos
A total of 61 EE-DCR videos were evaluated. The videos were produced between March 2009 and March 2023. The country with the most videos uploaded is India [25 videos (41%)] (Figure 1). All the videos were uploaded to the YouTube by healthcare providers. The mean duration of the videos was 11.68 (SD ± 12.16) minutes. The number of views was 15.659 (SD ± 38.097), the mean number of likes per video was 85.37 (SD ± 129.96), and the mean number of dislikes was 4.27 (SD ± 9.46). Table 1 displays other video characteristics.
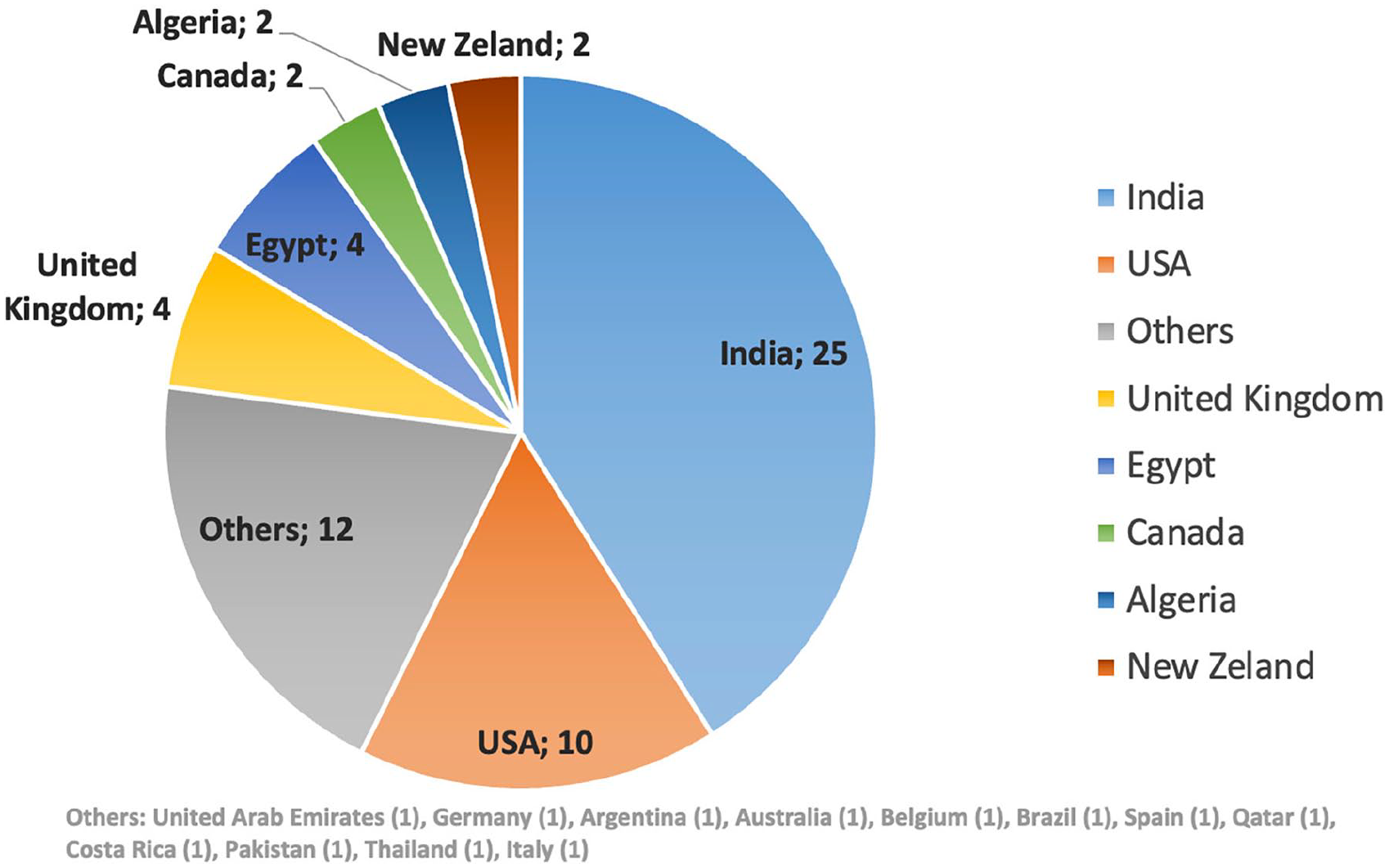
Country origin and numbers of EE-DCR videos. EE-DCR, endonasal endoscopic dacryocystorhinostomy.
Characteristics of YouTube Videos About EE-DCR.
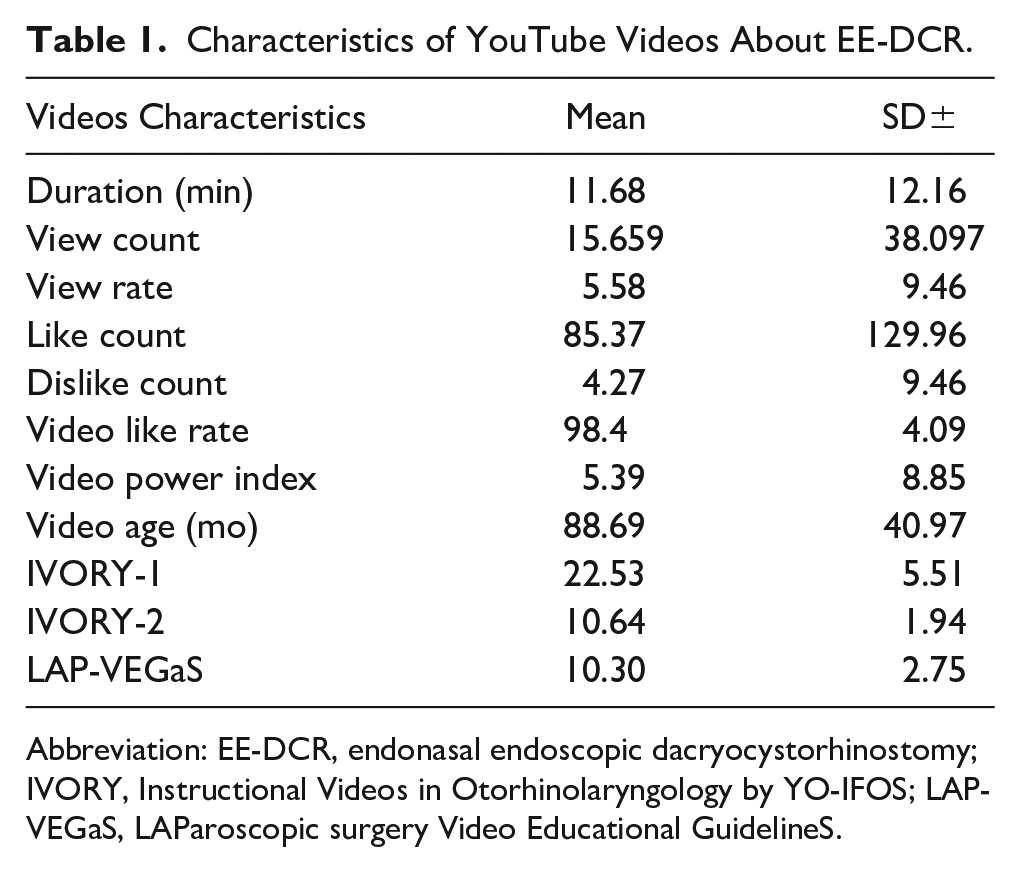
Abbreviation: EE-DCR, endonasal endoscopic dacryocystorhinostomy; IVORY, Instructional Videos in Otorhinolaryngology by YO-IFOS; LAP-VEGaS, LAParoscopic surgery Video Educational GuidelineS.
LAP-VEGaS and IVORY Grading System
The mean score of LAP-VEGaS was 10.3 (±SD 2.7). According to LAP-VEGaS grading, 5 (8.2%) videos were in low, 42 (68.9%) were in medium, and 14 (23%) were in high quality.
The mean IVORY-1 total score was 22.5 (min: 10, max: 36, SD: 5.5). The mean value of IVORY-2 was 10.6 (min: 2, max: 12, SD: 1.94). The distribution of videos according to IVORY-1 grading system in academic grades is shown in Table 2.
Distribution of Videos According to IVORY-1 Grading System in Academic Grades.
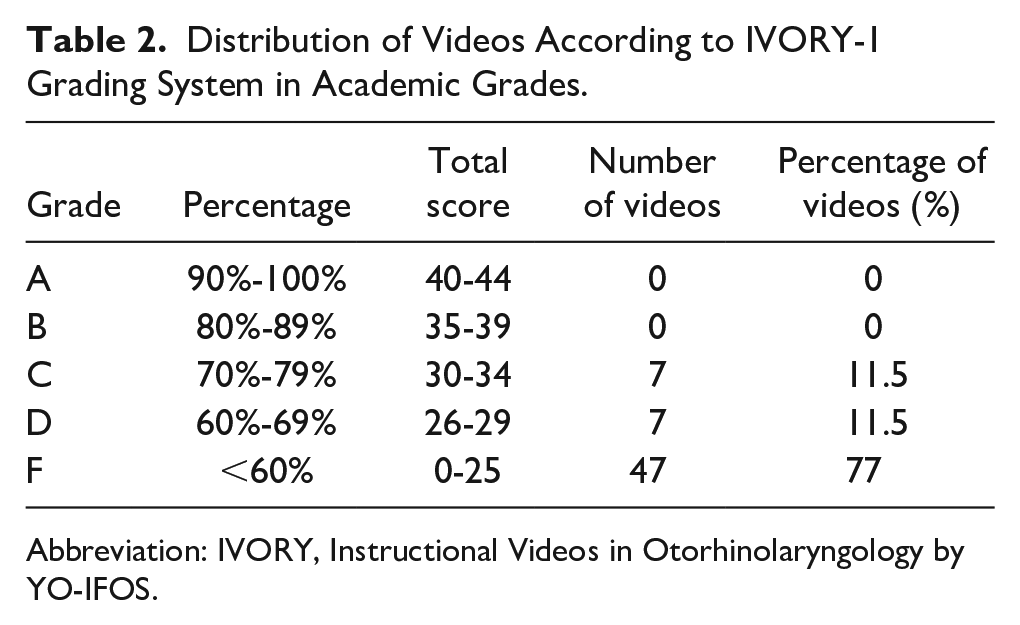
Abbreviation: IVORY, Instructional Videos in Otorhinolaryngology by YO-IFOS.
Correlation analysis revealed a statistically significant correlation between the IVORY-1 total score and the number of likes (P = .012, Spearman’s ρ = 0.327), the duration of the video (P = .012, Spearman’s ρ = 0.325), the age of the video (P = .002, Spearman’s ρ = −0.400), and the LAP-VEGaS score (P < .001, Spearman’s ρ = 0.639). No significant correlation was found between total number of views (P = .789, Spearman’s ρ = 0.036) and video power index (P = .105, Spearman’s ρ = 0.215) (Table 3).
Correlation Between IVORY-1 Total Score and Video Characteristics.
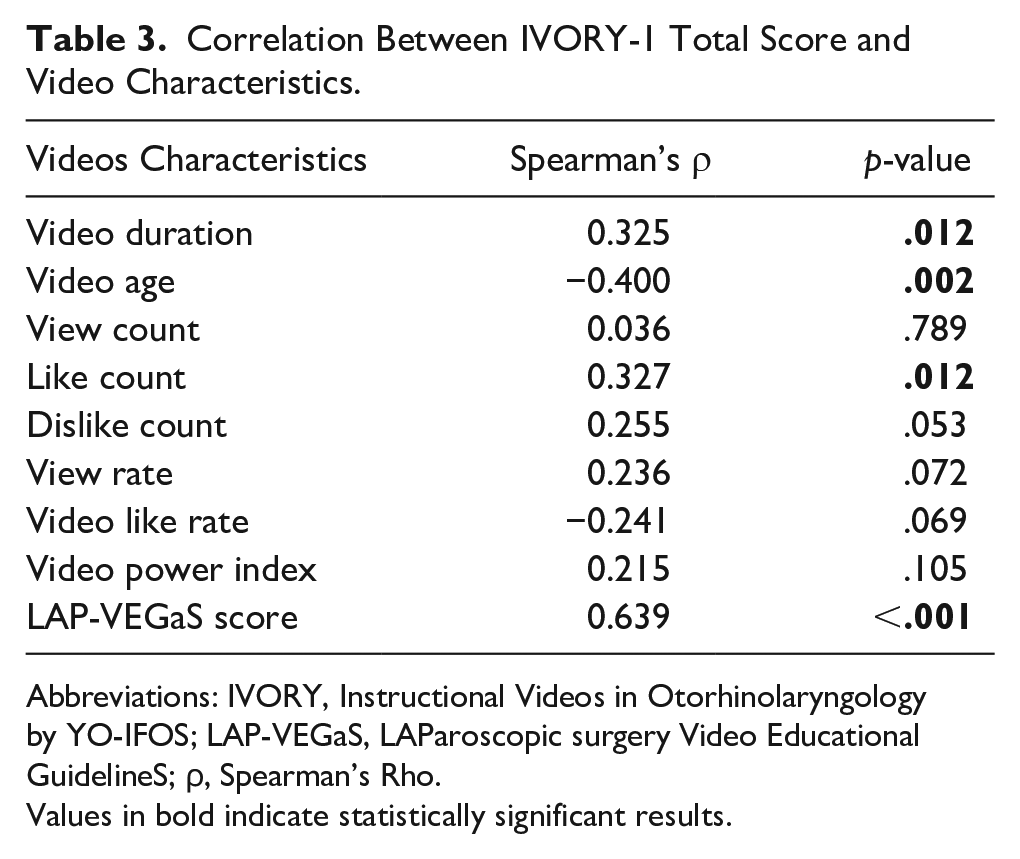
Abbreviations: IVORY, Instructional Videos in Otorhinolaryngology by YO-IFOS; LAP-VEGaS, LAParoscopic surgery Video Educational GuidelineS; ρ, Spearman’s Rho.Values in bold indicate statistically significant results.
There was a significant association between LAP-VEGaS categories and the IVORY-1 total score (P < .001). The mean IVORY-1 score for low-quality videos was 12.7, compared to 26.7 for medium-quality videos and 36.00 for high-quality videos, according to LAP-VEGaS video quality categories.
Linear regression analysis demonstrated that higher IVORY-1 scores predicted longer video duration (P = .008), newer video age (P < .001), and more LAP-VEGaS score (P < .001) (Table 4).
Linear Regression Analysis Between IVORY-1 Total Score and Video Characteristics.
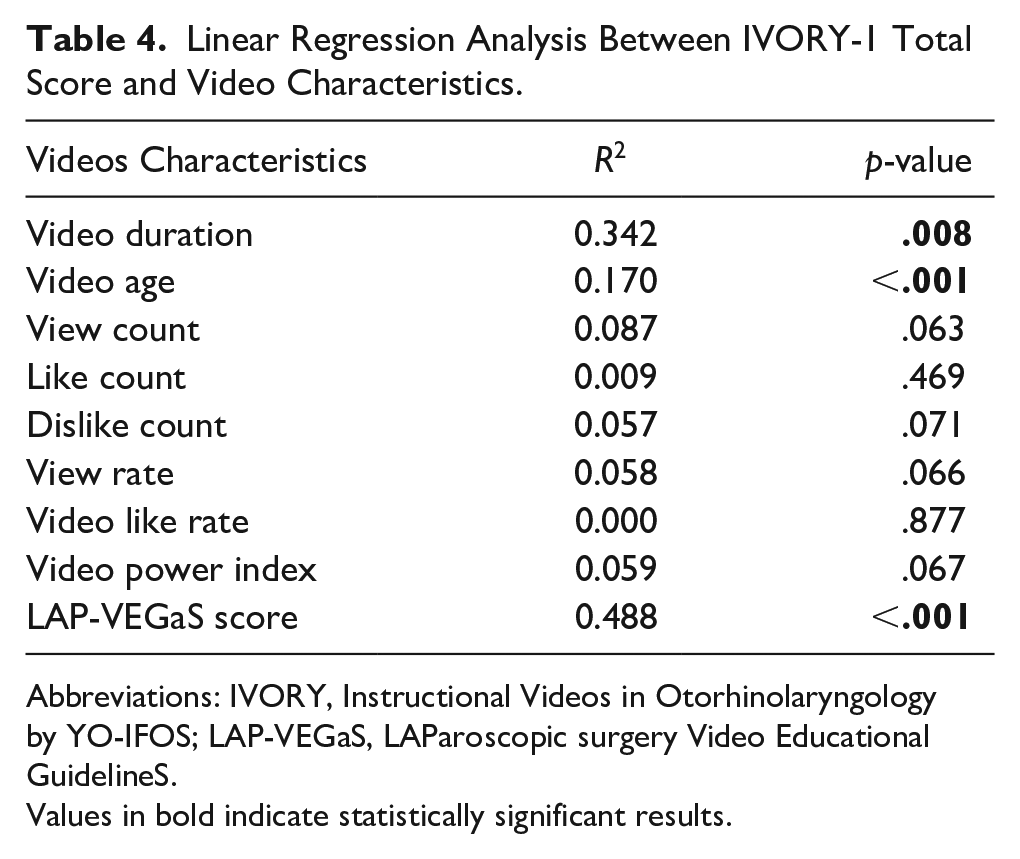
Abbreviations: IVORY, Instructional Videos in Otorhinolaryngology by YO-IFOS; LAP-VEGaS, LAParoscopic surgery Video Educational GuidelineS.
Values in bold indicate statistically significant results.
Discussion
Although YouTube and social media platforms were initially used by the public for communication and entertainment purposes, today they are also frequently used for getting information and briefing purposes. In our study, we aimed to evaluate the quality of EE-DCR videos on YouTube, a popular platform. We investigated the correlation between the LAP-VEGaS and IVORY scales and the usability of both scales in evaluating surgical videos on YouTube. Our study showed that higher IVORY-1 scores, in other words, higher-quality videos, were associated with longer video duration, and newer video age (Tables 3 and 4). We also found that LAP-VEGaS and IVORY-1 scale scores demonstrated a strong correlation when evaluating the quality of the videos.
Previously, surgical training videos in both head and neck and other disciplines have been evaluated in many studies using various evaluation methods and scales, such as DISCERN, Modified DISCERN, JAMA, and GQS.18-22 In only one study, evaluating the quality and reliability of DCR videos on YouTube as a patient education source using the JAMA, DISCERN, and HON scales, Singh et al 22 found that the quality and reliability of these videos were low. In 2018, the LAP-VEGaS scale was released, and the quality of the videos and their suitability for education were assessed through this scale. Many publications were published in various surgical branches and in head and neck surgery using the LAP-VEGaS scale, and the overall quality of the surgery training videos was low to medium.19,23-25 Dikmen et al 23 evaluated external and endoscopic dacryocystorhinostomy videos on YouTube and reported that 59.4% of the videos were of low-to-medium quality. De La Torre et al 24 evaluated endoscopic endonasal approaches in otolaryngology videos on YouTube and found 69.7% of the videos as low-to-medium quality. Similarly, Wu et al 19 searched functional endoscopic sinus surgery videos on YouTube and showed that 70.3% of the videos were low-to-moderate quality. In another study, Luu et al 25 investigated neck dissection videos on YouTube and found that 91.9% of the videos were low-to-moderate quality. In our study, similar to other studies, we found that 77.1% of the videos were low-to-medium quality.
The IVORY scale, specially developed for head and neck surgery videos, was released in 2020. 5 No other publication was found except a study where IVORY and parotidectomy surgical YouTube videos were evaluated. 26 In our study, we evaluated both the quality and educational suitability of EE-DCR videos on both scales and the correlation between them. As far as we know, this is the only study to evaluate EE-DCR YouTube videos using the IVORY scale and the LAP-VEGaS scoring system.
Mayer et al 26 evaluated parotidectomy videos on YouTube and found a mean overall IVORY score of 24.9 (maximum score of 44). Similarly, we found a mean IVORY-1 score of 22.5 (maximum score of 42). This result is consistent with the first study in the literature in which Mayer et al evaluated YouTube parotidectomy videos on the IVORY scale. Mayer et al 25 also identified 1 (2%) of the videos as A, 1 (2%) as B, 11 (22%) as C, 8 (16%) as D, and 29 (58%) as E according to the American Academic Grading System. We found 7 (11.5%) of the videos in our study as C, 7 (11.5%) as D, and 47 (77%) as E. In our study, we could not determine the video quality of A and B grades. These findings showed that the videos are generally low-to-medium quality.
The correlation between the LAP-VEGaS scale scores and the characteristics of the videos has shown different results in the literature. Wu et al 19 discovered a positive correlation between the number of likes, video length, and LAP-VEGaS scores, whereas Dikmen et al 23 identified a positive correlation between view ratio and the presence of a narrator’s voice. Conversely, Luu et al 25 found no correlation between total view count, video age, or likes/dislikes and LAP-VEGaS scores. They did, however, observe a moderately positive correlation between the presence of audio or written commentary and LAP-VEGaS scores. De La Torre et al 24 similarly reported no correlation between LAP-VEGaS scores and views, comments, or likes. Chapman et al 6 also found no correlation between LAP-VEGaS scores and views, video length, or upload date. Mayer et al 26 established a statistically significant correlation between total views, likes, and IVORY likes. However, they found no meaningful correlation between total scores, video length, or age. Our study demonstrated that higher IVORY-1 scores, in other words, higher-quality videos, were associated with higher LAP-VEGaS scores, more likes, longer video duration, and newer video age (Table 3).
In our study, we found the IVORY-1 average score of 22.5 (±SD 5.5) out of a maximum of 42 points, and the IVORY-2 score of 10.6 (±SD 1.94), out of a maximum of 12. When the average scores of IVORY-1 and IVORY-2 were assessed separately, the surgical training videos were found to show mostly surgery scores but lacked patient information and history, enlightened approval, conflict of interest, appropriate diagrams for anatomy, tips to look at during surgery, etc. Given that the upload dates of the videos are currently very high the IVORY and LAP-VEGaS scale scores are increasing, with the spread of such criteria, it is likely that video uploads will be more careful about items outside the surgical stages.
We compiled the scales of the EE-DCR operation and the score of the IVORY-2 scale based on the section “Endoscopic Dacryocystorhinostomy.” 16 In order to ensure that there are no differences between the studies and to produce more standard surgical training videos, we propose the expansion and improvement of the subsection of the IVORY scale “E (Organ Specific) Section.” In subsequent studies and guides, the organ-specific section in the IVORY grading system can be developed and detailed. Thus, we believe that videos with more standard features and higher quality can be produced for surgical education.
Our study has several limitations. First of all, we evaluated a limited number of videos. Second, since most of the videos originate from 2 countries, selecting videos that are more evenly distributed may affect the results. Third, YouTube is a social media and entertainment platform rather than an educational platform. Healthcare professionals who upload videos may have uploaded these videos not only for surgical education purposes but also for patient information and advertising purposes. Therefore, it may not be correct to evaluate videos directly according to certain scoring systems. In addition, since the majority of the videos evaluated in the study were uploaded before the LAP-VEGaS and IVORY scoring systems were published, their quality may have been found to be low or medium. The high-quality level of the newer videos may support this situation. Additionally, further investigations may be focused on detailing the specific features of the videos that rated more highly on their utilized scales to help to guide educators on how to develop useful educational videos.
Conclusion
The quality of EE-DCR videos is generally low to moderate. The IVORY and LAP-VEGaS guidelines were found to be correlated with each other. Both scales can be used to evaluate EE-DCR videos and otolaryngology surgical education videos in general. We believe that guidelines such as IVORY and LAP-VEGaS may be developed to improve the quality of surgical education videos.
Supplemental Material
sj-docx-1-ear-10.1177_01455613241293867 – Supplemental material for Evaluation of the Educational Quality of Endonasal Endoscopic Dacryocystorhinostomy Videos on YouTube with IVORY and LAP-VEGaS Guidelines
Supplemental material, sj-docx-1-ear-10.1177_01455613241293867 for Evaluation of the Educational Quality of Endonasal Endoscopic Dacryocystorhinostomy Videos on YouTube with IVORY and LAP-VEGaS Guidelines by Mitat Selçuk Bozhöyük and Levent Yücel in Ear, Nose & Throat Journal
Supplemental Material
sj-docx-2-ear-10.1177_01455613241293867 – Supplemental material for Evaluation of the Educational Quality of Endonasal Endoscopic Dacryocystorhinostomy Videos on YouTube with IVORY and LAP-VEGaS Guidelines
Supplemental material, sj-docx-2-ear-10.1177_01455613241293867 for Evaluation of the Educational Quality of Endonasal Endoscopic Dacryocystorhinostomy Videos on YouTube with IVORY and LAP-VEGaS Guidelines by Mitat Selçuk Bozhöyük and Levent Yücel in Ear, Nose & Throat Journal
Footnotes
Data Availability Statement
The data that support the findings of this study are available from the corresponding author upon request.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval
Ethical approval for this article was not required because the study was not included any patient and patient information.
Informed/Patient Consent
Informed/patient consent in this article was not required because the study was not included any patient and patient information.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.