
Abstract
Introduction
Temporomandibular disorder (TMD) is a broad term that includes functional and pathological problems in the masticatory muscles, the temporomandibular joints (TMJ), and surrounding structures.1,2 Symptoms of TMD include restricted mandibular movements, pain in the masticatory muscles or TMJ, joint noises, myofascial pain, and restricted mouth opening. 2 Complaints such as headache, neck pain, tinnitus, and ear pain are also associated with TMD. 2 Epidemiological studies show that TMD affects more than 5% of the population, and 60% have at least 1 symptom.2,3 It is a condition that typically occurs between the ages of 20 and 40 and is twice as common in women as in men.2,3
Studies have demonstrated that individuals with TMD exhibit a higher incidence of otological symptoms.4,5 Significant associations have been identified between TMD and conditions such as tinnitus, ear pain, hearing loss, and vertigo. 4 The most prevalent otological symptom associated with TMD is ear fullness, reported in 74.8% of cases, followed by otalgia (55.1%), tinnitus (52.1%), vertigo (40.8%), and hearing loss (38.9%). 5 It is essential for TMD patients to receive treatment according to established guidelines, and those presenting with otological symptoms should be referred to an otolaryngologist. 6
Tooth loss can cause TMJ problems, loss of occlusal support, and degenerative changes. 7 Studies have shown tooth loss is associated with clicking and crepitation in the TMJ. 8 As the duration of edentulism, the number of missing teeth, and the number of relevant quadrants increase, dysfunction symptoms become more common.7-10 Partial edentulism may be one of the causes of TMD-related conditions such as myofascial pain dysfunction syndrome. 11
There is a close anatomical relationship between the cervical spine and the TMJ, and it has been suggested that changes in posture may contribute to TMD.12,13 Poor head posture can lead to adaptive shortening or lengthening of the muscles of the craniocervical region and limited movement in the atlanto-occipital joint. 14 This can lead to increased tension in the suboccipital tissues, resulting in TMD. 15 Furthermore, it is possible that forward head posture may play an important role in the development of TMJ pain in TMD. Therefore, it is important to consider the effect of abnormal head and cervical posture in the clinical treatment of TMD-related TMJ pain. 16
Changes between the masticatory muscles, cervical spine, and teeth are believed to cause postural imbalances and changes in the center of pressure of the feet.17,18 Research suggests that different mandibular positions lead to variations in body posture, contributing to changes in the pressure center of the feet and consequently affecting body balance.17-19
No optimal program and dose for the treatment of TMD have been established. Although studies suggest that edentulism may increase the risk of TMD, there are no definitive recommendations in this regard. Patients with edentulism have been reported to exhibit more symptoms compared to fully dentate patients, but the impact of this on treatment remains uncertain. Further controlled trials on TMD treatment and a better understanding of the relationship between edentulism, posture, and TMD are needed.
The objectives of the present study were to determine the effect of postural exercises in patients with myofascial TMD; and to determine the differences between the partially edentulous group (PEG) and the dentate group (DG) in terms of static body balance, mandibular movement, pain and posture at the end of the 6-week treatment. It was hypothesized that, after 6 weeks, there would be differences in the effectiveness of physiotherapy between PEG and DG patients with temporomandibular disorder.
Materials and Methods
Study Design
This is a quasi-experimental controlled study that does not include randomization. Patients with myofascial TMD who met the inclusion criteria were divided into 2 groups based on the presence of loss of contact between the 2 posterior teeth: the dentate group and the partially edentulous group.
Participants
Participants were selected from patients who applied to the Ege University Prosthodontic Clinic between January and August 2022 and were diagnosed with myofascial TMD by a specialist dentist. Inclusion criteria were the following: people between 18 and 70 years; TMJ that lasts at least 3 months (considered chronic pain according to the International Association for the Study of Pain); complaints of headache and neck pain; not having used intraoral appliances; able to attend the treatment protocol regularly; and able to communicate verbally and willing to and diagnosed with myofascial TMD according to the Diagnostic Criteria for TMD.
Potential participants were excluded if they met any of the following criteria: diagnosis of fibromyalgia, rheumatic or neurological problems; history of neck or jaw fractures; previous orofacial treatment (such as orthodontics or physical therapy within the last 12 months); positive COVID-19 test; history of sports injury, trauma, whiplash, degenerative changes, TMJ disc displacement, symptoms of osteoarthritis, postoperative conditions involving the cervical or temporomandibular region, burns involving the cervical or temporomandibular region, use of analgesics or muscle relaxants within 8 hours prior to physical therapy, hypermobility of cervical movements, acute infections, any systemic disorder, or osteoporosis.
The Dokuz Eylül University Non-Interventional Clinical Research Ethics Committee approved the study on June 29, 2022, with protocol number GOA-7337 and decision number 2022/22-02. All participants gave their informed consent in writing.
Objectives
This study aims to assess the impact of posterior edentulism on the effectiveness of a physiotherapy program for patients with TMD. We hypothesize that there is a significant difference in the effectiveness of physiotherapy in patients with TMD with posterior edentulism and fully dentate.
Outcomes
All measurements were performed at baseline and after 6 weeks by the same physical therapist with 3 years of clinical experience in musculoskeletal disorders. The primary outcome measure was balance, while the secondary outcome measures included pain intensity, mandibular movements, and posture, as described below.
Balance
The Tetrax® Interactive Balance System (Sunlight Medical Ltd., Ramat Gan, Israel) performed a balanced assessment. This system consists of 4 platforms measuring vertical pressure fluctuations in the sole of the foot. 17 The balance index measured by Tetrax represents the amount of postural sway as a mathematical outcome. Tetrax® Fall Index (TETRAX FI) provides a numerical expression of the patient’s clinically unobservable postural abnormalities, postural controls, and compensations as seen in the Tetrax® parameters. Previous studies have shown high test-retest reliability of the Tetrax® Interactive Balance Scale. 20
Participants stood barefoot on the designated surface to perform the assessment and remained still for 32 seconds. They were evaluated in 8 different positions, including with their eyes open and closed, on soft and hard surfaces, and in various head positions.
Pain Intensity
Pain intensity was assessed using the Numeric Pain Rating Scale (NPRS). The severity of pain during activity and at rest in the TMJ, neck, and shoulder regions was assessed separately for the right and left sides. Based on a verbal rating system ranging from 0 (no pain) to 10 (worst pain), the NPRS had a reliability of 0.76 in patients with neck pain. 21
Mandibular Movements
The assessment of mandibular movement involved measuring the maximum mouth opening, protrusion, and fitting and left lateral deviations using a millimeter ruler and recording the values obtained in millimeters. A millimeter ruler is a reliable method to measure lower jaw movements. 22 To determine the maximum mouth opening (MMO), the patient was asked to smile with the teeth touching each other. The position of the upper incisors concerning the lower incisors was recorded, forming the value. The patient was then asked to open his mouth to the maximum, and the distance between the upper and lower front incisors was measured with a ruler (b-value). The 2 values (a,b) were summed and recorded as the maximum mouth opening. The distance between the upper and lower front incisors was recorded during the anterior movement of the mandible to measure the movement of the protrusion. Lateral movements of the jaw were calculated as the distance from the upper midline to the lower midline of the teeth.
Posture
The static posture of the patients was assessed using the New York Posture Rating Chart (NYPRC). This rating system divides the body into 13 sections and observes and scores potential postural changes. 23 The NYPRC has been shown to have a moderate internal correlation coefficient. 24 The patients were assessed barefoot, on a flat surface, facing a wall, and scored according to the observed postural changes. Each subsection scored 5 points for correct posture, 3 points for moderately impaired posture, and 1 for severely impaired posture. On a scale ranging from a minimum of 13 to a maximum of 65 points, a total score of 45 is considered “very good,” 40 to 44 as “good,” 30 to 39 as “moderate,” 20 to 29 as “poor,” and 19 as “bad.”
Intervention
All participants were subjected to a 6-week physiotherapy program of 12 sessions twice weekly with a minimum 48-hour break between sessions. Treatment was carried out individually at Dokuz Eylul University, Faculty of Physical Therapy and Rehabilitation. All participants received a single intervention tailored to clinical requirements and individual needs. This intervention included manual non-manipulative techniques, postural exercises, deep neck flexor stabilization exercises facilitated by biofeedback, and Kinesio taping (Figure 1). Participants were provided with written and visual exercise instructions via the WhatsApp mobile application for home practice to ensure the continuity of exercises on non-session days.

Physiotherapy interventions. (A, B) Examples of posture exercises. (C) Kinesio taping for upper trapezius and sternocleidomastoideus. (D) Suboccipital inhibition technique.
Manual Therapy
All participants received cervical traction, myofascial release, massage, suboccipital inhibition, and trigger point ischemic compression. Cervical traction was maintained for 40 to 60 seconds and administered twice per session. The suboccipital inhibition technique involved placing the fingertips along the occiput and applying cranial pressure with light traction for 3 minutes. These interventions were applied twice a week in addition to postural exercises. The total duration of the manual therapy techniques was approximately 30 minutes.
Kinesio Taping
The I-shaped Kinesio tape was applied once a week to the sternocleidomastoid (SCM) and upper trapezius muscles at 10% tension in the stretched position of the muscle. For upper trapezius Kinesio taping, patients were asked to try to touch their ear to the opposite shoulder, then tilt their head slightly forward, and the tape would adhere to the muscle. For SCM, patients were asked to try to touch their ears to the opposite shoulder and then turn their heads to the same side before applying the tape. Participants were instructed to keep the tapes on for 3 days unless they caused sensitivity. Kinesio taping was stopped for participants showing skin sensitivity.
Postural Exercises
All patients received WTYL (Prone WTYL Shoulder Movement Pattern in Scapular Stabilizer Exercise) exercise twice a week with 10 repetitions to maintain and activate coordination of the scapular region. Scapular adduction and shoulder girdle exercises were performed twice a week for 3 sets of 10 to 15 repetitions using resistance bands. The resistance level of the bands was set at a perceived difficulty of 5 on the modified Borg scale. Patients received tactile signals and feedback during exercises to avoid straining their neck muscles and to maintain the correct positioning. They were also encouraged to monitor their posture in a mirror while exercising. Patients were instructed in exercises targeting the upper trapezius, SCM, posterior scalene, latissimus dorsi, and pectoral muscles. Initially, each movement was performed for 20 seconds in 3 repetitions, but at the end of the sixth session, the duration was increased to 30 seconds with 5 repetitions. The patients were advised to perform stretching exercises daily.
Craniocervical Flexor Stabilization Exercise
Deep neck flexor endurance training was performed twice a week in a supine hook-lying position using the Chattanooga Pressure Feedback Stabilizer. A pressure sensor was placed in the cervical cavity and adjusted according to the patient’s endurance level. During the assessment, the highest pressure level at which the patient could perform 10 repetitions was considered their endurance threshold, and the exercise started at a slightly higher pressure level. The patient was instructed to bring his head into cervical flexion and maintain this position for 10 seconds, as in the assessment. The exercises were performed in sets of 10 repetitions for 3 sets. Progression to the next level was determined after completion of the training without SCM contraction, without compromising neck posture, and without falling below the desired pressure level.
Data Processing and Statistical Analysis
The G* Power software (version 3.1.9.7) was utilized to calculate the total sample size. The sample size was determined based on a .05 error margin of error (α), 90% power (β), and an effect size (Cohen’s d) of 1.02 derived from a similar study, resulting in 13 in each group and a total of 26 participants. The confidence interval was set at 95%. All data were recorded and analyzed using SPSS (Statistical Package for Social Sciences) for the Windows 22 program. Initially, the assumptions were assessed to decide which tests (parametric/nonparametric) to use. The Shapiro-Wilk test, kurtosis, and skewness values, which are other assumptions of normal distribution, and histogram graphs were used to decide the normality of the distribution. The independent samples t-test and the Mann-Whitney U test were used to compare 2 independent groups. Paired sample t-test and Wilcoxon test were used to analyze the difference between 2 related numerical variables. Fisher’s exact test was used for the relationship between categorical independent variables. The significance level for interpreting the values obtained was determined to be .05.
Results
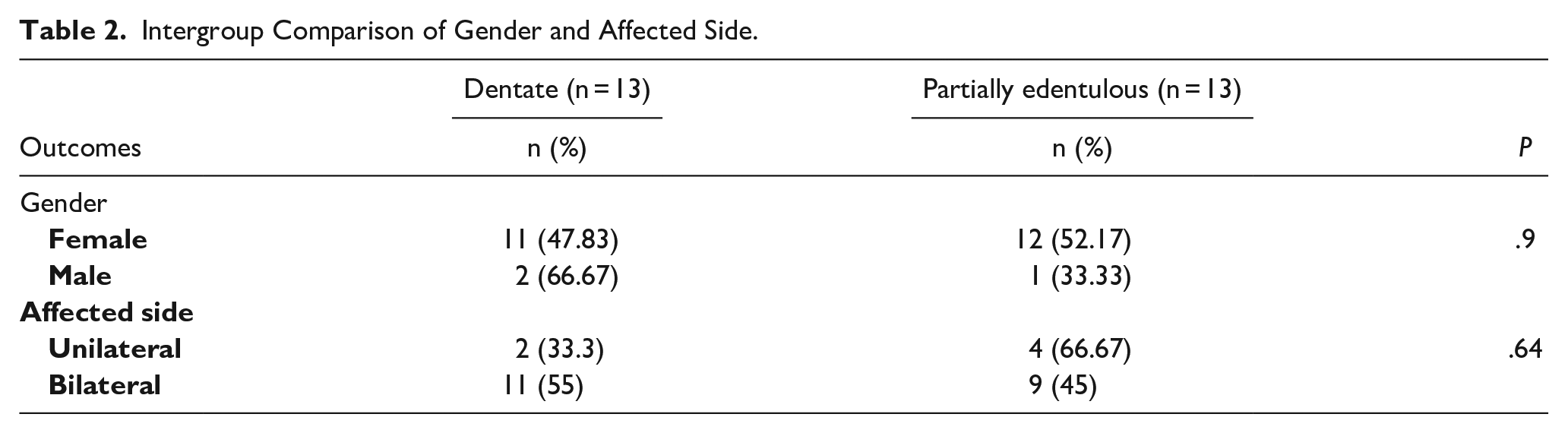
In all, 37 patients with myofascial TMD were evaluated, and 29 were included in the study. Three participants (2 from DG and 1 from PEG) dropped out for personal reasons. In total, 26 participants were included in the analysis. Their demographic and diagnostic characteristics are shown in Tables 1 and 2. No group differences were identified at baseline in any variables (P > .05).
Baseline Demographic and Diagnostic Characteristics of Each Group.
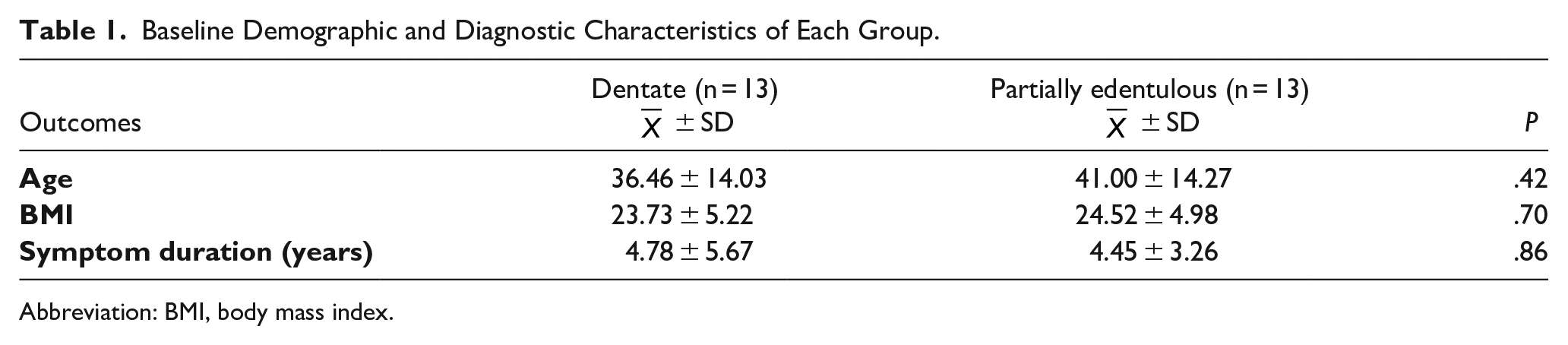
Abbreviation: BMI, body mass index.
Intergroup Comparison of Gender and Affected Side.
Balance
The pretreatment TETRAX FI values show a statistically significant difference between the groups (P = .01; Table 3). While there is no statistically significant difference between the pretreatment and post-treatment TETRAX FI values in DG (P = .41), there is a statistically significant difference in PEG (P = .02). The difference in the measurement values of TETRAX FI between the groups is statistically significant (P = .02; Table 4).
Comparison of Initial Values of Dentate Group and Partially Edentulous Group.
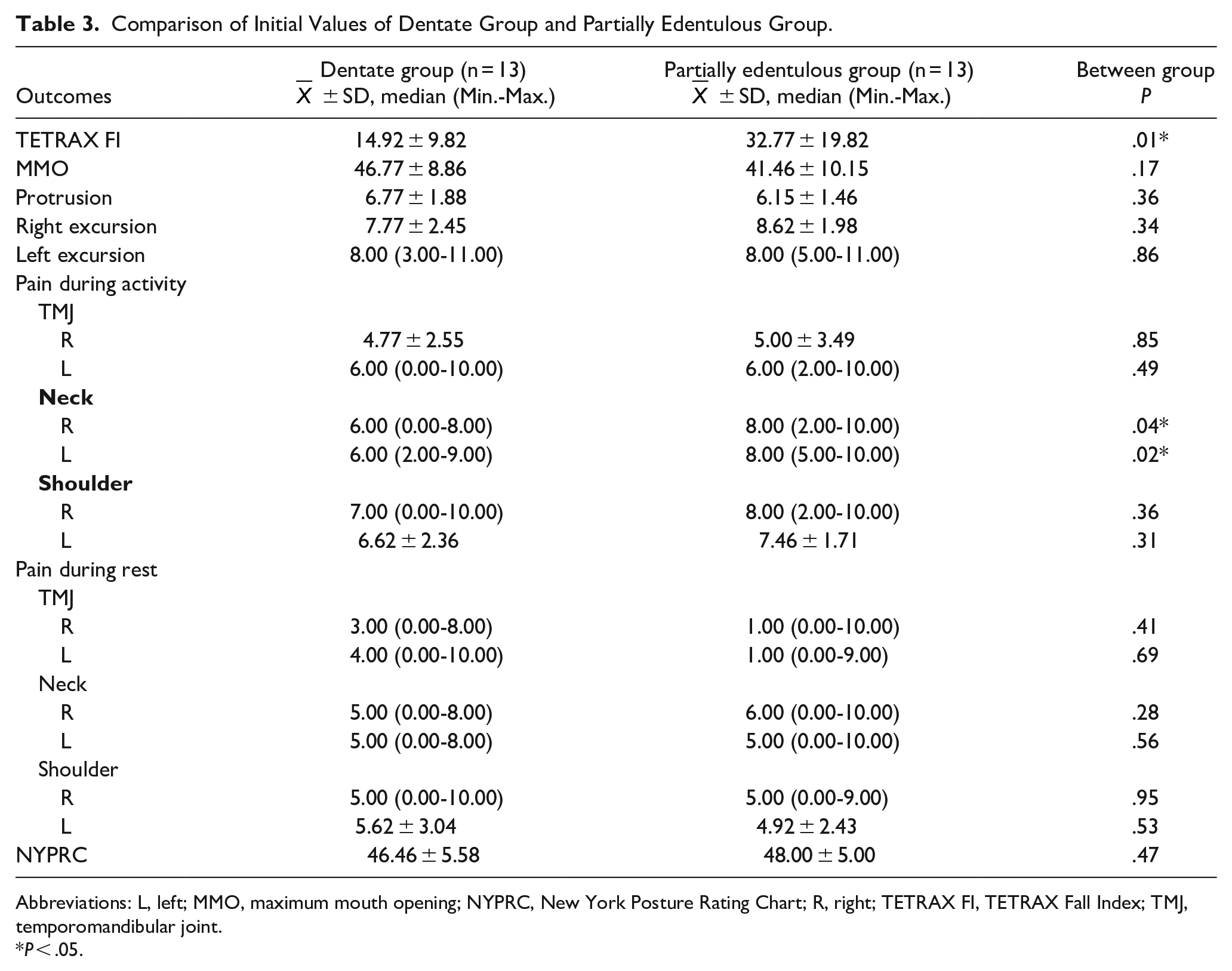
Abbreviations: L, left; MMO, maximum mouth opening; NYPRC, New York Posture Rating Chart; R, right; TETRAX FI, TETRAX Fall Index; TMJ, temporomandibular joint.
P < .05.
Baseline and Follow-Up Results for a Mandibular Range of Motion, Balance, and Posture of Each Group.
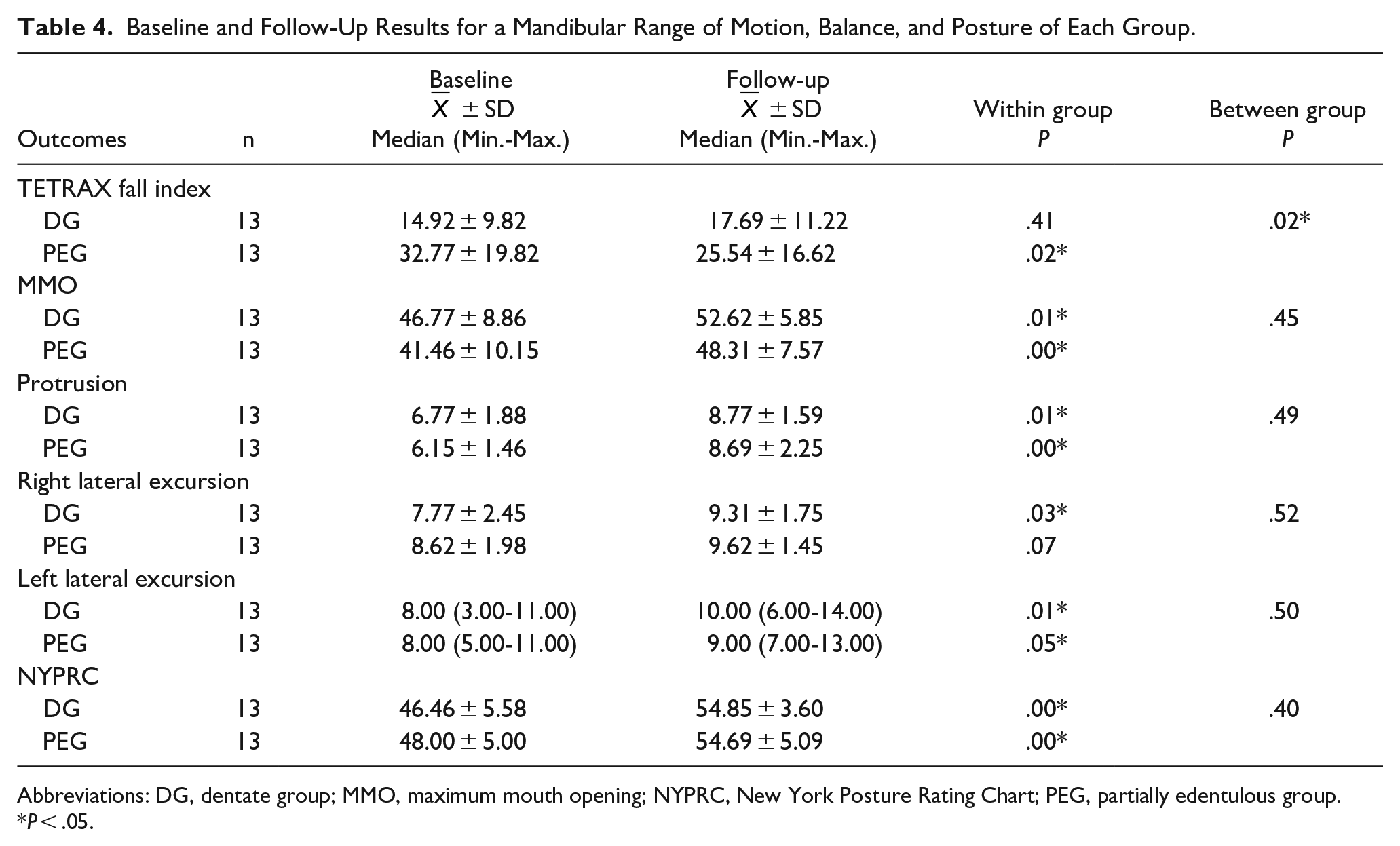
Abbreviations: DG, dentate group; MMO, maximum mouth opening; NYPRC, New York Posture Rating Chart; PEG, partially edentulous group.
P < .05.
Pain Intensity
The pain scores before treatment showed statistically significant differences between the groups for neck pain during activity (P < .05; Table 3). There were statistically significant differences between pre-and post-treatment scores in all regions in both groups after treatment (P < .05; Table 5).
Each Group’s Numeric Pain Rating Scale Measured Baseline and Follow-Up Results for Pain.
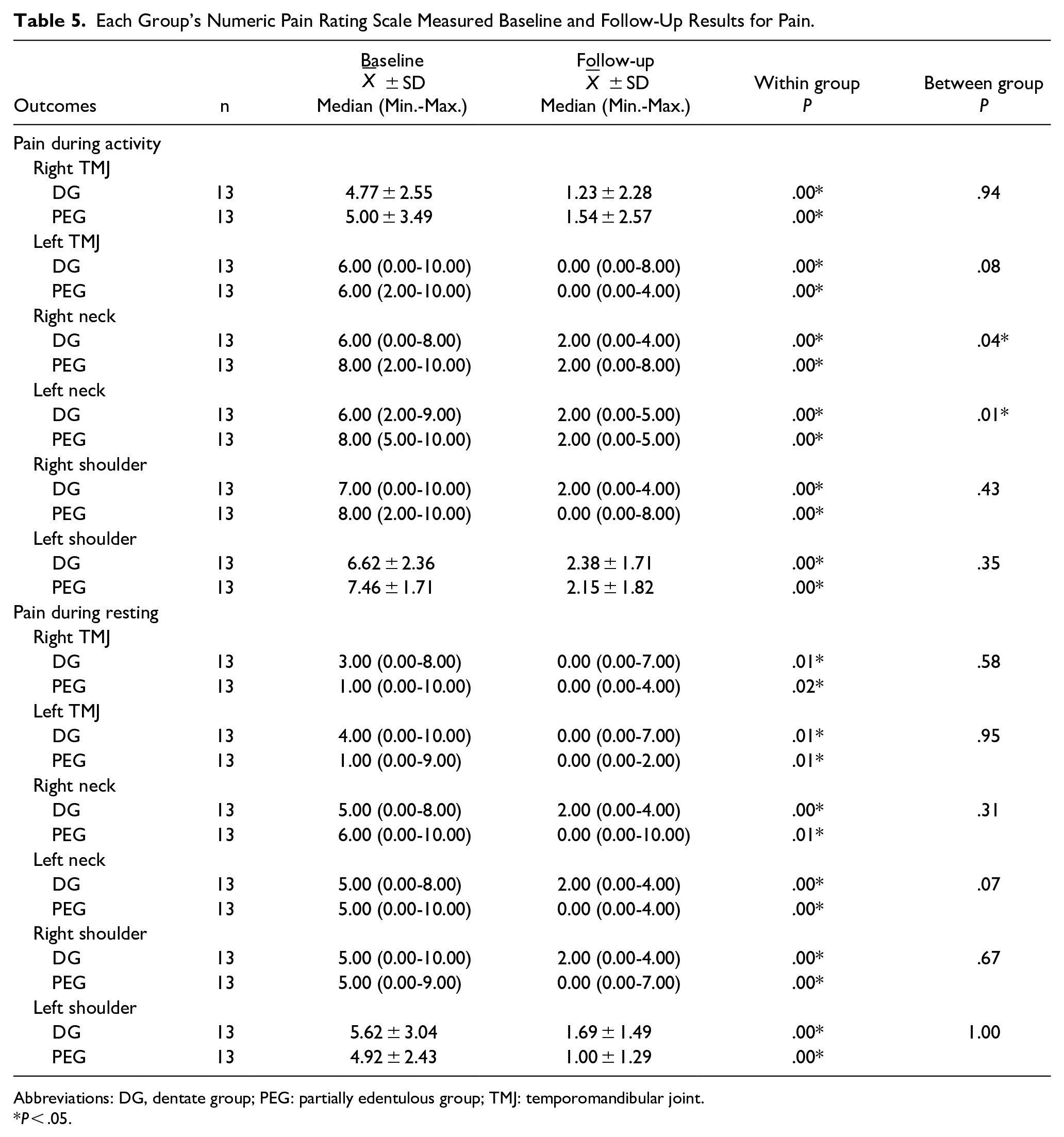
Abbreviations: DG, dentate group; PEG: partially edentulous group; TMJ: temporomandibular joint.
P < .05.
Mandibular Movements
In both groups, statistically significant increases were found in the post-treatment measurements of MMO, protrusion, and left lateral excursion compared to the pretreatment values (P < .05). After treatment, a statistically significant difference was observed in the right lateral excursion in DG (P = .03), while no significant differences were observed in PEG (P = .07). There were no statistically significant differences in the comparison between the groups (P > .05; Table 4).
Posture
There were statistically significant improvements in New York Posture Rating Chart (NYPRC) scores in both groups after treatment (P = .00). No significant differences were found in the comparison between the groups (P = .040; Table 4).
Discussion
The present study aimed to compare the effect of postural exercises on pain, mandibular movements, posture, and balance parameters in patients with Partially Edentulous Group (PEG) and Dental Group (DT) diagnosed with myofascial TMD.
The study sample consisted of 88.5% (n: 23) female patients and 11.5% (n: 3) male patients with a mean age of 38.7 years. In the literature, the prevalence of TMD has been reported to be twice as high in women as in men and peaks between the ages of 20 and 40 years. 25 In a similar study conducted by Manfredini et al, 26 it was shown that the number of female patients was 5 times higher than the number of male patients. Consequently, the sample in our study is compatible with the literature. There were no statistical differences between the groups in terms of age, body mass index, duration of symptoms, gender, and affected side, indicating that the groups were homogeneous.
Studies have been conducted in the literature to determine the relationship between posterior edentulism and MMO. 27 In a study published in 2010, it was reported that the loss of third molars and MMO showed a significant negative correlation and that missing posterior teeth can accelerate the development of degenerative joint disease and, consequently, cause a decrease in mouth opening. 28 However, a systematic review by Leal et al 29 shows that there is no scientific evidence to confirm an association between a loss of one or more teeth and the presence of signs and symptoms of TMD such as joint noise, TMJ pain, and restricted mouth opening. In our study, no significant differences were found between the groups in mandibular movements prior to treatment. As there are not many studies comparing the 2 groups in terms of both MMO and other jaw movements, new studies are needed.
In a study that included cervical mobilization and deep neck flexor muscle endurance training as a treatment program in patients with TMD, a significant increase in the value of MMO was reported after treatment. 30 Sahin et al 31 also reported that the MMO value increased after a treatment program consisting of exercise and ischemic compression in patients with TMD. In our study, significant improvements were observed in both groups according to measurements of MMO, protrusion, and left lateral excursion after treatment. The right lateral excursion showed a significant increase only in DG. This may be because we did not divide the patients into different groups such as right or left according to the affected side in the analysis. It is recommended that future studies take this issue into account and that patients be classified according to the temporomandibular joints of the affected side for analysis. Both groups did not appear to be superior to each other in terms of increased mandibular movements after treatment.
In a 2021 study conducted on people with neck and lower back pain, it was mentioned that posterior edentulism would increase the prevalence of neck pain and TMD. 32 Parallel to these findings, our pretreatment evaluations indicated that patients with TMD with posterior edentulism experienced more severe neck pain during activity. Fiorelli et al 33 reported that 6 weeks of global postural exercises reduced the intensity of pain in patients with TMD. In a similar study comparing global postural reeducation and static stretching, it was observed that both postural interventions were found to reduce TMD-induced pain. 34 In our study, we observed statistically significant reductions in pain intensity in both groups in all measured areas. When the differences before and after treatment were compared, we observed that PEG had a greater improvement in the intensity of neck pain during activity compared to DG. We believe that the reason for this difference is that the occlusion is worse in the PEG than in the DG, and an additional improvement in pain intensity is observed due to the good effect of improved head posture on occlusion as a result of postural exercises. This conclusion may explain the pain in the rest of the lower left neck after treatment in the PEG group compared to the DG group.
Studies have highlighted the potential role of dental occlusion and trigeminal afferents in providing postural control. 17 In particular, it has been argued that especially head posture is impaired and forward tilt of the head increases in individuals with TMD.16,17 Marchena-Rodriguez et al 35 showed that different dental malocclusions seen in children lead to changes in foot posture. There are not many studies on the specific effect of posterior edentulism on posture. In a 2020 study, it was reported that the angle of inclination of the articular eminence decreased in people with a single missing tooth, and tooth loss may reduce the craniocervical angle and cause the occlusal plane to deviate more from the C1-C2 intersection. 36 However, not all studies in the literature support the relationship between the stomatognathic system and posture.37-39 Perinetti 40 stated that there was no detectable relationship between occlusion and body posture. Even if studies are significant, they have a low level of evidence, and more research is needed. In our study, the pretreatment values of both groups were similar. In this sense, our study shows that posterior edentulism does not significantly affect body posture. When the differences between the 2 groups were compared at the post-treatment period, they were not found. However, both groups showed significant improvements in posture due to treatment.
A change in mandibular position, which can lead to changes in proprioceptive and periodontal afferents, can affect foot center pressure, foot position, and gait stability.19,41-43 Asymmetric mandibular position means more symmetric contraction of the SCM, which reduces body sway. 44 There is also a positive correlation between masticatory efficiency and postural balance.45,46 Therefore, tooth loss is a risk factor for postural imbalance. 47 A study carried out in geriatric individuals in Japan showed that the areas of contact with the occlus and the forces of the occlus were greater in the group with more teeth and the postural stability increased as the number of teeth and the areas of contact with the occlus increased. 48 In another study conducted on elderly individuals, standing on 1 leg and performing the functional reaching test showed worse results in the missing teeth group compared to the full dentate group. 49 In support of these articles, the pretreatment PEG balance results were significantly worse than DG in our study. The distortion of the bite plane and the change in bite force associated with tooth loss are compensated by the postural muscles. The better the head posture, the better the jaw closure. We believe that improving posture and, therefore, occlusion after treatment led to an improvement in PEG balance.
Comparison of physiotherapy efficacy between patients with posterior edentulous and fully dentate myofascial TMD, an area that has never been investigated, and the fact that it is one of the few studies to show that TMD symptoms can be significantly reduced by postural exercises alone are the main strengths of our study.
The study’s limitations include the lower number of male patients participating due to the higher prevalence of TMD in women, the reduced effectiveness of exercise due to some patients testing positive for COVID-19 under pandemic conditions, and the subsequent exclusion from the study. In addition, tracking home-based exercises proved challenging.
Postural exercises should involve more areas of the body, beyond just the upper body. Comparative studies on the effectiveness of treatment between edentulous groups are lacking, highlighting the need for research comparing their responses to physical therapy. We also recommend multidisciplinary studies that combine dental treatment and physical therapy between these 2 groups.
Conclusion
This study showed that postural exercises, manual therapy, and Kinesio taping could provide significant improvement in patients with myofascial TMD. The presence of posterior edentulism affected the effectiveness of physiotherapy on pain and balance parameters. We recommend that physiotherapists and dentists work together with a multidisciplinary approach and that patients start treatment simultaneously with the physiotherapy program and dental treatment.
Footnotes
Author Contributions
All authors were involved in developing, designing, and critically reviewing the study’s manuscript. SNA worked on the study design and data interpretation. RT contributed to the design and planning of the study, data collection, analysis, and interpretation of results. GCA played a role in study design, data collection, and interpretation.
Consent to Participate
All subjects provided their informed written consent to include them before participating in the study.
Consent for Publication
We confirm that informed consent for publication has been obtained from all participants involved in this study. Participants were fully informed about the purpose of the study and the potential publication of their data in an academic journal. The authors have documented and retained informed consent in a manner that is consistent with institutional guidelines and regulations.
Data Availability Statement
All data presented in this article are included in the manuscripts or tables/figures. Further inquiries can be directed to the corresponding author.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Considerations
This study was conducted following the Declaration of Helsinki of 1975 (as revised in 2013), and the research was approved by the Dokuz Eylül University Faculty of Medicine Non-Interventional Clinical Research Ethics Committee with protocol number GOA-7337 and decision number 2022/22-02. The study was conducted under the Declaration of Helsinki.