
Abstract
Histiocytic necrotizing lymphadenitis (HNL), also known as Kikuchi disease, is a relatively rare sub-acute necrotic localized lymphadenitis. This benign, self-limiting condition is characterized by fever, painful lymphadenopathy, skin rash, and other systemic symptoms. Due to its nonspecific presentation, unclear etiology, and pathogenesis, HNL has a low incidence rate in clinical practice. Insufficient awareness among clinicians and pathologists can easily lead to misdiagnosis. This article reported a 27-year-old female patient who was admitted to the hospital with fever, neck pain, and enlarged lymph nodes in the neck. There were no special medical or personal histories, and postoperative pathology confirmed tissue necrotizing lymphadenitis. After treatment with steroids and symptomatic therapy, she recovered and was discharged from the hospital. Follow-up to date has shown no recurrence.
Keywords
Introduction
Histiocytic necrotizing lymphadenitis (HNL), also known as Kikuchi disease Fujimoto disease or Kikuchi disease, is a rare benign self-limiting disease characterized by cervical lymph node enlargement, fever, and leukopenia, presenting as the acute subacute onset. Due to the unclear etiology and pathogenesis, as well as the lack of specificity in clinical manifestations, there is currently no unified diagnostic standard. Diagnosis mainly relies on histopathological examination and needs to be differentiated from lymphadenitis, lymph node tuberculosis, malignant lymphoma, metastatic malignant tumors, etc. Due to the lack of specificity of its clinical manifestations, the clinical incidence rate is relatively low, and clinicians and pathologists lack understanding of it, which is easy to leads to misdiagnosis. This article shares a case of a patient misdiagnosed with a cervical abscess and a review of relevant literature.
Case Report
A 27-year-old female patient was admitted to the hospital with a 1-week history of “left neck pain accompanied by intermittent fever.” The patient developed left neck pain without apparent cause 1 week prior to admission. The initial symptoms were mild but progressively intensified, accompanied by chills and pyrexia, with body temperature oscillating between 38.5°C and 39°C. A diagnosis of upper respiratory infection was made at a local medical facility, where dexamethasone sodium phosphate and piperacillin sodium tazobactam were administered for symptomatic relief. This intervention resulted in a reduction of body temperature; however, the cervical discomfort persisted. Two days prior to hospital admission, the patient experienced a significant exacerbation of neck pain, accompanied by left cervical tumefaction and systemic manifestations including recurrent rigors, pyrexia, cephalalgia, and fatigue. Notably, the patient did not report odynophagia, cough, or expectoration. Due to unsatisfactory treatment effects at the local hospital, the patient sought further diagnosis and treatment at our hospital. Outpatient neck computed tomography (CT) suggested a left deep cervical space infection, and the patient was admitted with a diagnosis of “left neck abscess.” Upon admission, the physical examination revealed the following: a body temperature of 36.5°C, respiratory rate of 20 breaths/min, and blood pressure of 130/69 mmHg. The patient was alert and oriented but exhibited an acute facial expression. No icterus or cutaneous eruptions were observed on the mucous membranes. Palpation did not reveal superficial lymphadenopathy or hepatosplenomegaly. Cardiopulmonary and neurological examinations were unremarkable. Cervical mobility was restricted, with the head inclined toward the left. The upper-middle segment of the left neck displayed significant tumefaction and protrusion compared to the contralateral side. The surface skin temperature was normal, and palpation revealed a hard, tender mass without fluctuation. Oropharyngeal and laryngeal examinations did not reveal any notable abnormalities. Ancillary examinations revealed normal blood cell counts, with a neutrophil percentage of 71.50%, an eosinophil percentage of 0.1%, an eosinophil absolute value of 0.10 × 109/L, and a hematocrit of 36.50%. The biochemical series and urine routine were normal. A neck CT examination suggested a left deep cervical space infection. The initial diagnosis was a left neck abscess, and the patient was treated with cefmetazole sodium and ornidazole for anti-inflammatory therapy. However, the patient continued to experience recurrent chills and fever. A subsequent cervical magnetic resonance imaging (MRI) examination revealed abnormal signal shadows in the left cervical soft tissue space. These shadows exhibited slightly elevated signal intensity on T1-weighted images, markedly elevated signal intensity on T2-weighted images, and high signal intensity on diffusion-weighted imaging, suggesting abscess formation (Figure 1). On the second day post-admission, an exploratory operation of the left neck was performed under general anesthesia. No obvious abscess was found during the operation, but an enlarged lymph node was discovered on the deep surface of the sternocleidomastoid muscle. Postoperatively, neck pain was significantly relieved, but the patient experienced chills and fever again in the afternoon of the first postoperative day, with temperatures fluctuating between 38.5°C and 40°C. Pathological findings revealed multifocal necrosis and extensive neutrophilic infiltration in lymphoid tissue, consistent with necrotizing lymphadenitis (Figure 2). No bacteria were found in the blood culture. The patient was transferred to a superior hospital for further treatment on the second postoperative day. During follow-up, bilateral popliteal lymph node enlargement occurred, resulting in limited squatting. After glucocorticoid and other symptomatic treatments, the patient was cured and discharged from the hospital in the third week of the disease course.
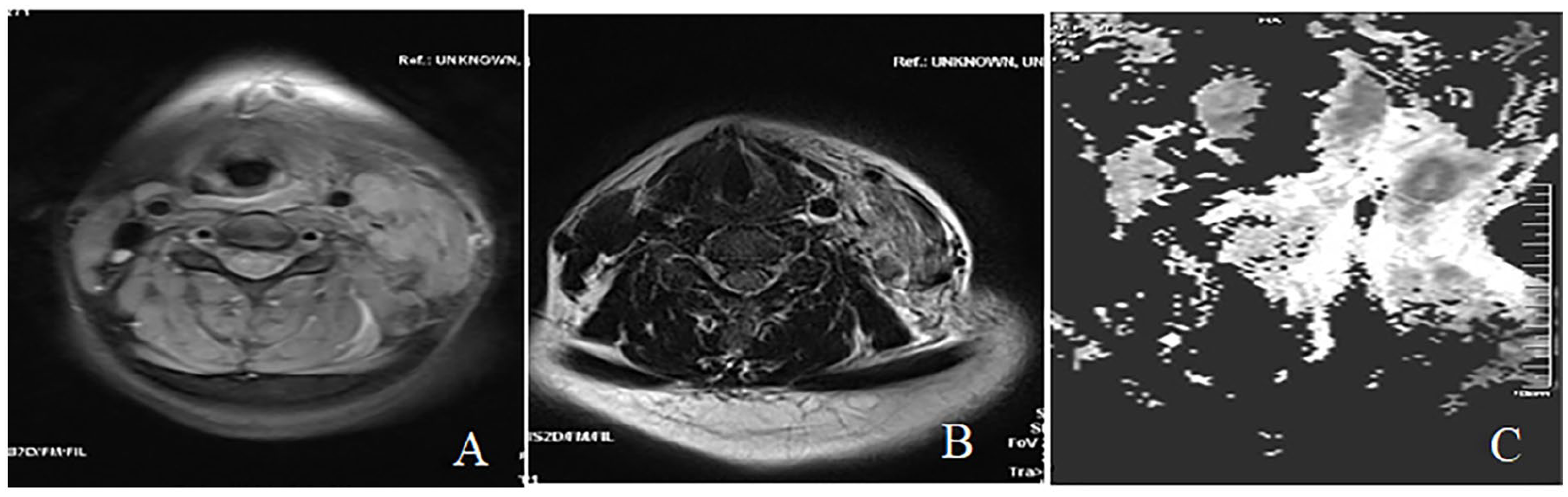
Preoperative MRI examination with lesion (A) shows significantly high signal intensity and uneven internal signal, lesion (B) shows slightly high signal intensity, and lesion (C) shows high signal shadow with unclear boundaries.
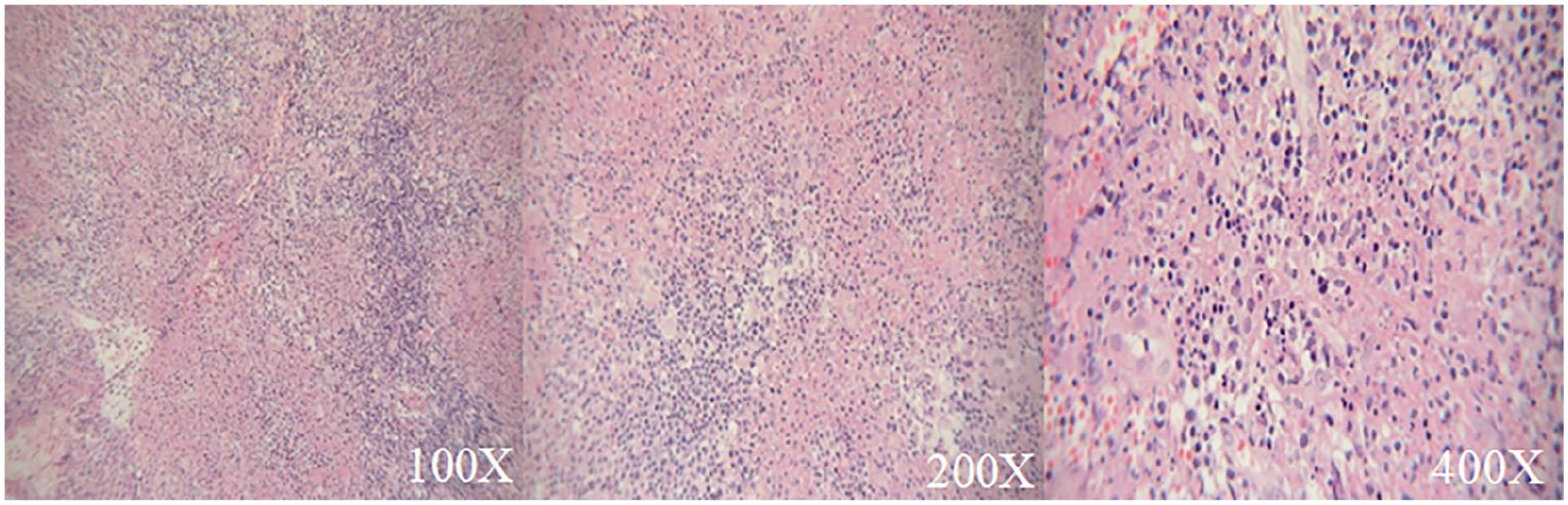
The postoperative pathological results show a large amount of neutrophil infiltration in the lesions of SP×100, SP×200, and SP×400, respectively.
Discussion
HNL, also referred to as Kikuchi-Fujimoto disease or Kikuchi disease, is an uncommon, benign, self-limiting disorder characterized by cervical lymphadenopathy, pyrexia, and leukopenia, with an acute or sub-acute onset.1-3 Epidemiologically, HNL demonstrates a higher incidence among Asian populations, particularly in females under 40 years of age. 4 The etiology and pathogenesis remain elusive; however, some researchers 5 postulate that it may be an autoimmune disorder or an exaggerated immune response to an underlying infection. Viral infections are frequently implicated, with the Epstein-Barr virus being the most commonly associated pathogen. 6 Other viruses implicated include human herpesvirus 6 (HHV-6) 7 and HHV-8, 8 although subsequent studies have failed to detect the presence of these specific infectious agents through serological or polymerase chain reaction tests, rendering the relationship between these viruses and HNL controversial.
The clinical manifestations of HNL, in addition to the typical cervical lymphadenopathy and pyrexia, include fatigue, weight loss, cutaneous eruptions, arthralgia, myalgia, and hepatosplenomegaly. Lymph node involvement is often unilateral, with cervical lymph nodes being the most frequently affected site, followed by supraclavicular, axillary, thoracic, abdominal, pelvic, and popliteal lymph nodes. Affected lymph nodes typically present as enlarged, painful, or indurated. 9 Approximately 40% of patients may develop erythema, papules, or plaques on the face, trunk, or upper extremities.
At present, there are no universally accepted diagnostic criteria for HNL, either domestically or internationally. 10 Imaging studies play a crucial role in assessing the extent and nature of lymph node lesions in HNL patients. Color Doppler ultrasonography typically reveals clustered or mass-like lesions of the affected lymph nodes, occasionally accompanied by perinodal adipose tissue edema. 11 CT scans demonstrate uniformly enhanced or hypodense areas within the affected lymph nodes. 12 MRI exhibits isointense or hypointense central necrotic areas on T1-weighted images, with signals lower than non-necrotic areas on T2-weighted images. 12 Laboratory investigations may reveal elevated C-reactive protein (CRP), abnormal hepatic transaminases, leukopenia (particularly neutropenia), lymphocytosis, anemia and/or thrombocytopenia, and positive antinuclear antibodies.
In the present case, the patient presented with cervical pain and pyrexia; however, preoperative color Doppler ultrasonography was not performed, and cervical CT, MRI, and laboratory examinations were not entirely consistent with the typical findings. Definitive diagnosis of HNL primarily relies on lymph node biopsy and histopathological analysis. Characteristic 5 histopathological features include necrosis and/or histiocytic infiltration within lymph nodes, accompanied by reactive proliferation of surrounding tissues. Proliferative tissues are often present around the lesions, with diverse cellular morphology, including monocytes, nuclear fragments, and karyopyknosis. Immunohistochemical staining demonstrates that cells in the necrotic areas are predominantly CD4, CD8, and CD68 positive, with numerous cells containing human leukocyte antigen-1 granules. The proliferating histiocytes in HNL simultaneously express CD68 and myeloperoxidase, which is a distinguishing feature of histiocytes in HNL. Natural killer cells and B cells are less frequently observed. HNL must be differentiated from lymphadenitis, tuberculous lymphadenitis, malignant lymphoma, and metastatic malignancies.
The management of HNL typically involves symptomatic treatment with analgesics, antipyretics, and other supportive therapies. In severe cases or those with protracted courses, short-term oral glucocorticoid therapy may be employed, although there is no standardized regimen for dosage and duration of steroid administration. 5 Some researchers have reported that hydroxychloroquine can also be utilized in the treatment of this condition, offering superior long-term safety and reliability compared to glucocorticoids, and is often employed as an alternative to high-dose corticosteroids. For severe cases, intravenous immunoglobulin may be administered. 11 While HNL is generally self-limiting with a relatively favorable prognosis, there is a potential for recurrence and progression to systemic lupus erythematosus. 3 Consequently, long-term close follow-up should be established for patients with this condition.
Conclusion
This case highlights the importance of considering HNL in patients presenting with painful cervical lymphadenopathy, recurrent chills and fever, congested rashes on both lower limbs, normal or decreased white blood cell count, decreased granulocytes, elevated CRP, and ineffective antibiotic treatment. The misdiagnosis, in this case, can be attributed to several factors: insufficient understanding of HNL among clinicians and radiologists, relatively cursory admission examinations, inaccurate interpretation of imaging reports, incomplete preoperative evaluations, and failure to make timely judgments regarding the ineffectiveness of antibiotic treatment while overlooking the patient’s provided medical history (normalization of temperature following local glucocorticoid administration). This review of literature related to HNL aims to summarize the shortcomings in the diagnostic process and provide insights for colleagues in subsequent clinical work.
Footnotes
Author Contributions
All authors have contributed to the research. YZ: Investigation, data organization, initial draft writing, case follow-up. QL: Data organization, writing review, and editing. CX: Image production.
Data Availability Statement
The data that support the findings of this study are available from the corresponding author, [QL], upon reasonable request.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Written Informed Consent
The Guizhou Provincial People’s Hospital Ethics Review Committee approved our interviews. Respondents gave written consent for review and signature before starting interviews. All participants provided written informed consent prior to enrollment in the study, and they consented to the publication of the study as well as the use of their photographs or other images.