
Abstract
Keywords
Introduction
Chronic otitis media with effusion (COME) is an inflammatory condition affecting the middle ear and presenting as a nonsuppurative effusion behind a non-inflamed tympanic membrane (TM) of at least 3 months duration. 1 It is commonly seen in otologic clinics and results from dilatory Eustachian tube dysfunction (DETD). 1 Most patients with COME are treated via myringotomy or tympanostomy tube (TT) insertion.2,3 Although the latter is very successful in ventilating the middle ear in patients with DETD, premature extrusion of the TT may result in the need for tube reinsertion. 4 The cause of premature TT extrusion is unclear. However, invasive methods from the aural side often cannot address the underlying condition of the nasopharyngeal side of the eustachian tube (ET). 5 Therefore, management of the underlying pathogenesis of DETD remains a topic of research interest.
Some studies have identified the cartilaginous lumen portion of the ET as the most frequent site of dysfunction6,7; others have focused on treatment approaches, mostly eustachian tuboplasty, including laser,6,8 and microdebrider 9 eustachian tuboplasty. The reported success rates are 60% 6 and 65%, 9 respectively. Although these results are satisfactory, consecutive studies are lacking due to pain during the healing period and complications. Notably, despite the broad adoption and high efficacy of balloon eustachian tuboplasty (BET), the success rate is 47% to 90%, depending on the evaluated parameter and length of follow-up.10-12 However, the use of BET has remained limited because of its high cost and the poor medical insurance coverage in most developing countries. It has also been suggested that among patients with middle ear pathologies caused by Eustachian tube dysfunction (ETD), only those with symptoms of chronic ETD will benefit, including longer-lasting results. Lower success rates have been reported in patients with secondary middle ear pathology from their ETD.10,13 In addition, eustachian tuboplasties are more often employed to address the cartilaginous tubal lumen than to manage the ET orifice.8-12
Recent studies indicate that a thickened mucosa in the tubal orifice acts as a barrier to ET ventilation, which would not be directly addressed by balloon dilation of the cartilaginous ET. 14 Yanez et al 15 found that 87.4% of their patients with DETD had remarkable mucosal hypertrophic disease in the ET orifice or posterior cushion. In Christov et al, 14 61% of the patients had advanced mucosal disease at the tubal orifice. However, according to Gey et al, 16 82% of the patients with chronic inflammatory middle ear disease had no measurable DETD in the ET lumen. These findings have drawn attention to the management of mucosal hypertrophic disease in the ET orifice to treat DETD. Yanez et al 15 reported an improvement of the subjective symptoms of ear blockage in 92% of patients, and an improved abnormal tympanogram in 96% of those treated using the cross-hatching technique. In Lou et al, 17 72.2% of the treated patients had both a normal tympanogram and a normal TM 30 months after following ablation tuboplasty.
Radiofrequency ablation (RFA) is an evolving technology in which simultaneous ablation, cutting, hemostasis, and suction are achieved at low temperatures (40-70℃) using 1 instrument.18-20 The advantages include a shorter operation time and lower medical costs than those associated with commonly used lasers and microdebriders.14-16 Previous studies have found that the mucosal epithelium and its function may not be preserved after the use of CO2 laser ablation and microdebriders.21,22 Impaired epithelial function and mucociliary transport can cause prolonged rhinorrhea and crusting. By contrast, RFA is capable of preserving epithelial function and is associated with less postoperative pain.22,23 It also obviates the need for additional nasal packing, whereas the need for packing with microdebriders to control hemorrhage and close the submucosal dead space decreases postoperative patient comfort and prolongs hospitalization. 22 Zong et al 18 reported a success rate of 90.4% at 6 months postoperatively and 86.0% at 12 months postoperatively following RF eustachian tuboplasty. In some studies, RFA has been found to be significantly better than CO2 laser ablation and microdebriders for postoperative mucosal recovery.18,22 In addition, in RFA the plasma knife head can be bent to fit a narrow space, allowing the removal of hypertrophic tissue, which is difficult to achieve with the linear beam of a CO2 laser. 19 Nevertheless, the disadvantage of RFA is that the plasma knife head is still thick enough that it can easily injure the anterior wall, resulting in synechiae of the ET orifice. Thus, we evaluated the effect and complications of RFA eustachian tuboplasty on the treatment of intractable COME in patients with a history of multiple spontaneous TT extrusions.
Materials and Methods
Ethical Considerations
The study protocol was reviewed and approved by the Institutional Ethical Review Board of the 908th Hospital of PLA and Yu Jiang People’s Hospital (clinical trial number: 2021KY1186). All participants provided written informed consent.
Patients and Definitions
The inclusion criteria for this prospective study were as follows: adult (age >18 years) patient with unilateral intractable COME >12 months duration; symptoms of hearing loss, ear fullness, and tinnitus; negative Valsalva maneuver; type B findings in tympanometry; a history of premature TT extrusion; premature extrusion within 3 months following TT insertion; and air-bone gap (ABG) <35 dB. The exclusion criteria were head or neck surgery within the past 3 months, history of radiation therapy of the head/neck, fungal sinusitis, chronic rhinosinusitis, allergic rhinitis, suspicious laryngopharyngeal reflux, prior surgical intervention to dilate the ET, abnormal bony portion of the ET, and hypertrophic disease of the cartilage near the isthmus. Intractable COME was defined as COME with premature TT extrusion following TT insertion within 12 months of this study. All patients had previously undergone Goode T-tube treatment. All surgeries were performed by the same experienced surgeon and did not involve any trainee.
The patients underwent preoperative and postoperative high-resolution thin-slice computed tomography (HRCT) scanning and audiograms. The patient’s age, ear side, sex, duration of COME, time, number of spontaneous TT extrusions, duration of intubation, and mucosal inflammation scale (MIS) score were recorded and evaluated. Audiometric data were assessed preoperatively and 24 months postoperatively. Pure-tone averages were calculated for both air conduction (AC) and bone conduction (BC), by averaging the thresholds at 500, 1000, 2000, and 3000 Hz. In most cases, a threshold of 4000 Hz was used to interpolate the 3000 Hz threshold, in accordance with the standards of the Hearing Committee of the American Academy of Otolaryngology—Head and Neck Surgery. ABG was calculated by subtracting AC from BC thresholds. ABG closure was defined as the difference between the preoperative and postoperative ABG. The MIS score of the ET orifice was based on a 4-point scale, as described in previous studies.24,25
Surgical Procedure
All surgical procedures were performed in the operating room, not as an office procedure. The patients were placed in the supine position and administered general anesthesia for endotracheal intubation. All patients underwent simultaneous RF eustachian tuboplasty and TT insertion. The coblation system was introduced using a 0° or 30° endoscope via the ipsilateral nasal passage. Septorhinoplasty, lateral outfracture of the inferior turbinate, and partial inferior ablation turbinectomy were used to enhance exposure of the ET orifice.
RFA eustachian tuboplasty has been described in previous reports. 18 The coblation system used in this study is marketed by China Micro Medical Limited Shanghai Micro Medical Devices Co., Ltd. (Shanghai, China); the Evac 70 Plasma wand was preferred. During the entire process, the wand was set at an ablation power of 7 and a coagulation power of 3.
The hypertrophic mucosal and submucosal tissues of the ET orifice were ablated, including the leading edge of the medial cartilaginous lamina and the proximal (anterior) and posterior surface of the posterior cushion. Tissue ablation was superficial, with the cartilage serving as the deep margin throughout the procedure. RFA of the submucosal tissue was possible after the free edge of the medial cartilaginous lamina had been identified.
The extent of tissue ablation was determined by the bulkiness of the hyperplastic mucosa (Figure 1). The TT was inserted once ET orifice ablation was completed. No nasal packing was used following tuboplasty. Patients were discharged within 24 hours of surgery and advised to use intranasal steroid sprays for 2 weeks to reduce postoperative swelling of the ET orifice.
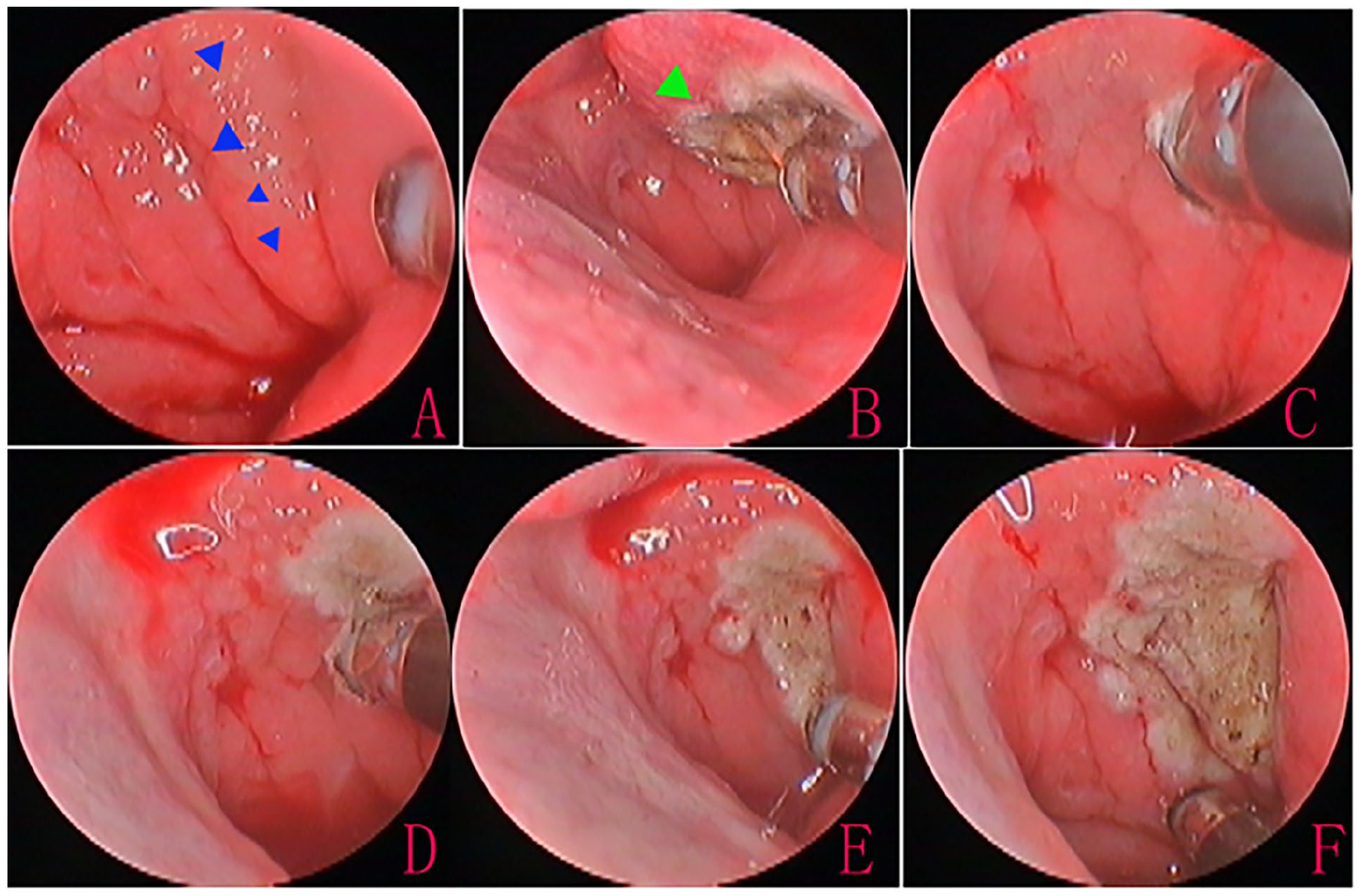
Radiofrequency ablation tuboplasty. Preoperative ET orifice (A); posterior end ablation of the inferior turbinate to fully expose the ET orifice (B); posterior wall ablation (C, D); posterior cushion ablation (E); and end of the procedure (F). The blue triangle indicates mucosal polypoid change, and the green triangle is the end of the inferior turbinate. ET, eustachian tube.
Postoperative Follow-Up and Outcome Measures
All patients were followed up postoperatively and assessed at 4 weeks and at 6, 12, and 18 months. The nasopharynx and middle ear were inspected at each follow-up. An audiometric evaluation and HRCT were performed 18 months postoperatively. Tube retention success was defined as TT retention of at least 12 months or intentional removal of the TT 6 months after surgery. The recurrence of otitis media with effusion (OME) was defined as visible OME 6 months after intentional TT removal. Successful perforation closure was defined as spontaneous closure of the perforation 6 months after intentional removal.
The outcome measures were the TT retention success rate, the perforation closure rate, hearing improvement, and complications.
Results
The study population consisted of 24 ears with COME. The 21 male and 3 female patients had a mean age of 39.2 ± 10.6 years (range: 28-52 years). The right ear was involved in 17 patients, and the left ear in 7 patients. All patients had previously undergone Goode TT treatment. Of the 24 ears, HRCT revealed a left parapharyngeal space tumor in 1 patient, who was excluded from this study. Thus, a total of 23 ears were ultimately included in the study. Preoperative computed tomography (CT) showed a soft-tissue shadow of the tympanic cavity and mastoid in all 23 ears. All surgeries were completed within 20 min after general anesthesia. The medical cost of the plasma knife was $210.2 for each patient.
Of the 23 ears, premature extrusion following TT insertion within 1 week, 4 weeks, and 3 months occurred in 8.7% (2/23), 26.1% (6/23), and 65.2% (15/23) of the patients. Prior to undergoing concurrent RF eustachian tuboplasty, 56.5% (13/23) of the patients had 1 set of TT, 34.8% (8/23) had 2 sets, and 8.7% (2/23) had 3 sets. Endoscopic inspection of the ET orifice showed remarkable mucosal hypertrophic disease or mucosa polypoid changes in the posterior cushion or posterior wall. Overall, 2 patients (8.7%) had mild thickening (Grade 2), 4 (17.4%) had moderate thickening (grade 3), 14 (60.9%) had severe thickening (Grade 4), and 3 (13.0%) had polypoid degeneration (grade 4).
The preoperative AC Pure-tone average (PTA) in the 23 ears was 47.1 ± 4.9 dB; the preoperative BC PTA was 16.8 ± 5.4 dB, and the preoperative ABG was 30.2 ± 1.7 dB. The corresponding postoperative values were 28.6 ± 3.6 dB, 15.7 ± 1.2 dB, and 13.1 ± 4.6 dB. The ABG gain was 18.3 ± 2.5 dB. Of the 23 patients, 4 had postoperative otorrhea and were administered topical ofloxacin ear drops and oral antibiotics to prevent infection, with all 4 cases successfully controlled within 1 week. None of the 4 patients had a significant preoperative history.
Of the 23 ears, the TT was retained for at least 12 months in 19 patients; intentional premature removal at postoperative 8 to 9 months was performed in 2 patients, and premature extrusion in 2 patients. Thus, the tube retention success rate was 91.3% (21/23). OME recurrence was not seen in any of the 21 ears with intentional removal at the 6-month follow-up, whereas 4 patients had persistent perforations and 17 had spontaneous closure of the perforation.
Of the 21 ears with intentional removal, postoperative endoscopic examination showed grade 1 and a positive Valsalva maneuver in 18 ears, grade 2 and a positive Valsalva maneuver in 2 ears, and grade 1 and a negative Valsalva maneuver in 1 ear. Of the 2 cases of premature extrusion, one occurred at postoperative 3 months; in that patient, a cholesterol granuloma was considered and later confirmed by pathological examination. In the other patient, a scar synechia of the ET orifice and recurrent OME were endoscopically seen at postoperative 5 months.
Of the 21 ears with intentional removal, the perforation closure rate was 81.0% (17/21). Among those 17 ears, the ET was well dilated. The postoperative CT showed good aeration of the mastoid in 14 patients and a small amount of soft-tissue shadow in 3 patients. Of the 4 ears with persistent perforation, ET orifice stenosis occurred in 3 (Figures 2 and 3) and pseudomembrane formation in one; in the latter, postoperative CT showed poor aeration of the mastoid.
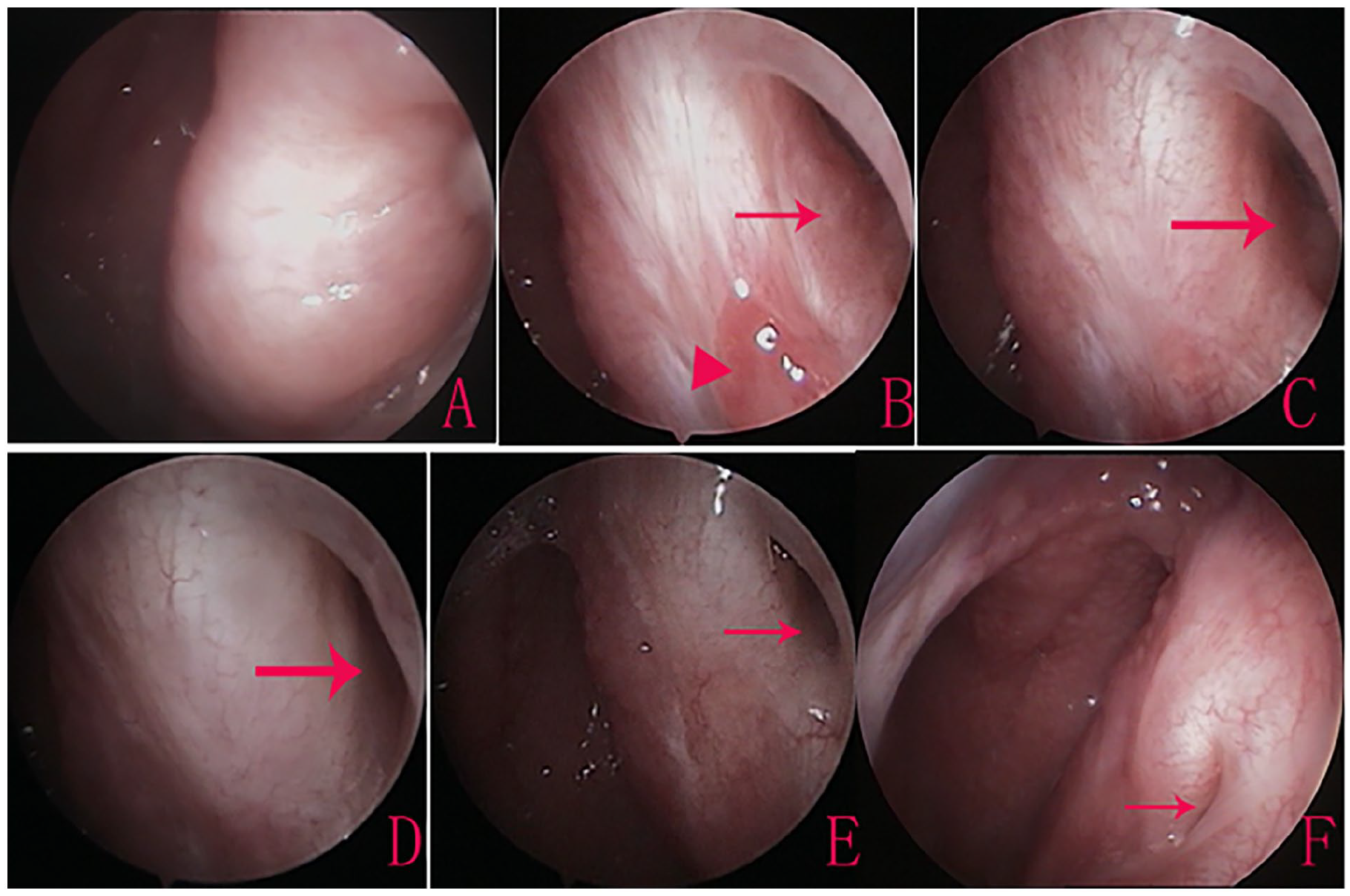
A 56-year-old patient with 3 previous spontaneous TT extrusions: ET status. Preoperative ET orifice (A), and the ET orifice 3 months (B), 6 months (C), and 12 months (D) after surgery. Stenosis of the ET orifice 18 months (E) and 40 months (F) postoperatively. Red arrows indicate the ET orifice. ET, Eustachian tube; TT, tympanostomy tube.
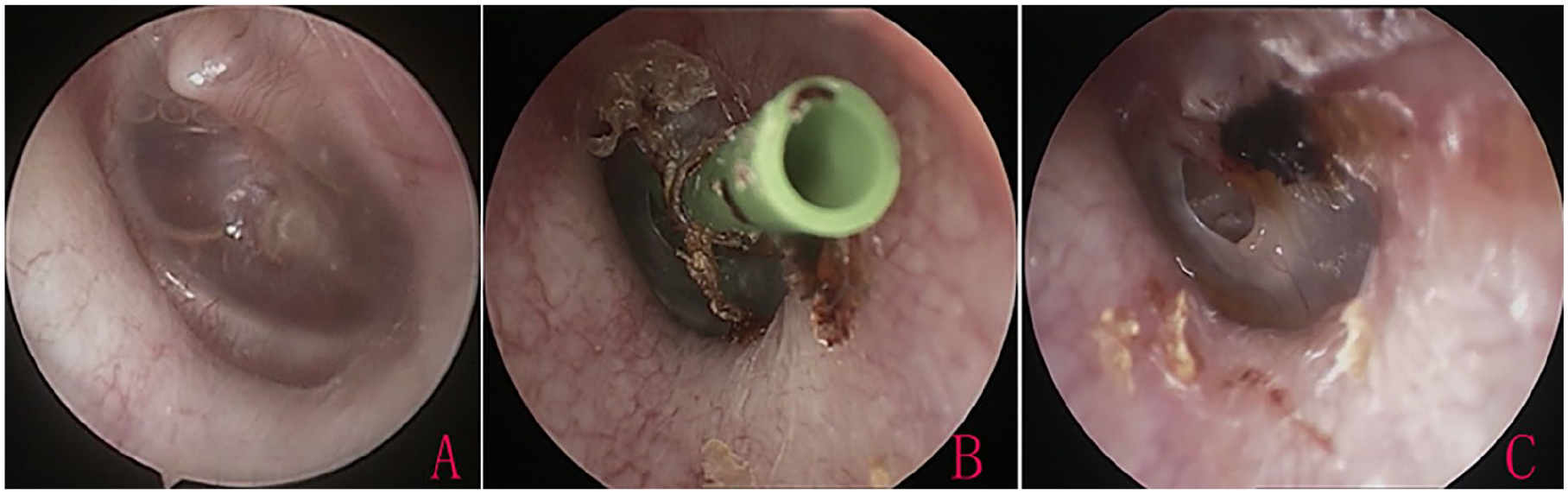
Status of the tympanic membrane and TT in the same patient as in Figure 2. Preoperative tympanic membrane (A); TT retention at postoperative 15 months and intentional removal on the same day (B); persistent perforation at 40 months postoperatively (C). TT, tympanostomy tube.
Complications
Neither RFA-related serious adverse events developed in any of the patients nor were there any cases of patulous ET. However, scar synechia of the anterior-posterior wall was seen in the ET orifice of 1 patient and was subsequently separated using Merocel packing in the ET orifice for 1 week. In addition, stenosis of the ET orifice occurred in 3 patients and pseudomembrane formation, which was not further treated, in 1.
Discussion
The retention period of TT for the treatment of COME should be at least 12 months. 4 Premature extrusion results in OME recurrence and thus the need for repeat TT insertion. 2 Takai et al 26 found that the shorter the duration of TT retention in the middle ear, the more significant the rate of increase in OME recurrence. The main cause of premature extrusion of the TT is the failure to address the etiology of DETD and therefore to improve ET function, resulting in persistent effusion or granulation tissue in the middle ear. Previous studies have demonstrated a significant association with mucosal inflammation of the ET orifice in most cases of DETD,24,25 with severe mucosal edema and polypoid change acting as a barrier to ET ventilation.14,17 Based on an ET mucosal inflammation scale, patients with grade 3 and grade 4 thickening have obviously compromised ET lumen dilation.15,17 BET of the cartilaginous aspect of the ET has recently emerged as a means to directly augment tubal dilatory function. 1 However, while clinical studies have demonstrated the higher efficacy of BET compared to continued medical management, many cases of OME and ETD do not respond to this type of treatment. 14 Ai et al 27 reported no significant difference in the effective rates of BET+TT versus TT for the treatment of COME. A correlation between a short cartilaginous ET and failed BET has been reported. 28
A thickened mucosa in the tubal orifice may act as a barrier to ET ventilation and would not be directly addressed by BET of the cartilaginous aspect of the ET. 14 Both laser6,8 and microdebriders 9 have been used to treat a thickened mucosa of the cartilaginous tubal lumen and thereby improve ET function. However, because the cartilaginous tubal lumen is obscured, neither technique can effectively remove hypertrophic mucosa and could result in complications, such as closure or stenosis of the ET orifice.6,9 Other techniques have been used to manage a thickened mucosa of the ET orifice and have yielded satisfactory results.15,17-19 For example, Yañez 15 reported abnormal tympanogram improvement in 96% of patients and improvement of the subjective symptoms of ear blockage in 92% following cross-hatching eustachian tuboplasty. Zong et al 18 reported a success rate of 86.0% using RFA tuboplasty, and Lou et al 17 reported a success rate of 72.2% following microwave ablation tuboplasty. These results demonstrate that the management of a thickened mucosa can effectively improve ET ventilation.
We applied RFA eustachian tuboplasty combined with TT reinsertion to treat COME in patients with premature TT extrusion. All 23 patients had remarkable mucosal hypertrophic disease or polypoid changes in the posterior cushion or posterior wall. The tube retention success rate was 91.3%. ABG improved from 30.2 ± 1.7 dB preoperatively to 13.1 ± 4.6 dB postoperatively; the ABG gain was 18.3 ± 2.5 dB. The high success rate may be related to our strict patient selection criteria but it nonetheless demonstrates that RFA eustachian tuboplasty combined with TT reinsertion is effective for the treatment of intractable COME in patients with premature TT extrusion. Notably, of the 21 patients with intentional removal, despite nasopharyngeal ET orifice stenosis or pseudomembrane in a few patients, all had normal ET dilation, a positive Valsalva maneuver, and a well-aerated tympanic cavity and mastoid postoperatively. This suggests the absence of a significant correlation between the size of the ET orifice and the ET ventilation capacity, which may mainly depend on ET dilation. RFA eustachian tuboplasty may thus relieve the pressure of ET dilation caused by a thickened mucosa, in turn improving ET ventilation function even in patients with postoperative stenosis of the nasopharyngeal ET orifice. However, all of our patients had a history of previous TT insertion and premature extrusion, including multiple insertions and premature extrusion in 43.5%. After RFA eustachian tuboplasty, the TT was prematurely extruded in only 2 patients. Thus, whether the improvement in the remaining 21 patients was due to RFA of the nasopharyngeal ET orifice or to successful retention of the TT for more than a year is unclear. Although TT reinsertion may indeed have played a role, RFA eustachian tuboplasty is likely to have successfully addressed the obstruction caused by the hypertrophic mucosa of the nasopharyngeal ET orifice, in turn improving ET ventilation and avoiding premature extrusion of the TT.
Interestingly, in the 17 ears with perforation closure, a well-dilated ET and good aeration of the mastoid were achieved postoperatively. By contrast, in the 4 ears with persistent perforation, ET orifice stenosis and poor aeration of the mastoid could not be successfully treated. ET ventilation may therefore not suffice to completely improve aeration of the mastoid in patients with stenosis of the ET orifice; in such cases, perforation of the eardrum may be necessary. This may also explain the higher proportion of persistent perforations following early intentional TT removal in children. 29 In addition, in one of our patients with premature extrusion, a cholesterol granuloma was subsequently identified on pathological examination. This patient had grade 1 thickening without stenosis and synechia of the ET orifice; the postoperative CT showed no change and a soft-tissue shadow of the tympanic cavity and mastoid. Thus, in patients with multiple premature extrusions, magnetic resonance imaging should be performed to exclude cholesterol granuloma.
As in a previous study, 18 none of our patients reported RFA-related serious adverse events or a patulous ET. However, scar synechia of anterior-posterior wall was seen in the ET orifice of 1 patient and ET stenosis in the orifices of 4 patients. All tuboplasties were completed within 20 minutes after general anesthesia, and no patient reported postoperative pain. Previous studies have suggested that compared to laser and microdebrider eustachian tuboplasty, RF eustachian tuboplasty causes minimal postoperative pain and allows faster mucosal recovery.21-23 However, the limitations of this study were its small sample size, the absence of a control group, and the lack of an objective assessment of ET function.
Conclusion
RFA eustachian tuboplasty combined with TT insertion is a simple and minimally invasive technique for the treatment of intractable COME in patients with a thickened mucosa of the nasopharyngeal ET orifice. This approach may prevent premature extrusion of the TT.
Footnotes
Author’s Note
Author Contributions
Y.G.L. and J.Y.Z.: interpretation of data for the work, design of the work, analysis of data for the work, drafting the work, final approval of the version to be published; X.H.L.: analysis of data for the work, drafting the work and technical the diagram, and final approval of the version to be published.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by the Health Commission of Jiangxi province, China (Grants #2021KY1186).
Ethical/Consent Statement
The study protocol was reviewed and approved by the Institutional Ethical Review Board of 908th Hospital of PLA and Yu Jiang people’s hospital. All participants provided written informed consent.