
Abstract
Keywords
Introduction
The eustachian tube (ET) is a narrow tube that connects the middle ear cavity and the nasopharynx that is considered to be a unique organ due to its specific functions in the physiology of the middle ear. Eustachian tube dysfunction (ETD) refers to the inability of the ET to perform its function and is mostly diagnosed based on the presence of symptoms and signs of pressure dysregulation in the middle ear. ETD is classified as dilatory, barochallenge-induced or patulous dysfunctions. Dilatory ET dysfunction can be subdivided into obstruction and dynamic dysfunction. 1
Compared to adults, children have a shorter, more floppy, and more horizontal ET. Due to this anatomical peculiarity and the fact that children are highly susceptible to common viral infections and have more prominent adenoids and tubal tonsils, children are more likely to develop ETD. 2 Obstructive eustachian tube dysfunction (OETD) was found to have a prevalence of 4.4% to 6.1% among adolescents.3,4 However, this is likely underestimated in the pediatric population. It is estimated that approximately 40% of children will develop OETD in the form of chronic or recurrent otitis media with effusion, tympanic membrane retraction, or hearing loss, among other symptoms. 5
Currently, the surgical treatment of ETD associated with otitis media with effusion (OME) and other middle ear disorders is mainly indirect, involving ventilation tube (VT) insertion and adenoidectomy. 6 Recently, balloon eustachian tuboplasty (BET) with or without VT insertion has been a safe and effective treatment for chronic OETD that was reported to be first applied in pediatric patients in 2013. 7
However, due to the development of the anatomic peculiarities of patients with ET and different secondary disorders, OETD in children is quite heterogeneous. The effectiveness and safety of BET in patients with comorbidities and mixed hearing loss remain unclear. Therefore, further understanding of the possible predictive factors for OETD is crucial for selecting patients who could benefit from BET. To date, only retrospective cohort studies have been studied, and predictive factors have not been studied in children.
Therefore, we retrospectively compared the clinical data of children with OETD who underwent BET combined with VT insertion with those who underwent VT insertion alone to evaluate the efficacy and safety of BET combined with VT insertion and to identify the predictive factors for symptom recurrence.
Patients and Methods
Patient Selection
In this retrospective study, we analyzed data of 29 patients (48 ears) who were diagnosed with OETD and treated with BET combined with VT insertion (BET + VT group) between August 2018 and February 2022 at Shenzhen Children’s Hospital. As a control group, we assigned 29 patients with OETD (46 ears) who were treated with VT insertion alone during the same period to the VT group.
The inclusion criteria were as follows: (1) patients who were younger than 18 years of age; (2) patients who were diagnosed with OETD based on clinical manifestations of chronic otitis media with effusion, recurrent acute otitis media with effusion and adhesive otitis media 8 ; (3) patients whose conventional therapy including conservative treatments (eg, watchful waiting, antibiotics, corticosteroids, mucolytics, etc.) failed, patients who underwent VT insertion or adenoidectomy. The exclusion criteria were as follows: (1) patients with acute upper respiratory infections; (2) patients with an ET or internal carotid artery anatomical abnormality confirmed by computed tomography (CT) images; and (3) patients with a hemorrhagic disease or anesthesia intolerance.
We collected data from the patients’ medical records and charts, including otologic history and preoperative examination results such as age, sex, medical history of comorbidities, symptom duration, surgery history, preoperative diagnosis, ability to undergo Valsalva’s maneuver, available temporal bone CT data, pure tone audiogram (PTA, average hearing levels at 0.5, 1, 2, and 4 kHz) data, average air-bone gap (ABG, average hearing levels at 0.5, 1, 2, and 4 kHz) data, tympanogram results, and endoscopy results of the ear and nose. These assessments were used to evaluate ear symptoms such as physical suffering, hearing loss, speech impairment, emotional distress, and activity limitations.
This study was conducted in accordance with the Declaration of Helsinki and approved by the ethics committee of Shenzhen Children’s Hospital (2022133).
Surgical Procedures
After insertion of the short VT under general anesthesia, the eustachian tuboplasty procedure was performed using a balloon. If adenoid hypertrophy was present, patients with this condition underwent revision adenoidectomy. A 70° endoscope was inserted through the contralateral nostril or transorally to access the nasopharynx. Then, a standard balloon catheter measuring 3 mm in width and 20 mm in length was introduced into the ET. The saline solution was then injected into the balloon under 10 bar pressure for 2 minutes, after which the balloon was deflated, and the integrity was checked.
Follow-up
Patients were followed up at 1, 6, and 12 months postoperatively and then annually thereafter. If the VT remained in place for 6 months postoperatively, it was extracted, and the patient was scheduled for an ear evaluation 2 months later. This follow-up visit as well as the post-6-months follow-up were defined as the first follow-up after VT removal (6-9 months). The primary outcome was the ABG, and the other outcome measures included the ability to tolerate the Valsalva maneuver, and data on PTA, tympanogram, endoscopy, symptoms and adverse events. Children who did not attend their follow-up appointments were interviewed by telephone to assess the postoperative symptoms.
In this study, cure was defined as complete resolution of middle ear effusion and retraction, tympanogram switch to type A, an ABG ≤ 15 dB, and the absence of symptoms. Effective was defined as symptomatic improvement without complete resolution, tympanogram switch B to C or C to A, and the ABG decreased but remained >15 dB. Ineffective was defined as no relief of symptoms or signs. Failure time was defined as the time from the surgery date to the recurrence of ear symptoms and signs or the need for VT insertion.
Subgroup Analysis
Due to the concern that the effect of BET combined with VT insertion may differ in high-risk patients, we stratified patients by risk into 2 categories: high-risk patients and non-high-risk patients.
According to the Clinical Practice Guideline: Otitis Media with Effusion (Update), 9 high-risk patients were defined as patients with (1) permanent hearing loss independent of otitis media with effusion, (2) suspected or confirmed speech and language delay or disorder, (3) syndromes (eg, Down) or craniofacial disorders that include cognitive, speech, or language delays, (4) cleft palate, with or without associated syndrome, and (5) developmental delays.
Statistical Analysis
Statistical analyses were performed with SPSS (IBM SPSS 21.0, SPSS Inc.) and GraphPad Prism (GraphPad Prism 9; GraphPad Software, Inc). The optimum cutoff value was obtained using X-tile software (Yale University, version 3.6.1). Continuous variables were expressed as the mean ± SD if normally distributed and median (range) if not normally distributed. The independent sample T test was used to compare 2 independent groups. Paired comparisons were performed using the paired T test and the Wilcoxon paired signed rank test. Categorical variables were compared using the chi-square test and Fisher’s exact chi-square test. Kaplan‒Meier curves were used to analyze failure-free survival (FFS), and the log-rank test was performed. Kaplan‒Meier survival analysis with the log-rank test (P < .05) was included in a multivariate Cox proportional hazard model to identify independent prognostic factors. A P value less than .05 was considered statistically significant.
Results
Characteristics of the Patient
Forty-eight BET procedures combined with VT insertion were performed in 29 pediatric patients (72.4% male and 27.6% female), and 46 VT insertion procedures were performed in 29 pediatric patients (58.6% male and 41.4% female) between August 2018 and February 2022 at Shenzhen Children’s Hospital. The clinical characteristics of the study population are presented in Table 1. No significant difference was found between the 2 groups in terms of sex, age, types of hearing loss, symptom duration, follow-up duration, PTA, or ABG. However, there was a significant difference in the diagnosis and the characteristics of the high-risk patients between the 2 groups. Two patients, including 4 ears (8.3%), were lost to follow-up after the first follow-up after VT removal in the BET + VT group. No additional patients were lost to follow-up at the 12-month postoperative follow-up. During the first follow-up (6–9 months), all the patients in the study had their VTs removed and their tympanic membranes remained intact. Table 2 shows the times of tympanostomy tube removal in both groups.
Baseline Characteristics of Patients.
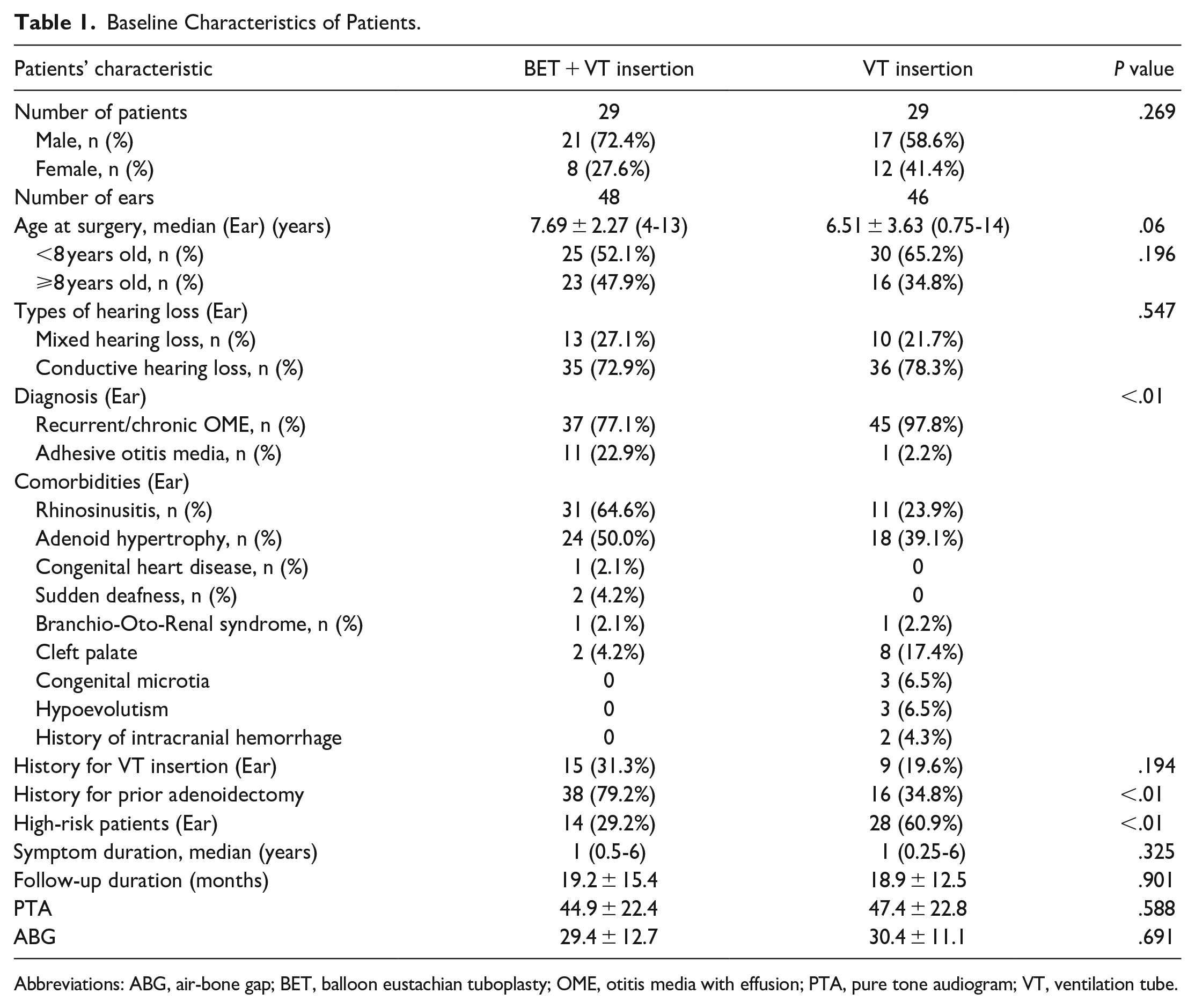
Abbreviations: ABG, air-bone gap; BET, balloon eustachian tuboplasty; OME, otitis media with effusion; PTA, pure tone audiogram; VT, ventilation tube.
VT Remaining in Both Groups, No Significant Differences (P > .05) Between Each Group and Subgroup.
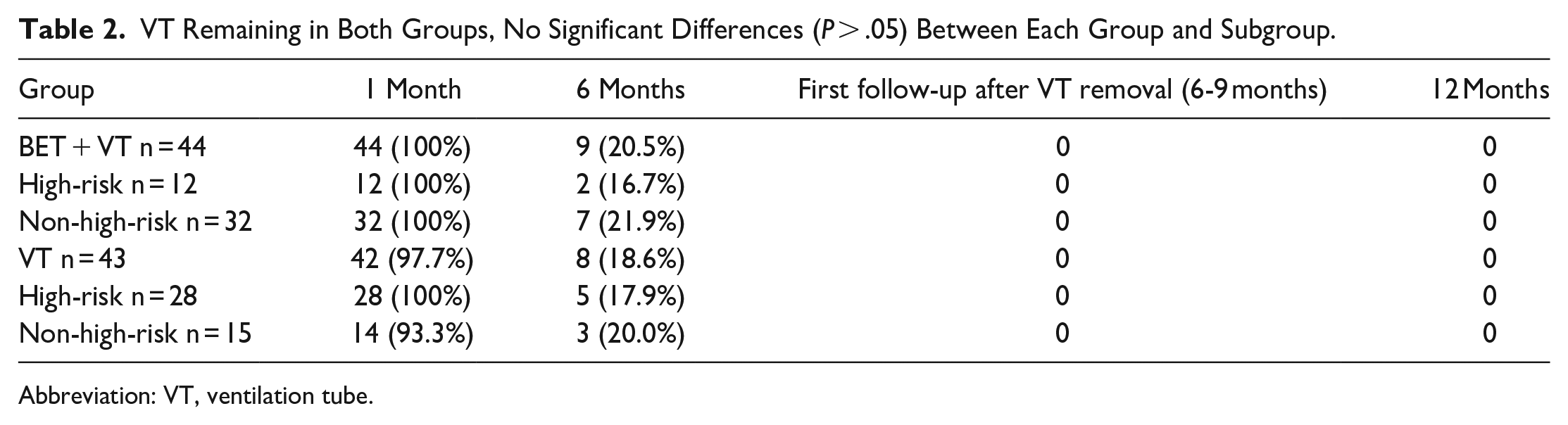
Abbreviation: VT, ventilation tube.
Efficacy and Safety of BET Combined With VT Insertion for Middle Ear Diseases
The changes in the evaluations of the middle ear from baseline to 12 months after surgery in the BET + VT group are shown in Table 3. The mean PTA decreased significantly from 44.9 ± 22.4 dB to 26.4 ± 16.5 dB (P < .01) at the first follow-up after VT removal (6-9 months) to 24.8 ± 19.6 dB (P < .01) at 12 months. Likewise, the mean ABG also significantly decreased from 29.4 ± 12.7 dB to 11.6 ± 9.3 dB (P < .01) at the first follow-up after VT removal (6-9 months) to 13.7 ± 12.9 dB (P < .01) at 12 months. The tympanogram type, tympanic membrane position, and the patients’ abilities to perform the Valsalva maneuver were significantly improved after the first follow-up after VT removal (6-9 months) (chi-square test, all P < .01). At the first follow-up after VT removal, the procedure cured 24 ears, was effective for 16, and ineffective for 4, resulting in a total effective rate of 90.9%. The total effective rate slightly decreased to 81.5% at 12 months post operation, with the procedure curing 16 ears, effectively treating 6, and ineffectively treating 5 (Table 4).
Change in Middle Ear Assessments in BET Group.
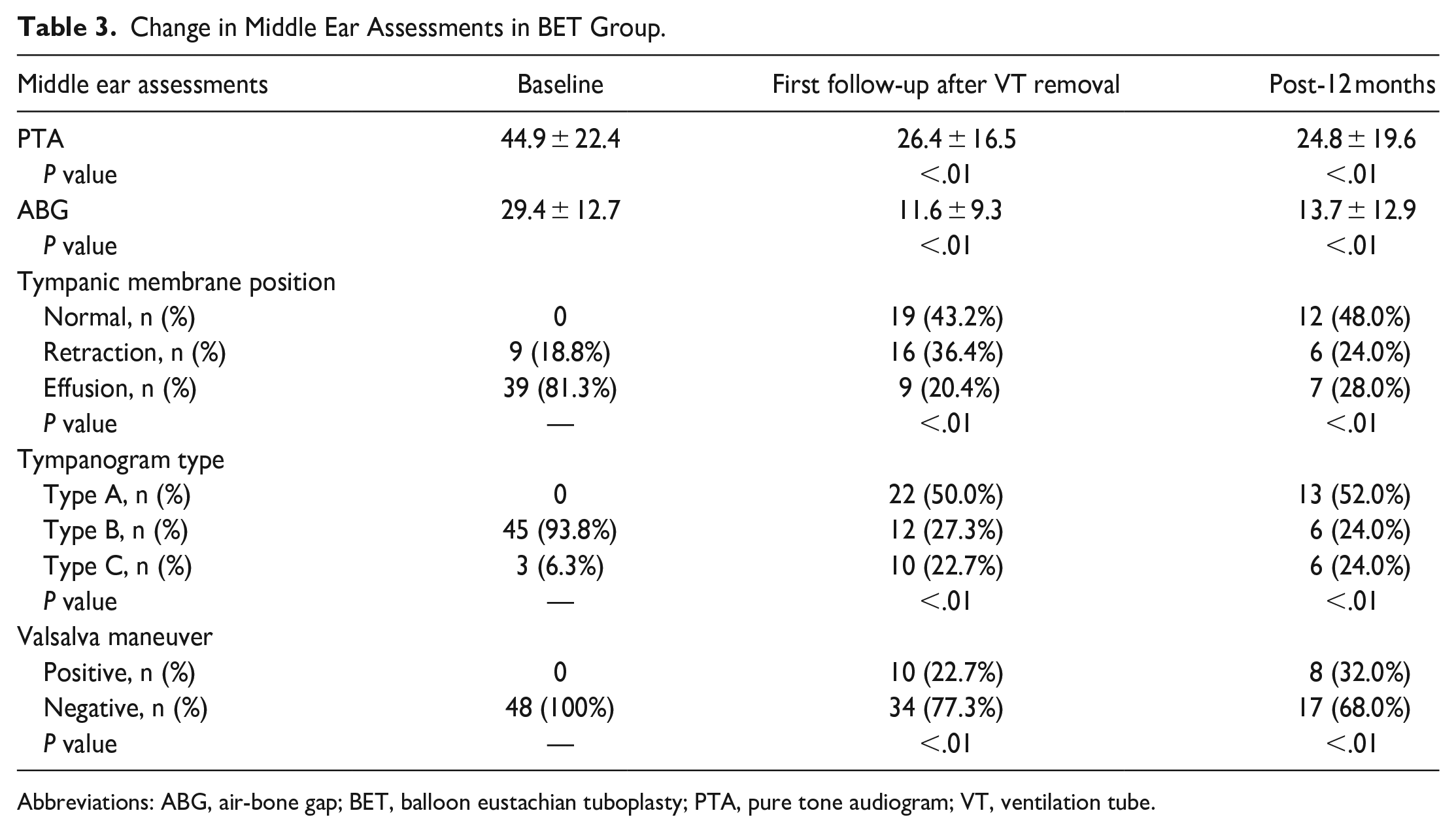
Abbreviations: ABG, air-bone gap; BET, balloon eustachian tuboplasty; PTA, pure tone audiogram; VT, ventilation tube.
Curative Effect in All Patients.
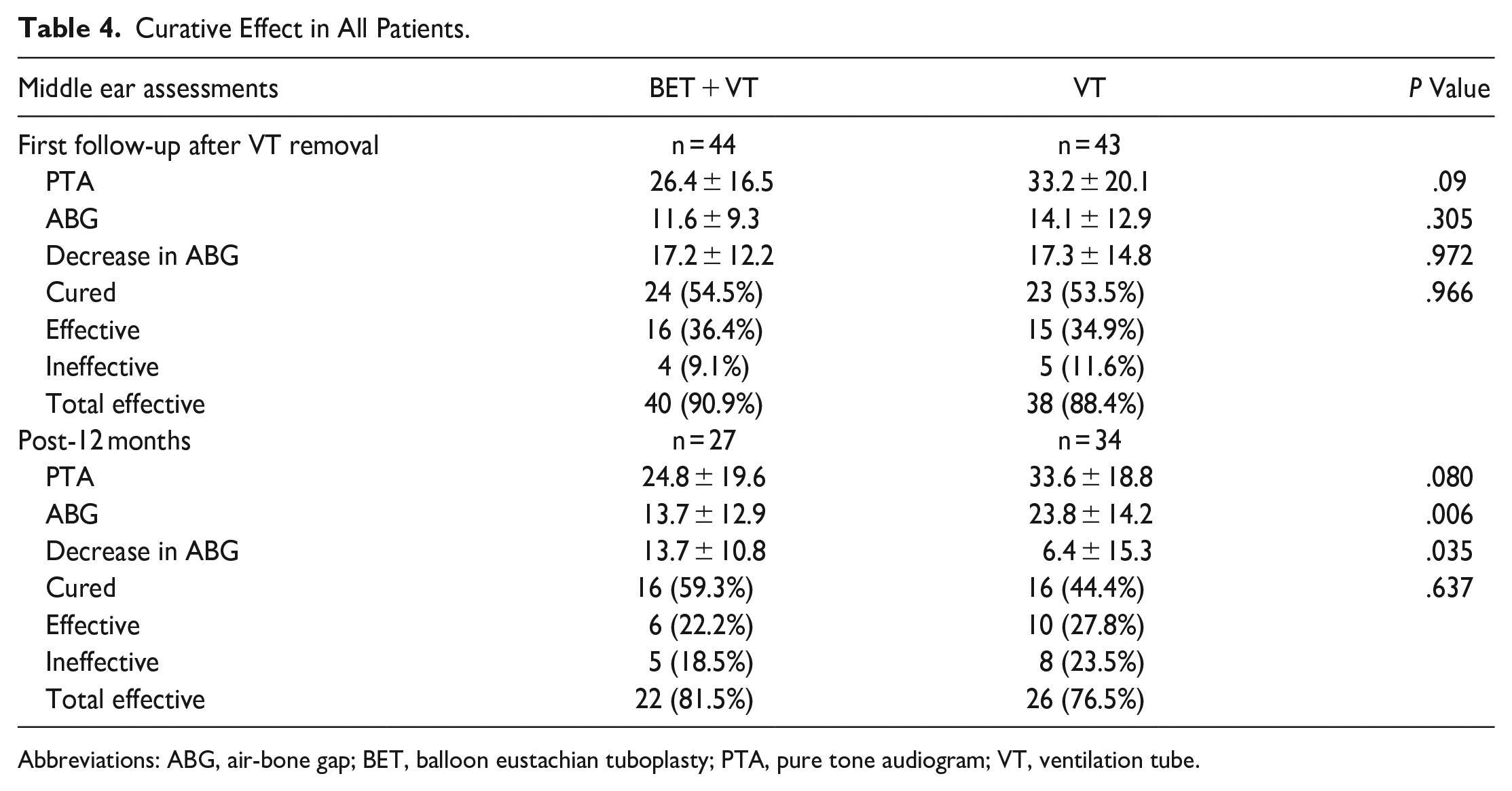
Abbreviations: ABG, air-bone gap; BET, balloon eustachian tuboplasty; PTA, pure tone audiogram; VT, ventilation tube.
Compared to the matched control group, there was no significant difference in the PTA or cure rate at the first follow-up after VT removal. However, a smaller ABG was observed in the BET + VT group at 12 months (13.7 ± 12.9 vs 23.8 ± 14.2, P < .01), and the decrease in the ABG was more significant in the BET + VT group (P < .05).
In the subgroup analyses, 42 ears were included in the high-risk group, with 14 ears that underwent BET combined with VT insertion and 28 ears that underwent VT insertion alone. Subgroup analyses revealed that there was no significant difference between the groups at either of the follow-up visits in terms of PTA, ABG, or cure rate (Table 5). In non-high-risk patients, the BET + VT group had a significantly smaller ABG at 12 months than the VT group (11.1 ± 9.5 vs 19.0 ± 10.9, P < .01), and the BET + VT group had a more significant decrease in the ABG (P < .05). However, there were no significant differences between the 2 groups at either of the follow-up visits in terms of other outcomes, including PTA, cure rate, and ABG at the first follow-up after VT removal (Table 6).
Curative Effect in High-risk Patients.
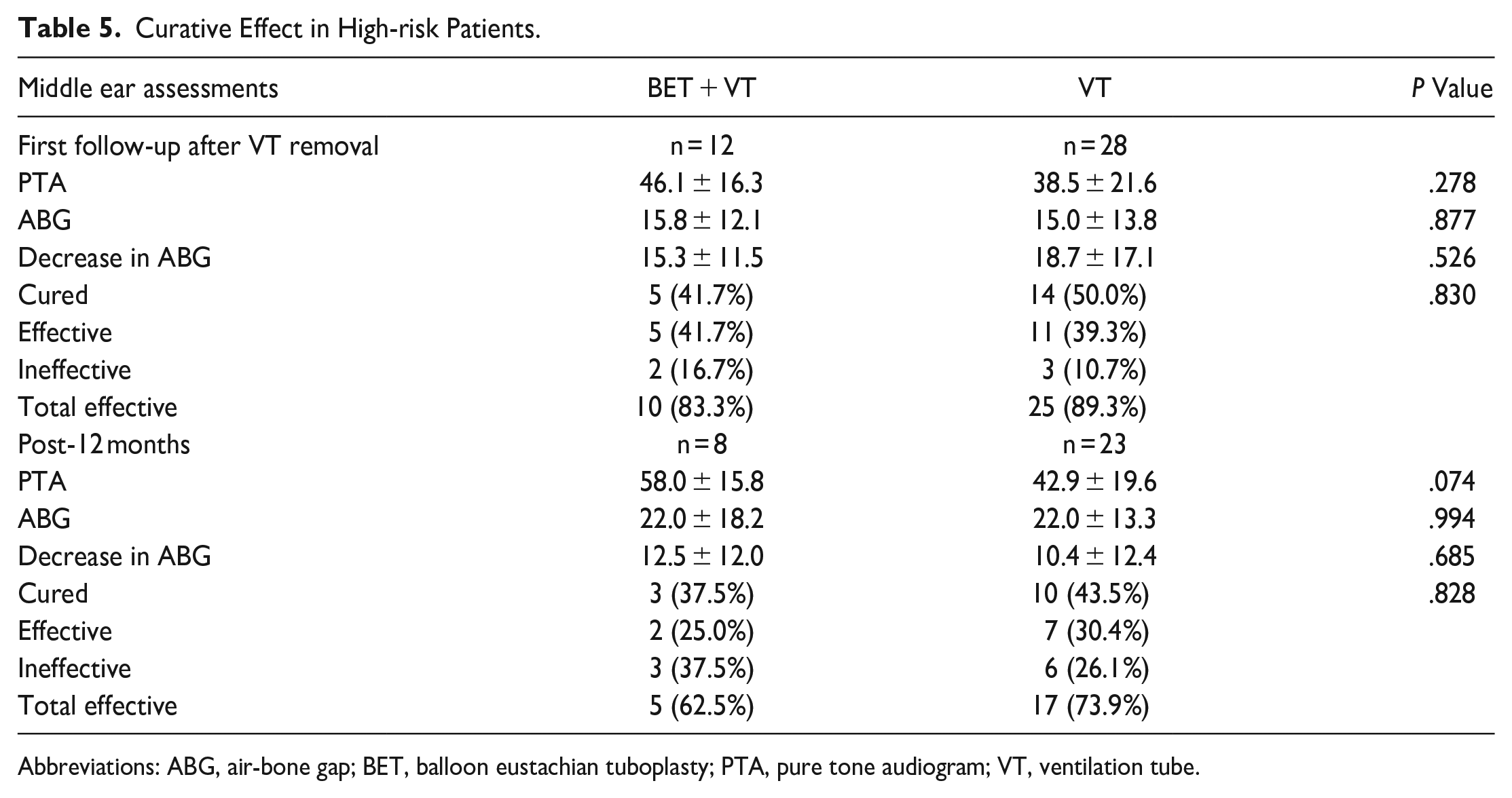
Abbreviations: ABG, air-bone gap; BET, balloon eustachian tuboplasty; PTA, pure tone audiogram; VT, ventilation tube.
Curative Effect in Non-high-risk Patients.
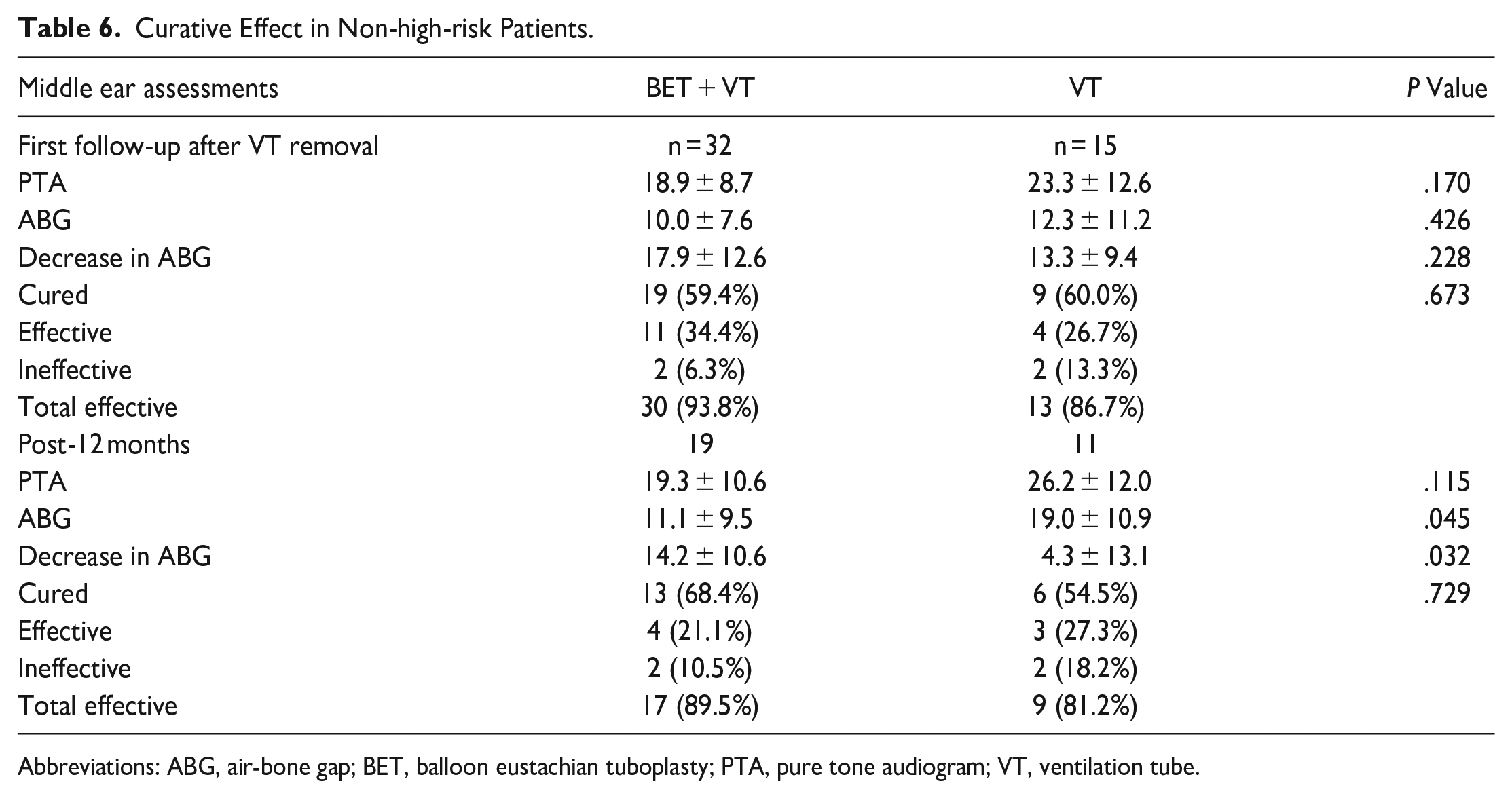
Abbreviations: ABG, air-bone gap; BET, balloon eustachian tuboplasty; PTA, pure tone audiogram; VT, ventilation tube.
Adverse Events
No patient developed any serious complications following BET. However, hemotympanum and ear bleeding were observed in 1 ear of a 5-year-old female patient who was promptly treated before discharge. Tympanic membranes were all healed at or before the 9-month follow-up. No patient in the VT group developed any complications.
Predictors for FFS in the BET + VT group
The mean duration of follow-up in the BET + VT group was 19.2 ± 15.4 months. During the follow-up period, recurrent ear symptoms were observed in 16 (33.3%) patients in the BET + VT group and in 27 (58.7%) patients in the VT group.
We performed a Kaplan‒Meier survival analysis to examine the possible factors impacting FFS in pediatric patients who underwent BET combined with VT insertion. The analysis revealed a significantly higher probability of recurrence of ear symptoms in male patients (log-rank test, P < .05; Figure 1a), patients with adhesive otitis media (log-rank test, P < .05; Figure 1b), patients with a history of VT insertion (log-rank test, P < .01; Figure 1c), and patients with ABGs smaller than 25 dB (log-rank test, P < .01; Figure 1d). The Kaplan‒Meier curve suggested worse outcomes in patients younger than 8 years old, with a disease duration longer than 2 years, no signs of rhinosinusitis, and a PTA value lower than 35 dB, but the difference was not statistically significant (log-rank test, .05 < P < .2; Figure 2). No difference was observed in the other parameters, including adenoid hypertrophy, special medical history, or type of hearing loss. Multivariate analysis showed that only a history of VT insertion was independently associated with a higher recurrence rate (hazard ratio 3.177; 95% CI, 1.027-9.826; P < .05; Table 7).
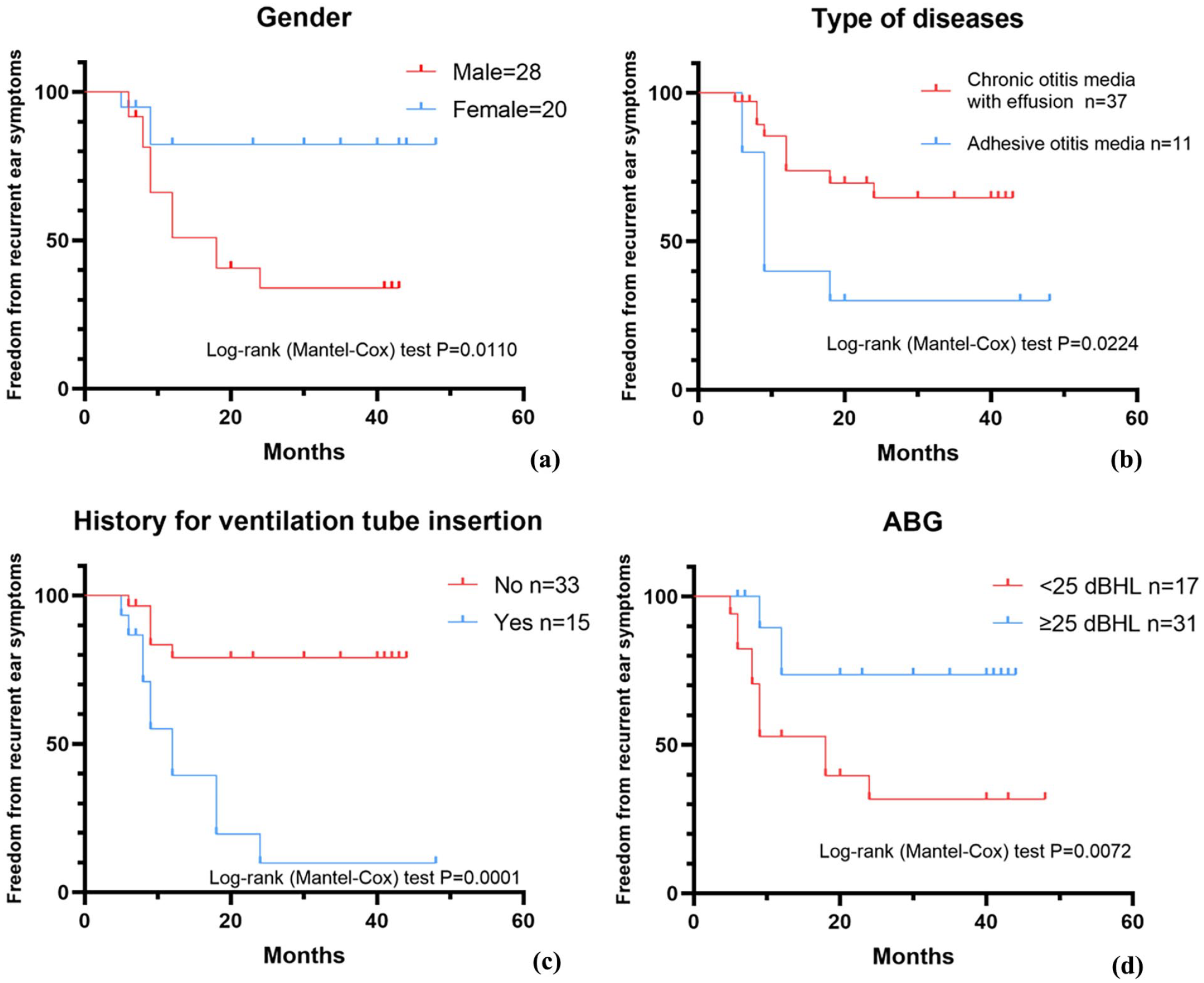
(a) Kaplan‒Meier curve of freedom from recurrent ear symptoms, by gender, (b) Kaplan‒Meier curve of freedom from recurrent ear symptoms, by type of diseases, (c) Kaplan‒Meier curve of freedom from recurrent ear symptoms, by history for VT insertion, and (d) Kaplan‒Meier curve of freedom from recurrent ear symptoms, by ABG.
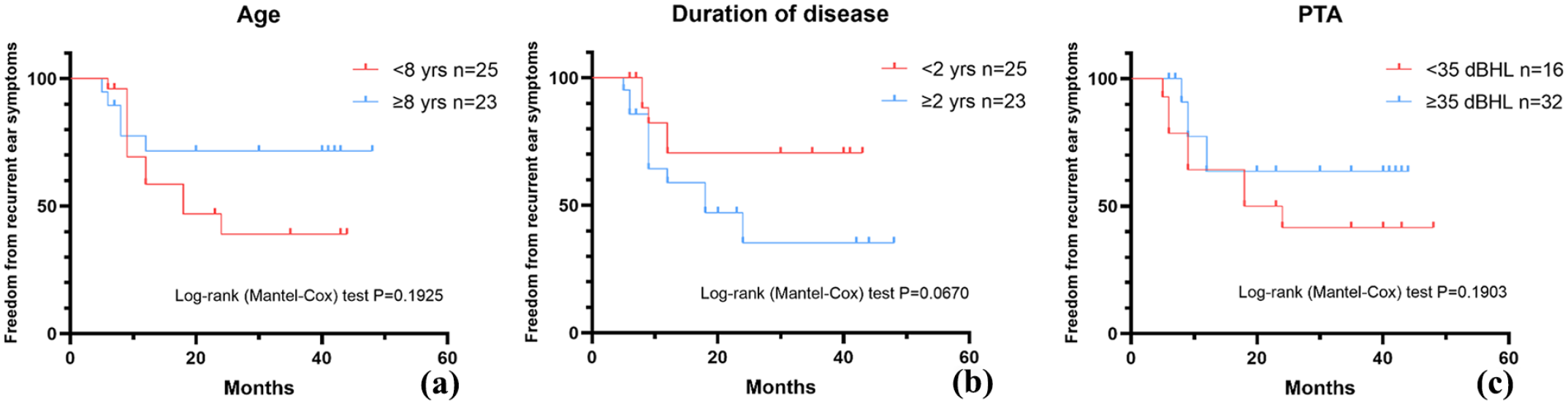
(a) Kaplan‒Meier curve of freedom from recurrent ear symptoms, by age, (b) Kaplan‒Meier curve of freedom from recurrent ear symptoms, by duration of disease, and (c) Kaplan‒Meier curve of freedom from recurrent ear symptoms, by PTA.
Multivariate Cox Regression Analyses of Freedom From Recurrent Ear Symptoms.
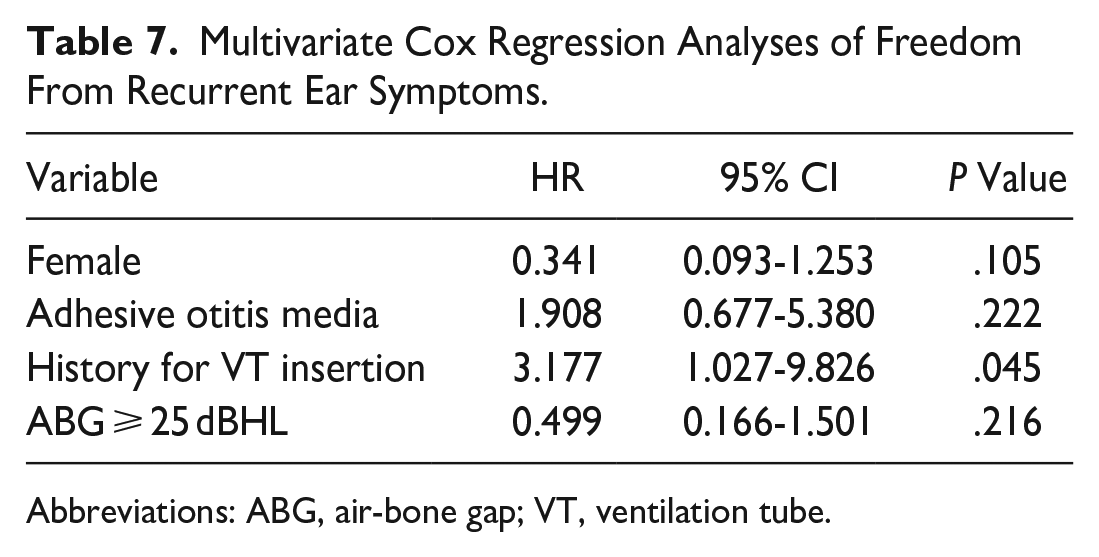
Abbreviations: ABG, air-bone gap; VT, ventilation tube.
Discussion
This retrospective study investigated the outcomes and prognostic factors of BET combined with VT insertion in children. OETD can manifest as chronic or recurrent otitis media with effusion and retraction of the tympanic membrane, among other symptoms. The insertion of VTs provides an alternative means of ventilating the middle ear space and is recommended as the first-line treatment in managing OME in pediatric patients according to guidelines. Nevertheless, it should be noted that this approach does not primarily address the issue underlying ET dysfunction and may be related to possible complications, including infection, persistent perforation, and tympanosclerosis.6,10 Although BET with or without VT insertion is not a traditional first-line treatment for otitis media in children, several studies have reported various advantages. A recent meta-analysis that included 408 children found that the BET group had a greater decrease in the postoperative ABG than the VT insertion group. The study concluded that the outcomes of patients who underwent BET for the treatment of otitis media with effusion may be comparable to those of patients who underwent tympanostomy. 11 It was found that BET improved the clinical symptoms (eg, otorrhea, otalgia, hearing loss) of approximately 80% of pediatric patients and provided a high degree of patient satisfaction.12-16 However, whether BET should be performed in conjunction with VT insertion remains controversial. Demir and Batman 17 found that, compared to VT insertion alone, BET with or without adenoidectomy led to a significantly greater decrease in the ABG. The study suggested that BET may be an effective first-choice therapeutic approach for OME in pediatric patients. Chen’s study found that BET combined with VT placement effectively extended the improvement period and increased the cure rate when compared to VT alone, especially after VT removal. 18 In addition, a study by Liang et al 19 found that for adults with intractable chronic otitis media with effusion, BET combined with paracentesis showed better outcomes than BET alone or paracentesis alone. In this study, patients underwent combined BET and VT insertion to promptly eliminate serous or mucoid fluid accumulation in the middle ear, balance pressure, and improve hearing levels.
Our results indicate that BET combined with VT insertion is effective for reducing the ABG in non-high-risk patients. However, this treatment was not superior to VT for high-risk patients. Similar to previous studies, our study reported a total effective rate of 90.9% at the first follow-up after VT removal and 84.6% at the 12-month follow-up. Previous studies have reported a range of symptom improvement rates after the procedure in children, from 80% to 93.5%.13,15,16,18. Chen et al 18 reported that BET combined with myringotomy and tube insertion for pediatric OME patients resulted in the best ABG after 6 months of follow-up and a gradual increase for up to 18 months. However, Toivonen et al 20 found that during 36 months of follow-up of pediatric ETD patients, the health of the tympanic membranes was improved, the results of the tympanograms were improved, and mucosal inflammation was relieved with BET. Similarly, in adult patients with OME, BET + VT has also shown therapeutic efficacy. 21 Compared to VT alone, BET + VT has led to significant improvements in clinical symptoms and a reduction in the disease recurrence rate in adult OME patients.22,23 Notably, there was heterogeneity in the study population and adjunctive procedures that may have contributed to the differences. Our results showed that in non-high-risk patients, there was no significant difference in the ABGs between the 2 groups at the first follow-up after VT removal. Prior to the removal of the VT, the VT effectively mitigated causing any noticeable ear symptoms in both groups. Additionally, this is reflected in the lack of significant differences in the first follow-up after VT removal. However, at the post-12-month follow-up, the ABG increased in both groups after VT removal, but the BET + VT group had significantly smaller ABGs than the VT group. We postulate that the significant increase in ABG values could be attributed to the removal of the tympanostomy tube, 24 whereas BET ameliorated this process through its unique effect on the ET. In addition, a ET with a small diameter was associated with the development of adhesive otitis media. 25 In the survival analysis, adhesive otitis media may potentially influence the recurrence of ear symptoms. In the BET + VT group, there was a higher prevalence of adhesive otitis media, which could have potentially led to an underestimation of the overall therapeutic effect of BET.
According to the Clinical Practice Guideline: Otitis Media with Effusion (Update), 9 high-risk patients have an increased risk of developmental difficulties (delay or disorder). In previous studies, BET was commonly performed in patients with OETD and pure conductive hearing loss. However, it is important to note that patients with comorbidities such as Branchio-oto-renal syndrome and Down syndrome may also experience OETD and present with mixed hearing loss.26,27 Furthermore, BET is not recommended in cases of cleft palate due to abnormal development of the tensor veli palatini and levator veli palatini muscles, which often lead to impaired opening and closing of the ET. 28 Although ETD in cleft palate patients may improve after palatoplasty, it remains a persistent challenge for some patients. Research has demonstrated that more than 90% of children who undergo palatoplasty for cleft lip and palate still experience recurrent OME. 29 Howard et al 30 reported a case in which a patient underwent myringoplasty, BET, and inferior turbinate outfracture. Following the surgical procedures, the patient achieved normal hearing, as evidenced by a type A tympanogram. However, the patient experienced vertigo that was associated with upper respiratory tract infection-like symptoms and was diagnosed with vestibular migraine. The study authors did not find a clear direct link between the BET procedure and vertigo. In our study, we undertook a tentative approach to perform BET surgery on these high-risk patients. We performed BET + VT on two 10-year-old boys who had undergone cleft palate repair but were still experiencing unilateral OME. One year after surgery, both patients had normal hearing, and the tympanogram showed type A. A 5-year-old girl with Branchio-Oto-Renal syndrome had unilateral OME and Mondini malformation. After excluding ET malformation, she underwent BET + VT. Eight months after surgery, her audiometry showed a 20 dB ABG and a C-type tympanogram. However, our results from the limited cases showed that BET combined with VT insertion was not significantly superior to VT insertion alone in terms of efficacy for high-risk patients. It should be noted that the heterogeneity of the patients in our group was substantial. Given the small number of children in the high-risk group, conducting a more detailed subgroup analysis would require a larger sample size to obtain more reliable results.
One ear in one patient without any high-risk factors presented hemotympanum and ear bleeding in our study. Although severe adverse events were not observed in our cohort, the risk may be higher in patients with preexisting comorbidities. According to the Clinical Consensus Statement: Balloon Dilation of the ET, since the introduction of BET, the need for a preoperative high-resolution CT scan of the temporal bone has been a controversial topic. 10 The need for CT dose protection is particularly crucial in children, and whether preoperative CT scans should be performed on pediatric patients is unknown. Some studies suggest that during BET, it is the cartilaginous portion of the ET that is dilated, not the osseous portion. This area is located at a safe distance from the carotid canal.15,17 No contraindications were found in our non-high-risk patients, and thus, CT scans may not be necessary. However, CT or MRI abnormalities are found in 20% to 50% of children with sensorineural hearing loss and are correlated with the degree of hearing loss. 31 CT scans may still be necessary in high-risk children to exclude possible abnormalities of the ET and the middle and inner ear.
In the present study, due to the limited number of cases and the heterogeneity between groups, we were unable to compare the FFS rates of patients in the BET + VT group with those in the VT group. Toivonen’s research showed that BET with or without VT insertion had a lower risk of failure than VT insertion alone in pediatric patients (age ≥ 7 years) with chronic ETD who had previously undergone VT insertion. 20 Our study identified several factors that may influence the recurrence of ear symptoms, including male sex, adhesive otitis media, history of VT insertion, and ABG value. Interestingly, our findings suggest that higher ABG values may be a positive predictor for the BET procedure. However, only the history of VT insertion remained a significant predictor after multivariate regression analysis. This may be because a history of VT insertion indicates refractory otitis media with effusion, which requires further comparative study to confirm the efficacy of BET. Given our findings, it may be beneficial to implement better follow-up care for this population. Li et al 21 suggested that BET can effectively improve the active and passive opening function of the ET and that BET combined with grommet insertion was effective for refractory otitis media with effusion. Mandel et al 32 reported on the predictive factors for recurrence of OME in children with VT insertion, showing that male sex, a shorter period of VT patency, and low dilatory efficiency were significant factors. However, they found that the number of previous VTs inserted was not a significant predictor of disease recurrence. Our current results, in combination with theirs, suggest a unique role of VT in BET.
The current study has several limitations that need to be acknowledged. First, some of the patients who underwent adjunctive procedures, such as revision adenoidectomy, may have benefited from these procedures rather than from BET + VT insertion alone. Second, this study was retrospective, with varying durations of follow-up, which may not have been sufficient determining a long-term prognosis. The limited number of patients also hindered more detailed subgroup analyses, which makes the data unreliable. Third, an objective evaluation of ETD in pediatric patients may not be entirely reliable. Although the validity and reliability of tubomanometry is still controversial,12,14 we did not include this examination.
Conclusion
In conclusion, BET combined with VT insertion is an effective procedure to decrease ABG for OETD pediatric patients without risk factors who underwent failure conventional therapy. A history of VT insertion is an independent predictive factor for the recurrence of ear symptoms in pediatric patients. The treatment of pediatric patients with ETD who have coexisting risk factors is still a challenge that requires further high-quality prospective research.
Footnotes
Author Contributions
D.J., Z.W., and H.P. contributed to the study conception and design; data acquisition, analysis, and interpretation; and drafting and critical revision of the manuscript. Y.C., X.W., G.X., J.C., and L.L. contributed to the study conception and design; data analysis and interpretation; and critical revision of the manuscript. All authors provided final approval and agree to be accountable for all aspects of the work.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Funding was provided by the Shenzhen Science and Technology Innovation Committee (JCYJ20210324143008022) (JCYJ20220530155603007).
Ethics Approval,Guidelines and Consent to Participate
All procedures performed in this study involving human participants were in accordance with the ethical standards of the institutional and national research committee and with the 1964 Declaration of Helsinki and its later amendments or comparable ethical standards. The study was approved by the ethics committee of the Shenzhen Children's Hospital (2022133). Due to all participants included in the study being under 18 years of age, informed consent was obtained from all individual participants’ parents and/or legal guardian.
Consent for Publication
Informed consent for publication was obtained from all patients’ parents for the use of their medical records in writing this study. All the authors have approved the manuscript and agree with submission to your esteemed journal.
Availability of Data and Materials
Data sets used and/or analyzed during the current study are available from the corresponding author (Z.W.,