
Abstract
Introduction
Rhabdomyoma (RM) is a rare benign tumor originating from striated muscle, classified into cardiac RM and extra-cardiac RM. 1 Cardiac RM mostly occurs in infants and young children, with approximately 75% of cases arising within the first year of life and 33% during the neonatal period.2,3 Cardiac RM frequently presents as an isolated lesion or in association with a tuberous sclerosis complex.4,5 In contrast to the clinical and pathological characteristics of cardiac RM, extra-cardiac RM is a solid tumor, yet the specific genetic alterations remain unclear. 6 Extra-cardiac RM can occur in all age groups, with 70% of cases involving the head and neck 1 and the rest occurring in other parts of the body. 7 Based on the degree of cellular differentiation, extra-cardiac RM can be further classified into adult, fetal, and genital types.6,8 Among them, although fetal RM is the second commonest type of extra-cardiac RM, accounting for approximately 40% of cases, the rarity of fetal RM has led to most studies being published in the form of case reports 9 with even less evidence available for fetal RM in the upper esophagus of children. This article reported on 4 pediatric cases of upper esophageal fetal RM, collected and analyzed the clinical medical records of these cases, and reviewed relevant literature, aiming to provide new insights into the clinical diagnosis and treatment of this disease.
Materials and Methods
General Information
From July 2016 to July 2022, the present study included a total of 4 children with fetal RM of the upper esophagus and analyzed their clinical medical records, who were admitted to the Department of Otolaryngology, Head and Neck Surgery, Beijing Children’s Hospital affiliated to Capital Medical University. All of the guardians of the children signed clinical informed consent forms. Among them, there were 2 boys and 2 girls, aged 2 to 6 years old, with an average age of 3.5 years. Their chief complaint was persistent dysphagia, with a disease course ranging from 17 to 60 months. All 4 children experienced occasional nausea, vomiting, and anorexia. There was no evidence of trauma, infection, developmental malformations, or foreign body ingestion. Due to their inability to consume more than a small amount of liquid food after the onset of the disease, these children exhibited delayed growth and development compared to their peers.
The 4 children underwent multiple imaging examinations, such as X-ray barium esophagography (Figure 1A to C), electronic endoscopy (Figure 1D), cervical computerized tomography (CT) scans (Figure 2A and B), or cervical magnetic resonance imaging (MRI) scans (Figure 3A to D). All patients were diagnosed with upper esophageal tumors and esophageal stenosis and underwent resection of the upper esophageal tumor with esophageal-pharyngeal reconstruction. Postoperative pathological and immunohistochemical results were consistent with fetal RM (Figure 4A to D). Detailed immunohistochemical results were showed as follows: MyoD1 (+), Desmin (+), Myogenin (+), Ki-67 (5%+), CK(AE1/AE3) (−),β-Catenin (−), SMA (−), S-100 (−), ALK (−), CD34 (−), CD68 (−). All patients received intravenous metronidazole and ceftriaxone for infection prevention, followed by intravenous omeprazole to inhibit gastric acid. Two of the children underwent prophylactic tracheotomy due to adhesion of the fetal RM and the recurrent laryngeal nerve. Postoperative follow-ups were conducted via outpatient clinic visits and/or telephone interviews for 25 to 96 months (Table 1).
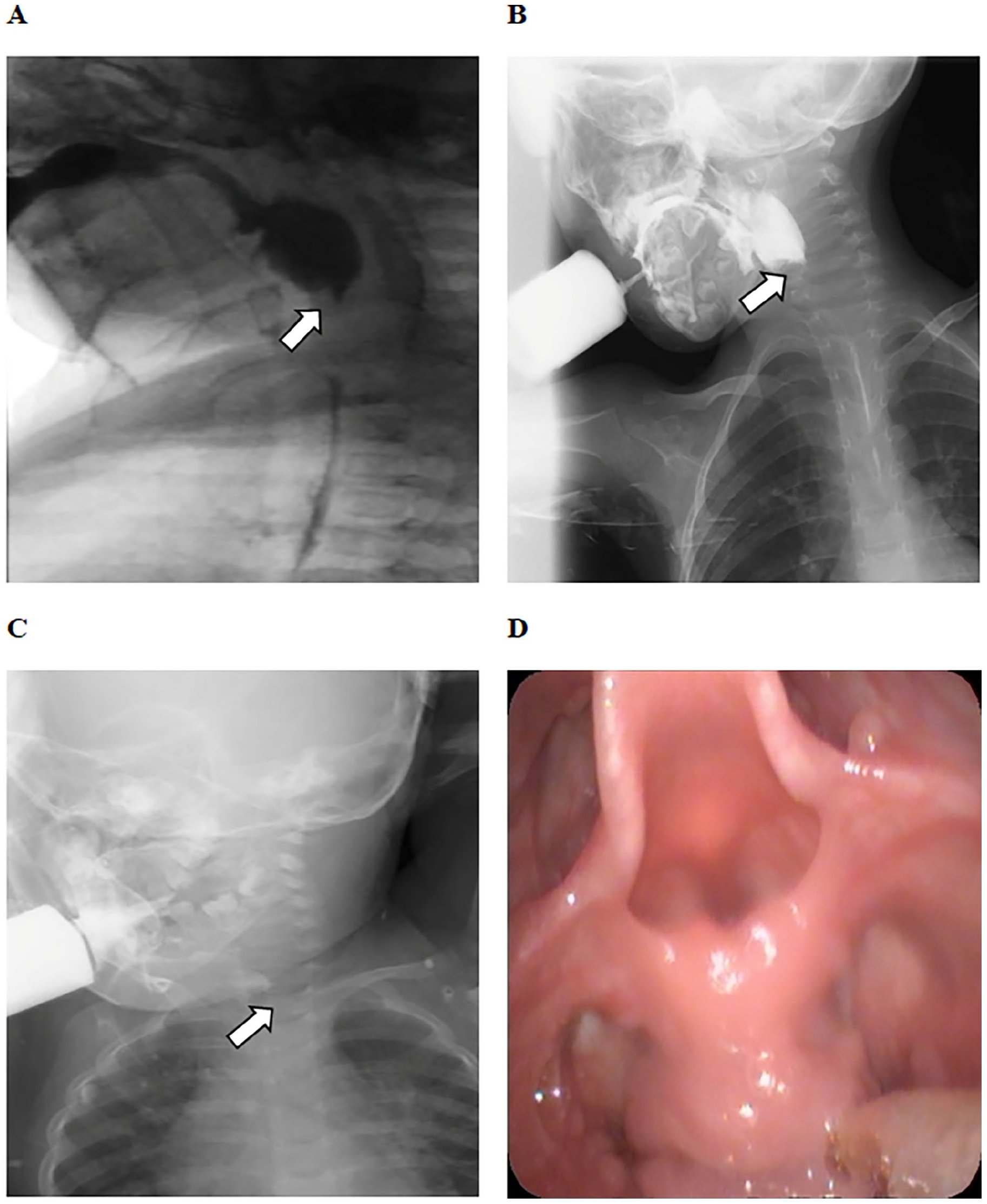
The X-ray barium esophagography of cases 1, 2, and 3, and the electronic endoscopy of case 4. (A) Case 1. (B) Case 2. (C) Case 3. (D) Case 4.
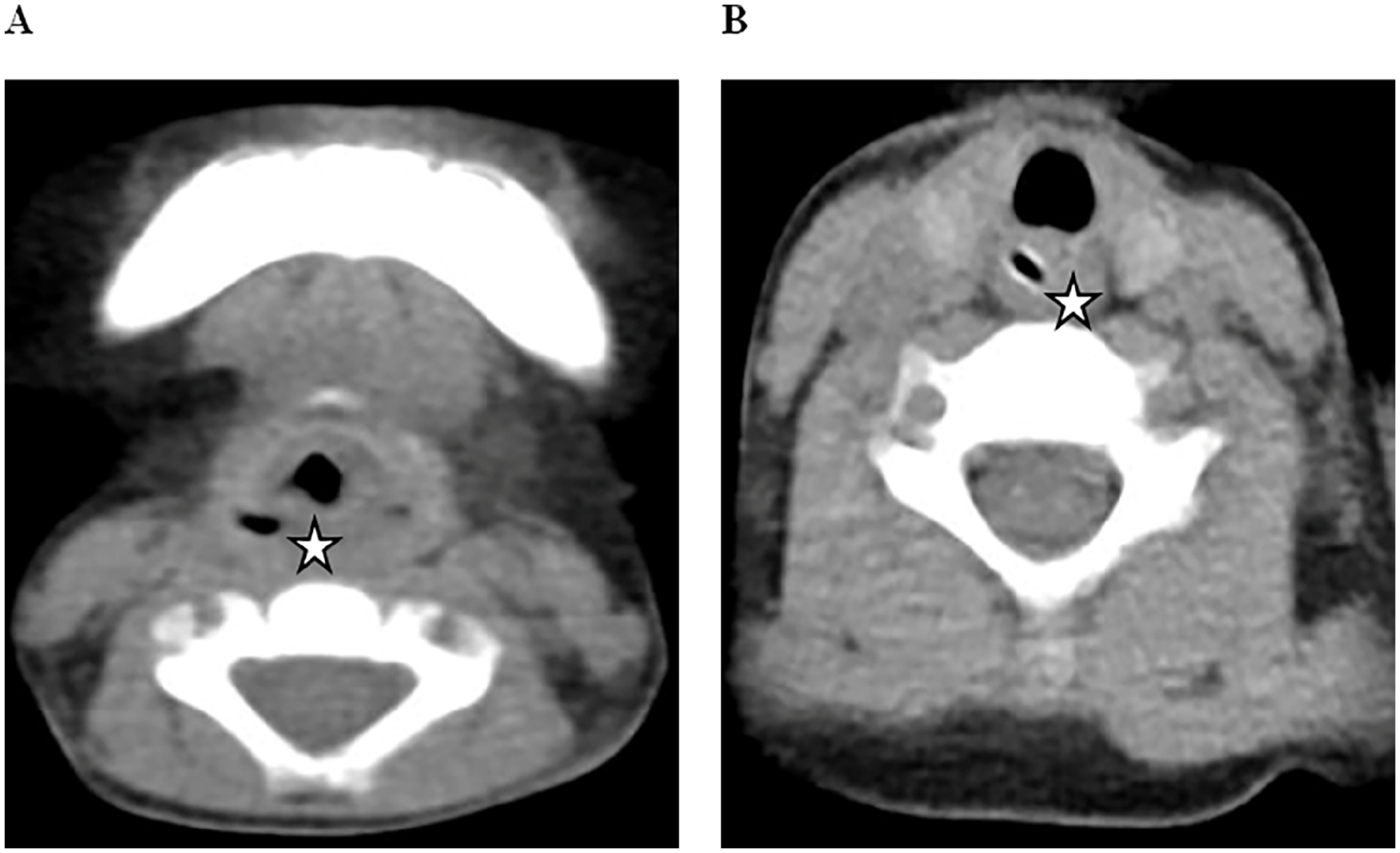
CT of case 1 and case 4. (A) Case 1. (B) Case 4.
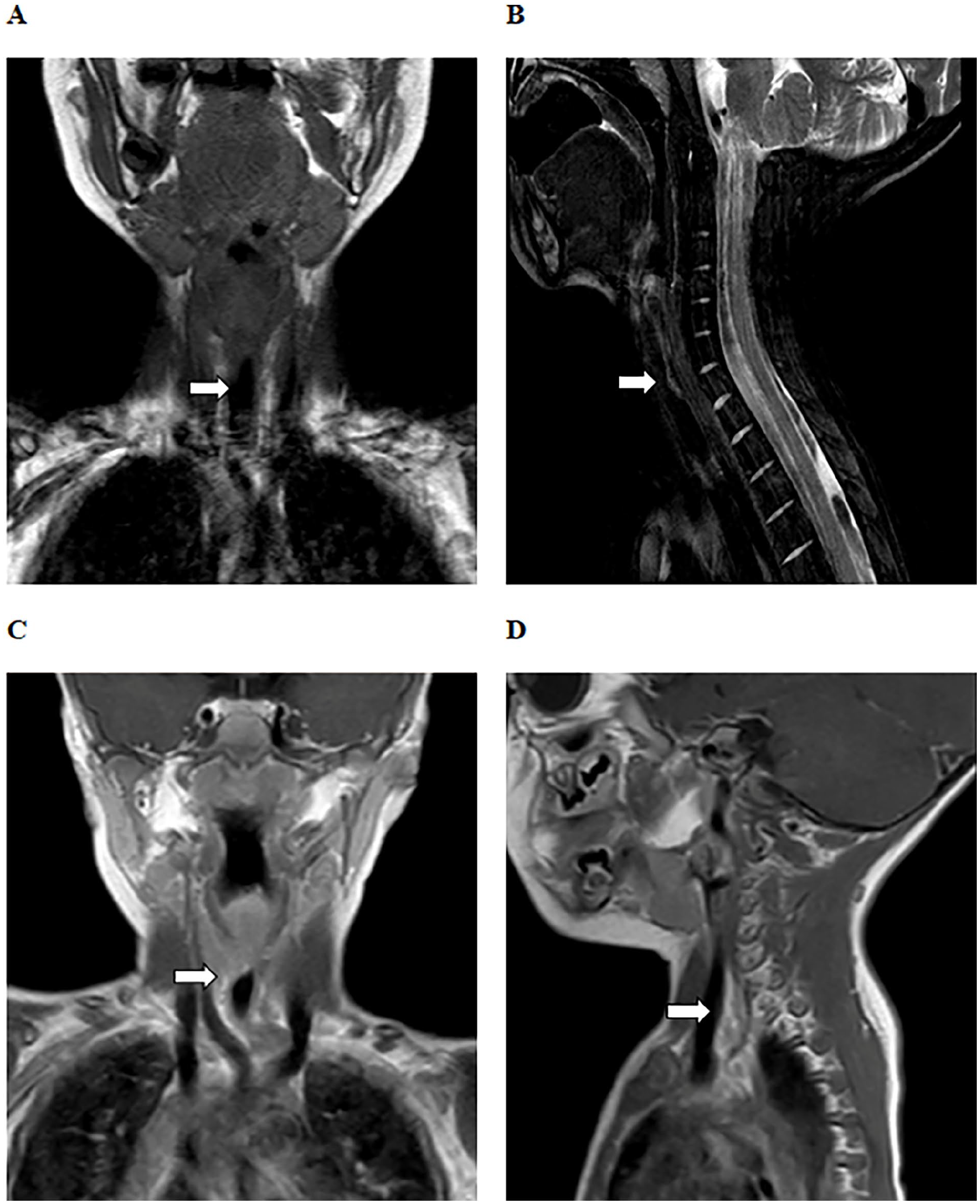
MRI of case 2 and case 3. (A and B) Case 2. (C and D) Case 3.
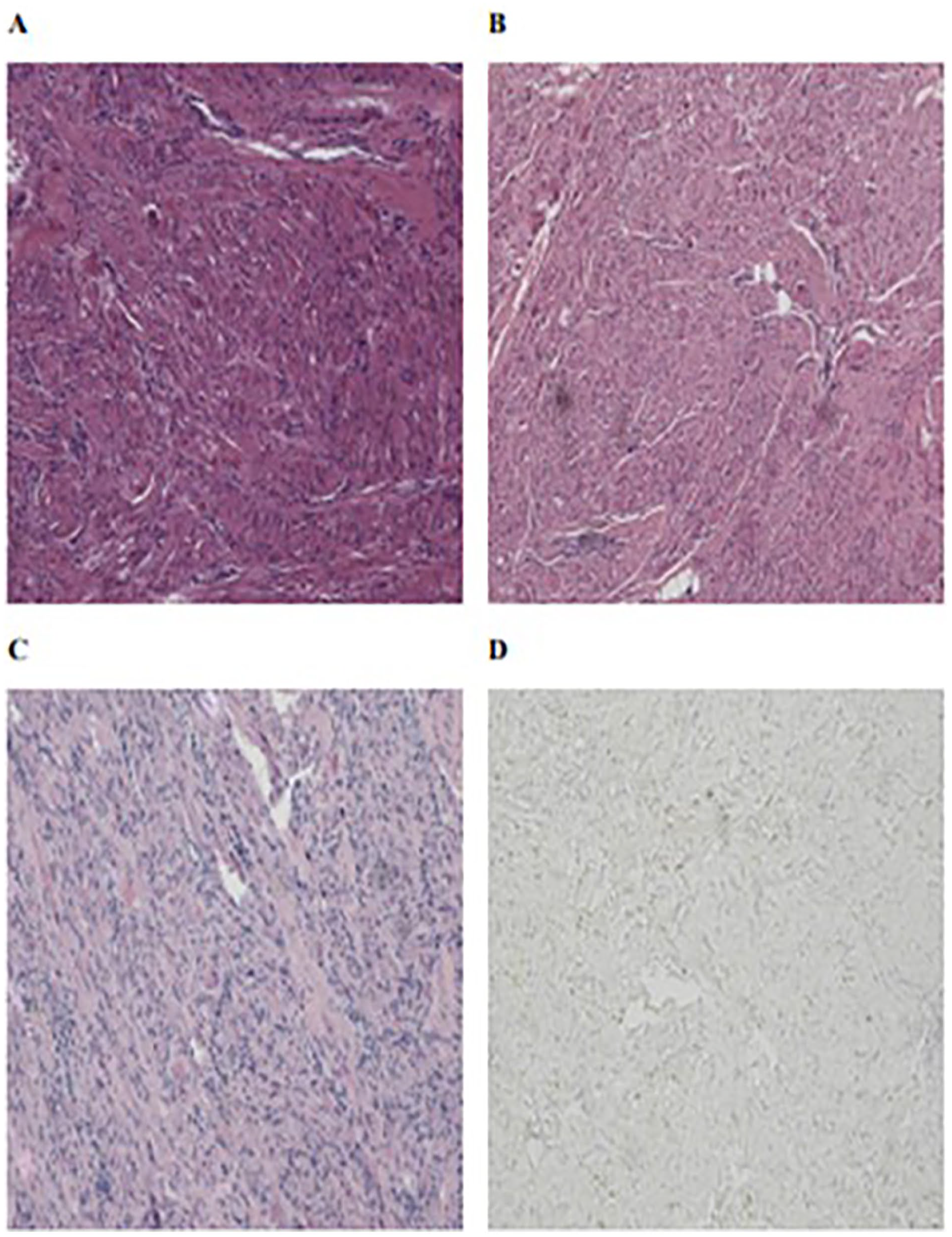
The pathological results of case 2, case 3, and case 4, along with the immunohistochemical results (MyoD1) of case 4. (A) Case 2. (B) Case 3. (C) Case 4. (D) Case 4.
Clinical Information of 4 Children with Upper Esophageal Fetal Rhabdomyoma.

Abbreviation: ICU, intensive care unit; RM, rhabdomyoma.
Patients’ Information
Case 1
A 2-year-old girl suffered from dysphagia for 20 months and was fed through a gastrostomy tube for long-term nutritional support. X-ray barium esophagography revealed an obstruction at the level of the fourth to seventh cervical vertebrae, and cervical CT demonstrated showed thickening of soft tissue in the same region of the upper esophagus, which was equal or slightly higher in density. The patient underwent resection of the upper esophageal tumor with esophageal-pharyngeal reconstruction under general anesthesia. Intraoperative frozen section analysis showed that the tumor was of spindle cell origin, and postoperative pathological and immunohistochemical results were consistent with fetal RM. The patient was transferred to the intensive care unit (ICU) on the day of surgery for sedation and supportive therapy to prevent wound tearing. She was transferred back to the general ward on the 11th day and discharged on the 20th day after surgery. The patient was followed up for 61 months after surgery and dysphagia recurred. Exploration of the upper esophagus under general anesthesia revealed significant stenosis at the entrance of the esophagus. A biopsy of the stenosis confirmed chronic hyperplasia with edema changes. After 2 esophageal balloon dilatations, dysphagia improved significantly, likely due to scar contracture. As of now, the patient has been followed up for 96 months without recurrence of dysphagia.
Case 2
A 6-year-old boy suffered from dysphagia for 60 months and relied on a gastrostomy tube for long-term nutritional support. X-ray barium esophagography revealed an obstruction at the level of the fourth to seventh cervical vertebrae, and cervical MRI showed localized thickening of soft tissue in the upper esophagus, with equal T1 and T2 signals or slightly shorter T1 and T2 signals. Preoperative biopsy of the upper esophageal tumor revealed the pathological and immunohistochemical results were consistent with fetal RM. Consequently, we performed resection of the upper esophageal tumor with esophageal-pharyngeal reconstruction under general anesthesia. During exploration of the neck structures, the tumor was unexpectedly found to be adherent to the left recurrent laryngeal nerve, which was carefully stripped and preserved intact. Additionally, the patient underwent prophylactic tracheotomy. Postoperatively, the patient developed hoarseness, and an electronic fiberoptic endoscope revealed left vocal cord paralysis. After 12 months of follow-up, dysphagia recurred and another cervical MRI showed a tumor in the upper esophagus, and the patient underwent a second tumor resection. Postoperative pathological results were again consistent with fetal RM, suggesting postoperative recurrence. Seven months after the second surgery, the patient was successfully extubated from the tracheotomy tube. To date, the patient has been followed up for 78 months without recurrence of dysphagia.
Case 3
A 2-year-old boy suffered from dysphagia for 17 months and was fed mainly through a gastrostomy tube for nutritional support. X-ray barium esophagography revealed an obstruction at the level of the third to sixth cervical vertebrae, and cervical MRI showed localized thickening of soft tissue at the same level in the upper esophagus, with equal T1 and T2 signals or slightly shorter T1 and T2 signals. The patient underwent resection of the upper esophageal tumor with esophageal-pharyngeal reconstruction under general anesthesia. During exploration of the neck structures, it was discovered that the tumor was attached to the bilateral recurrent laryngeal nerves, which could not be fully preserved despite careful dissection. A prophylactic tracheotomy was also performed. Intraoperative frozen section analysis showed that the tumor was of spindle cell origin, and postoperative pathological and immunohistochemical results were consistent with fetal RM. Postoperatively, the patient developed hoarseness and an electronic fiberoptic endoscope showed bilateral vocal cord paralysis. This child also developed a pharyngeal fistula on the ninth postoperative day, which was managed with routine wound dressings. After 18 months of follow-up, the patient was successfully extubated through the tracheotomy tube. To date, the patient has been followed up for 49 months without recurrence of dysphagia.
Case 4
A 4-year-old boy suffered from dysphagia for 55 months and was fed mainly through a nasogastric tube for nutritional support. Electronic endoscopy revealed a stenosis at the entrance of the esophagus, preventing the passage of a 3-mm fiberoptic endoscope. The cervical CT showed an obstruction at the level of the fourth to seventh cervical vertebrae, with thickening of soft tissue in the upper esophagus, which was equal to or slightly higher in density. Preoperative biopsy of the upper esophageal tumor revealed that the pathological and immunohistochemical results were consistent with fetal RM. Consequently, the patient underwent resection of the upper esophageal tumor with esophageal-pharyngeal reconstruction under general anesthesia. On the day of surgery, the patient was transferred to the ICU for sedation and supportive therapy to prevent wound tearing. Eight days later, the patient was transferred back to the general ward and discharged on the 18th day after surgery. Currently, the patient’s nasogastric tube has been removed, and he is feeding well on a regular diet with no recurrence of dysphagia.
Discussion
RM is considered a rare benign tumor and characterized by skeletal muscle differentiation, with cytological features demonstrating typical striated muscle cells. 10 Depending on the location of occurrence, RM can be classified into cardiac RM and extra-cardiac RM, with the latter being involved in the head and neck. 1 Based on the degree of cellular differentiation, extra-cardiac RM can be further categorized into 3 clinical and morphological types, namely, adult, fetal, and genital types, with prevalence rates of 50%, 40%, and 10%, respectively.6,8 Herein, we reported 4 children with upper esophageal fetal RM and discussed their clinical, histological, and therapeutic characteristics, combined with a review of the literature, aiming to provide new insights into the clinical diagnosis and treatment.
Fetal RM is often detected at birth or even during pregnancy 11 and occurs predominantly in the head and neck, especially in the retro-auricular regions,11,12 with few cases reported in other regions, such as the costal margin, 13 abdominal wall, 14 chest wall, 13 extremities,7,12 stomach, 6 perianal region, 15 and bladder, 16 etc. Furthermore, fetal RM is pathologically classified into 3 subtypes, including typical subtype, myxoid subtype, and intermediate (cellular or juvenile) subtype, the last subtype posing diagnostic challenges due to its histological features lying between those of typical fetal RM and adult RM.12,17,18 The clinical symptoms of fetal RM are often non-specific, manifesting as slow-growing, painless, and variable-sized masses in different anatomical locations, ranging from 2 to 5 cm in size,8,13,17 which can lead to misdiagnosis or underdiagnosis. In our series, 4 children presented with persistent dysphagia, with a history ranging from 17 to 60 months. The prolonged period between onset and diagnosis (i.e., more than 1 year) along with their multiple visits to clinics without a definitive diagnosis imposed significant financial and emotional burdens on the children and their parents. Therefore, prompt biopsy of upper esophageal masses is crucial for definitive diagnosis and guiding treatment.
In contrast to adult RM, which is characterized by mature skeletal muscle differentiation, fetal RM exhibits immature skeletal muscle differentiation, characterized by irregularly arranged spindle-shaped cells with fetal myotubes in an abundant myoid matrix.17,19 Histologically, fetal RM consists of relatively small eosinophilic cells with peripheral nuclei, sometimes surrounded by pseudoepithelial cell proliferation. 20 Morphologically, skeletal muscle differentiation can be easily demonstrated through immunohistochemical staining for muscle-specific actin, Desmin, and Myosin; thus, most fetal RMs show immunoreactivity for these biological markers, with only a minority also expressing S-100.17,20,21 Based on these histological and morphological settings, fetal RM can be easily distinguished from other benign tumors such as granular cell tumors, hibernoma, oncocytoma paraganglioma, oncocytoma, and crystal-storing histiocytosis, etc.20,22-25
Currently, the treatment of choice for fetal RM is surgical resection, as evidenced in most case reports and studies.13,26 Lapner et al 15 found recurrence in 5 of 43 patients (11.6%), 2 of which recurred as rhabdomyosarcoma, suggesting the possibility of malignant transformation of fetal RM. Additionally, Zheng et al 27 reported a case of a 12-year-old boy with paratesticular fetal RM who did not experience local recurrence within 5 years. Given that fetal RM predominantly affects the head and neck region in younger patients,11,12 surgical procedures are often associated with complications such as hemorrhage and recurrent laryngeal nerve injury, especially the latter of which can lead to hoarseness, vocal cord paralysis, and even respiratory distress in patients with bilateral recurrent laryngeal nerve injury. Therefore, while surgeons aim to remove the tumor as quickly as possible, great care must be taken to preserve the integrity of neural structures. In the present study, 2 of the 4 children with upper esophageal fetal RM had significant recurrent laryngeal nerve adhesion. To ensure normal ventilation in these patients, we performed a prophylactic tracheotomy during intraoperative exploring. Postoperatively, both children had their tracheotomy tubes extubated within 1 and a half years. And now, their operative wounds have healed well, their diets have been sufficient, and their respiration has been stable.
While a thorough understanding of the clinical, histological, and therapeutic characteristics of fetal RM is essential, it is also crucial to develop and standardize the management algorithm for this condition. Here, we proposed a preliminary management algorithm for fetal RM based on our own diagnostic and treatment experiences, which can serve as a reference for clinicians (Figure 5). Additionally, some recommendations are noteworthy. First, preoperative biopsy of upper esophageal masses is recommended to confirm the diagnosis. Second, the possibility of upper esophageal malignancies (e.g., embryonal rhabdomyosarcoma) should be considered in differential diagnosis, necessitating more aggressive comprehensive treatment based on surgery and regular follow-up. Lastly, even after surgical resection, fetal RM may recur years later.8,28 Thus, the long-term follow-up plays a vital role in the assessment and management of the fetal RM.
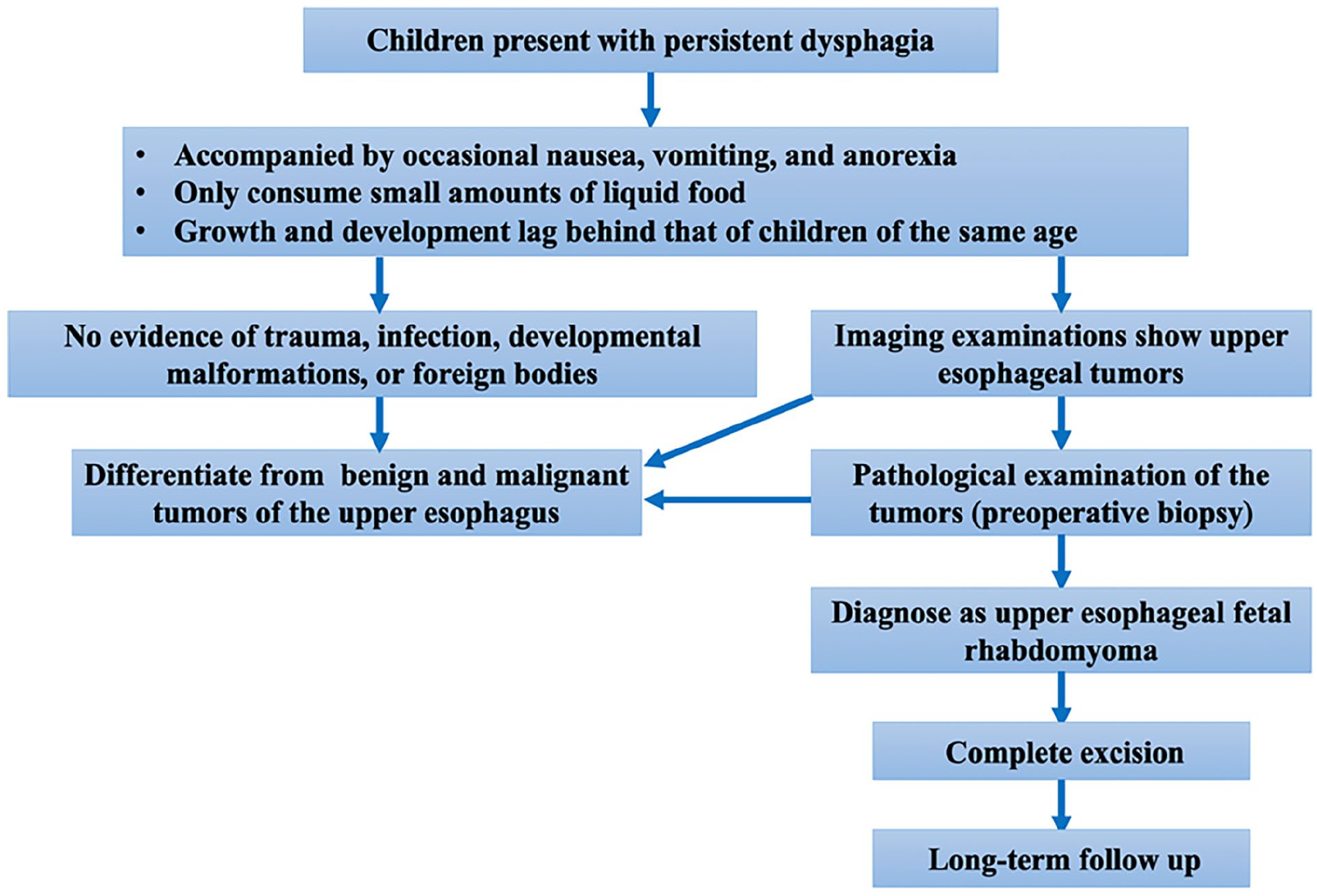
The preliminary management algorithm for fetal RM.
Certainly, there are also some limitations that need to be considered. First, due to the rarity of the fetal RM and the limited sample size, we were unable to conduct statistical analysis on the cases of this condition, which weakens the statistical power of our results. Second, although preoperative biopsy of the upper esophageal mass is the ideal choice for diagnosis, only 2 cases (case 2 and case 4) underwent preoperative biopsy, whereas the other 2 children (case 1 and case 3) underwent intraoperative frozen section and surgical resection, with the diagnosis confirmed by postoperative pathology. In the future, we need to continue standardizing the clinical diagnosis and treatment of fetal RM in the upper esophagus. Finally, our follow-up period was not long enough, and there is a need for continued follow-up in the future, for the collection of detailed information, and for an objective assessment of prognosis.
Conclusion
In summary, our study reported 4 children with fetal RM in the upper esophagus, a condition that is extremely rare both nationally and internationally. The clinical and imaging features of fetal upper esophageal RM are atypical, making differential diagnosis challenging, particularly in distinguishing it from malignant tumors of the upper esophagus. Accurate pathological examination is crucial for the correct diagnosis of this condition. Although fetal RM is a benign lesion, it is prone to recurrence, thus complete excision is the preferred optimal treatment. Care must be taken to avoid unnecessary surgical complications, such as recurrent laryngeal nerve injury. A preliminary treatment management algorithm can assist and standardize clinicians’ efforts in treating this condition.
Footnotes
Author Contributions
Prof. Xin Ni, and Prof. Shengcai Wang: designing this study; and revising the work critically for important intellectual content; and final approval of the version to be published; and agreement to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved. Dr. Yanzhen Li, Dr. Xuexi Zhang, Dr. Qiaoyin Liu, and Dr. Nian Sun: completing the acquisition, analysis, or interpretation of data for the work. Dr. Tingting Ji, Dr. Xiaodan Li, and Dr. Yuwei Liu: searching for relevant literature sources and recorded the information for the follow-up. Dr. Zhiyong Liu and Mr. Yiran Meng: composing the original manuscript. All the authors listed have read through the manuscript, approved for publication, and declared no conflict of interest.
Consent Statement
All the authors listed have read through the manuscript, approved for publication, and declared no conflict of interest.
Data Availability
The data used to support the findings of this study are available from the corresponding author upon request.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was supported by the National Natural Science Foundation of China (82000991; 82271184), and the Capital Health Development Scientific Research Project (2022-1-2092).
Ethics Approval and Consent to Participate
This study was approved by the Medical Ethics Committee of Beijing Children’s Hospital, China. All of the guardians of the children signed the clinical informed consent forms.