
Abstract
Hamartoma is a congenital benign lesion commonly found in the lungs, kidneys, colon, and other regions, but it is seldom seen in the oral cavity. Multiple hamartoma occurrences in the tongue are particularly rare. This article describes a 7-day-old female infant with multiple tongue tumors and a cleft palate, who had difficulty feeding and subsequently underwent tumor removal under general anesthesia. Nine months later, a cleft palate repair was performed. No genetic abnormalities were detected in the genetic testing. After the tumor removal, follow-ups were conducted every year to observe any recurrence of the tumors, the morphology and function of the tongue, and any systemic abnormalities. After 7 years of follow-up, there was no recurrence of the tumors, and the morphology and function of the tongue were normal, with no systemic diseases found. It is crucial to conduct multidisciplinary consultations for children diagnosed with multiple tongue hamartomas and to monitor their overall development while addressing oral lesions.
Introduction
Lingual hamartoma is a rare congenital benign lesion, first reported by Stamm and Tauber in 1945. It typically occurs as a solitary tumor but is exceedingly rare in multiple instances. 1 Associated genetic alterations have been noted. The pathogenesis of lingual hamartomas remains unclear; however, existing studies suggest a correlation with genetic factors, gene mutations, and developmental anomalies, underscoring the necessity for genetic testing. Tongue hamartomas commonly comprise adipose tissue, smooth muscle, blood vessels, nerves, and salivary gland tissue.1,2 Owing to its varied clinical presentations, diagnosing this condition can be complex. This paper presents a case of a neonatal female with multiple tongue hamartomas, detailing the symptoms, diagnostic process, treatment, and follow-up outcomes, thereby serving as a reference for clinicians in managing such cases.
Case Report
A 7-day-old female neonate presented with multiple nodular masses on the tongue and a cleft palate, identified postnatally. The tongue exhibited lobulation, affecting feeding and prompting hospital admission. Examination revealed 2 pale pink nodules at the tongue’s tip, 2 on the lingual margin, and 1 at the root, with the largest, measuring approximately 1.0 × 0.6 × 1.0 cm, located on the right lingual margin. The soft palate was also split (Figure 1a). Routine laboratory tests, including complete blood cell count, electrolyte panel, and urine analysis, were within normal limits, with no detected endocrine or metabolic anomalies. Genetic testing revealed no abnormalities. Due to the tumor’s size impacting normal feeding and swallowing, surgical removal of the multiple tongue tumors was performed under general anesthesia, and the tongue’s morphology was restored. Histopathological analysis revealed hyperplastic glandular tissue, vascular epithelium, smooth muscle, adipose, and cartilage tissue (Figure 1b), confirming a diagnosis of multiple hamartomas of the tongue. Cleft palate repair was conducted at 9 months to correct the palatal shape. Following a 7-year follow-up, the patient showed no recurrence, maintained good tongue morphology (Figure 1c), and exhibited normal speech function with well-recovered palatal structure.
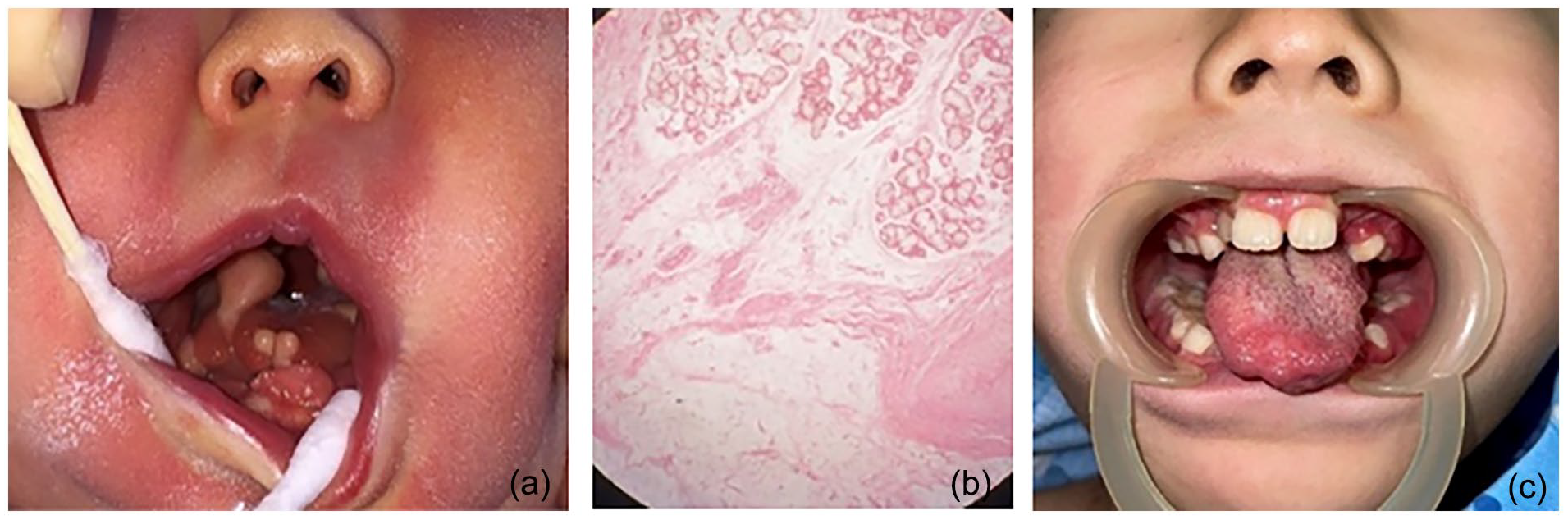
(a) Multiple nodular masses on the tongue and a cleft palate. (b) Hyperplastic glandular tissue, vascular epithelium, smooth muscle, adipose, and cartilage tissue (Hematoxylin-Eosin staining 10×). (c) The patient showed no recurrence and maintained good tongue morphology.
Discussion
Hamartoma is a congenital tumor-like malformation characterized by benign tumors arising from the abnormal arrangement or growth of normal tissues. These tumors display a disorganized structure with blurred boundaries, merging with the surrounding tissues. Typically, hamartomas occur in the gastrointestinal tract and respiratory system, with multiple occurrences in the oral cavity being uncommon.2-4 There is a propensity for these lesions to coexist with systemic developmental abnormalities, such as cleft palate, frenulum attachment abnormalities, and toe deformities. 5 Surej Kumar and Hiebert et al6,7 have suggested that the presence of a tongue mass during the embryonic period may mechanically interfere with the development of the tongue and palate, potentially leading to conditions such as cleft tongue and cleft palate, as observed in this case.
The etiology of tongue hamartoma remains unclear; it may be associated with gene mutations or environmental factors during embryonic development. These influences could cause abnormal proliferation and distribution of normal tissues. Moreover, maternal exposure to certain harmful chemicals or radiation during pregnancy could also elevate the risk of fetal hamartomas. Reports indicate that tongue hamartomas predominantly occur in female children under the age of 2, and are more commonly found on the posterior surface of the tongue. 8 This paper discusses a case involving multiple tongue masses accompanied by a cleft palate in a child. The lingual margin is lobulated, with lesions present at the tip of the tongue, along the lingual margin, and at the root of the tongue.
The studies by Velcek and Horn on tongue lesions revealed a low incidence of hamartoma, often leading to its neglect and difficulty in diagnosis within this context.9,10 Differential diagnosis for hamartoma typically includes choroidoma, teratoma, rhabdomyosarcoma, and glioma,1,7 which are generally distinguished through histopathological analysis. Choroidoma, characterized by nodular hyperplasia of normal tissues in abnormal anatomical locations, frequently appears in the retina and conjunctiva, and less commonly in the oral and nasal cavities. Teratoma, a mixed tumor derived from 3 germ layers, predominately occurs in the ovaries or testes, with occasional manifestations in the oral cavity, featuring components such as hair, teeth, and sebaceous glands. Rhabdomyosarcoma, a malignant soft tissue tumor arising in striated muscle tissues, is prevalent in the head and neck, genitourinary system, and limbs, noted for its rapid and invasive growth. Glioma, a tumor of the central nervous system, is rare in the oral cavity but can occur in the tongue, marked by abnormal proliferation of glial cells. Hamartomas are histologically characterized by proliferative salivary glands, smooth muscle, adipose tissue, blood vessels, cartilage, and fibrous tissue,11-13 all consistent with the findings in this case. In a few instances, ganglia 14 and meningeal epithelia 15 were observed. In addition, some patients may present with lesions in other body systems, such as the nervous and digestive systems. 16 Immunohistochemical staining techniques in pathological studies enhance the accuracy of identifying tissue composition. For example, salivary gland tissue typically expresses α-smooth muscle actin, adipose tissue manifests fat stains, and vascular epithelial cells are marked by CD34.8,17 These markers are instrumental in the diagnosis and differential diagnosis. Most patients with tongue hamartoma typically exhibit no pronounced symptoms, allowing for conservative management and regular monitoring for changes. However, for a minority of patients with lesions located at the root of the tongue, in the sublingual area, or those presenting with large volumes that cause dysphagia and dyspnea, surgical resection is recommended.3,15 In the case presented, multiple hamartomas led to feeding difficulties and showed a trend of gradual increase. Consequently, surgical resection was undertaken, restoring the normal morphology of the tongue. No recurrence was observed during a follow-up period of 7 years.
Conclusion
Multiple hamartoma of the tongue is a rare and frequently overlooked congenital benign lesion. For patients with this condition, a multidisciplinary consultation is recommended due to the potential coexistence with systemic dysplasia. When addressing oral lesions, consideration must also be given to systemic development. In addition, long-term follow-up post-surgery is essential to promptly detect and address any potential recurrences.
Footnotes
Author Contributions
Yuelin Qin: Conception and design of the study; Acquisition of data; Data analysis and interpretation; Drafting of the manuscript and critical revision; and Approval of final version of the manuscript.
Ningning Hu: Data analysis and interpretation
Runze Zhang: Acquisition of data
Xuecai Yang: Drafting of the manuscript and critical revision; Approval of final version of the manuscript.
Junwei Wang: Drafting of the manuscript and critical revision and Approval of final version of the manuscript.
Data Availability Statement
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethics Approval
The studies involving human participants were reviewed and approved by the ethics committee of Qingdao Women and Children’s Hospital.
Informed Consent
The patient’s legal guardian provided written informed consent to participate in this study.