
Abstract
Cornelia de Lange syndrome (CdLS) is a rare genetic multiple malformation disorder with many otolaryngologic comorbidities. Patients with CdLS appear to have an increased prevalence of chronic rhinosinusitis (CRS) and chronic rhinosinusitis with nasal polyposis (CRSwNP), however, there is limited literature describing the presentation, evaluation, and management of CRSwNP within the CdLS population. Here we performed a literature review from Embase, PubMed, Cochrane Library, and Google Scholar and reported a case of CRSwNP with concomitant CdLS that was identified at our institution. We describe an 8-year-old male with CdLS and CRSwNP confirmed by history, physical exam, nasal endoscopy, and computed tomography. Symptoms of nasal obstruction were refractory to medical management and required repeat surgical management with improvement in nasal obstruction. Literature review identified 2 additional cases of nasal polyposis with similar management strategies. Additionally, one case series showed 33% of CdLS patients had recurrent sinusitis while a second series identified 39% of CdLS patients with CRS and 12% with CRSwNP. These data suggest that CRSwNP is more prevalent in patients with CdLS compared to the general public and can be both safely and effectively managed with a combination of medical and surgical therapy.
Introduction
Cornelia De Lange syndrome (CdLS) is a genetic multiple malformation syndrome within the family of cohesinopathies characterized by a spectrum of craniofacial, musculoskeletal, gastrointestinal, and neurodevelopmental abnormalities. Despite being first described in 1933, the understanding of this disease entity has been historically poor up until the last few decades due to its rarity with an estimated incidence between 1 in 10,000 to 1 in 100,000 live births. 1 Clinical presentation of CdLS can be highly variable with 7 genes related to chromatin regulation of the cohesion complex implicated in the varying presentations of CdLS, including NIPBL, SMC1A, SMC3, RAD21, HDAC8, ANKRD11, and BRD4.1,2 In classic CdLS, most frequently with NIPBL mutations, there are a range of medical complications with craniofacial anomalies including microcephaly, low anterior hairline, synophrys, long eyelashes, short noses with concave nasal ridge and upturned nasal tip, long or smooth philtrum, thin upper lip vermilion, high arched palate often with cleft, down-turned oral commissures, and micrognathia.1-4
Much of the literature has focused on the implications of genetic variability and early life outcomes, but an assumption of poor life expectancy has pervaded despite many patients living past age 50 with modern medicine. In a population of adults with CdLS, over one-third of the patients were diagnosed with chronic rhinosinusitis (CRS). Surprisingly another third of the CdLS with CRS subgroup were found to have nasal polyposis (NP). 4 The prevalence of CRS is only 2.1% to 10.9% in the general population, with prevalence of chronic rhinosinusitis with nasal polyposis (CRSwNP) affecting up to 4% of the general population. 5 Furthermore, CRSwNP is more commonly described in individuals 40 to 60 years of age and is very rare in children less than 10 years of age.6,7 Despite the high prevalence of CRSwNP and unique sinonasal anatomy of CdLS, there is a paucity of literature on the management of CRSwNP in this population. We present this case report and review of literature to bring attention to this underdiagnosed disease entity, fill this knowledge gap, and provide guidance on diagnosis and treatment.
Methods
Subjects
The electronic medical record was retrospectively reviewed for patients with diagnosed CdLS and CRSwNP from the Weill Cornell Medical Center (WCMC). Chart review identified 1 patient who met criteria. A waiver of informed consent was granted by the Weill Cornell Medical Center IRB as this study was considered to be minimal risk to patients. All ethical guidelines and rules were followed to protect patient privacy. Telephone informed consent was obtained for deidentification and publication of this case report from the individual’s legal guardian and caregiver.
Review of Literature
We conducted a thorough literature review for all instances of CdLS and CRSwNP. We searched Embase, PubMed, Cochrane Library, and Google Scholar using the following keywords: “Cornelia de Lange Syndrome,” “de lange syndrome,” “sinusitis,” “nasal polyps,” “chronic rhinosinusitis,” and “CRSwNP.” Results were limited to those published in English. Abstracts were screened for inclusion of both CdLS and otolaryngologic manifestations prior to complete review.
Case Presentation
This patient first presented to WCMC at birth. He was born at 33 weeks gestation with unremarkable prenatal microarray and subsequent postnatal genetic testing positive for NIPBL mutation. Postnatal history was notable for a submucous cleft palate and failed ABR prompting early intervention with Pediatric Otolaryngology. His remaining medical history was notable for atrial septal defect, bilateral nasolacrimal duct obstruction requiring dacryocystorhinostomy at age 3, gastroesophageal reflux disease (GERD) with esophagitis requiring Nissen fundoplication and gastrostomy tube placement at age 7.
At age 8 the patient presented for follow-up with persistent snoring and nasal congestion, found on nasal endoscopy to have bilateral NP. Symptoms were initially managed medically with systemic antihistamines, intranasal steroid sprays, and intranasal saline sprays with limited effect. A short course of oral steroids provided near-term improvement in nasal congestion and rhinorrhea before recurrence approximately 1 month after completion. Budesonide saline irrigations were attempted but discontinued because of patient intolerance. After 5 months of ineffective medical therapy, the patient was referred to rhinology for surgical management of refractory CRSwNP. Preoperative computed tomography (CT) was obtained showing an opacified rudimentary left frontal sinus, nearly opacified right frontal sinus, bilateral complete ethmoid opacification, bilateral maxillary sinus opacification, and minimally developed sphenoid sinus (Figure 1). The patient subsequently underwent endoscopic sinus surgery (ESS), including bilateral maxillary antrostomies with removal of polypoid tissue, bilateral complete ethmoidectomies, and right frontal sinusotomy with removal of nasal polyps. Initial histopathologic evaluation described typical eosinophilic inflammation and interval outpatient follow-up showed improvement in nasal congestion with the use of daily intranasal steroids and intranasal saline sprays. However, later the patient developed interval polyp regrowth 7 months after primary ESS. He returned for revision ESS and histopathologic evaluation was notable for focal histiocytic inflammation (Supplemental Figure 1). Following the second ESS, the patient had a durable response for 9 months but is again scheduled for a third ESS, allergy evaluation, and possible initiation of immunotherapy.
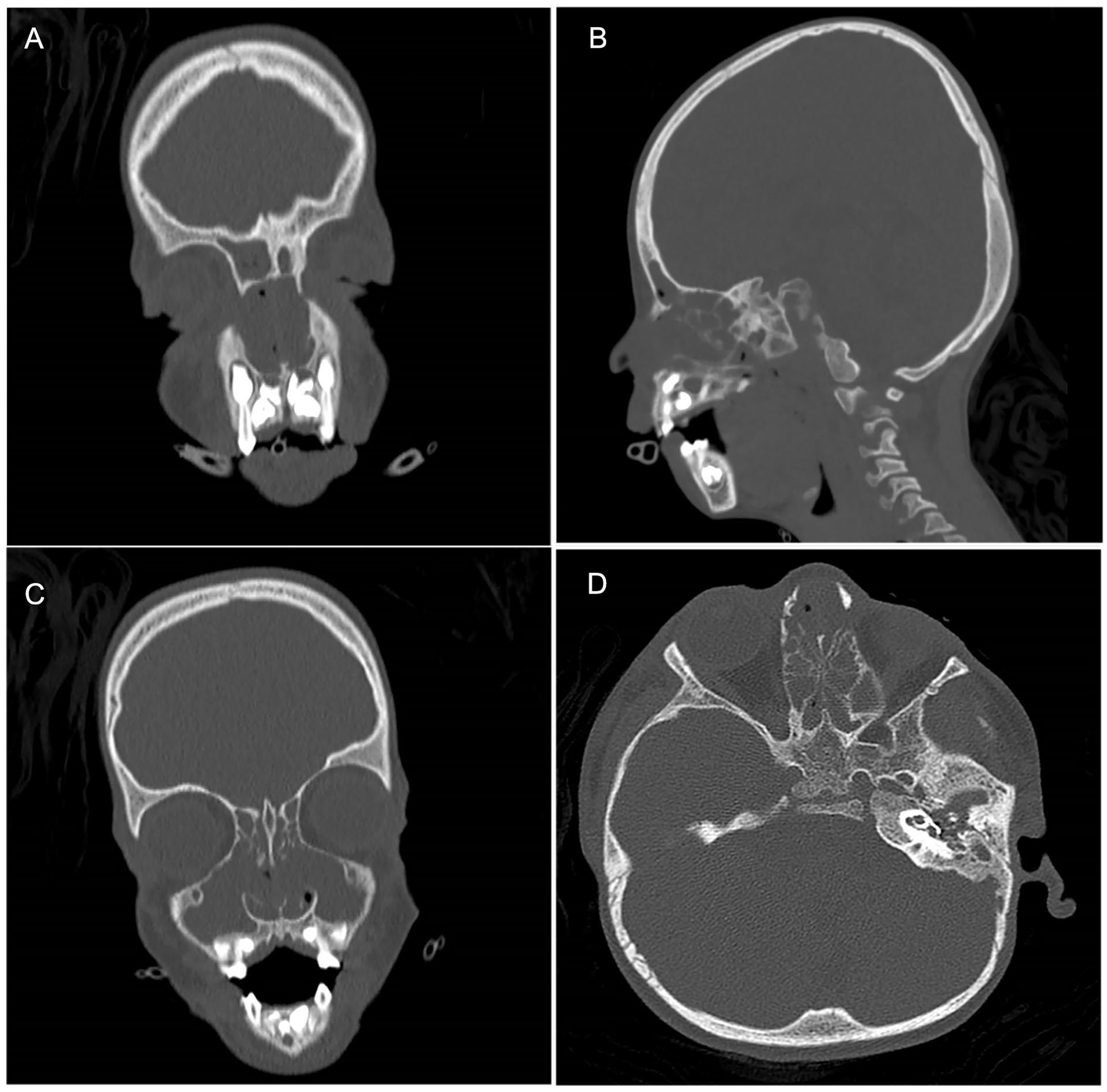
Preoperative radiographic evaluation of CRSwNP. (A) Coronal view of opacified rudimentary left frontal sinus, nearly opacified right frontal sinus. (B) Sagittal view right frontal sinus outflow tract. (C) Coronal view of bilateral maxillary sinus opacification, osteomeatal complex obstruction, and intact lamina papyracea. (D) Axial view of bilateral complete ethmoid opacification.
Review of Literature
Search results identified 204 reports, 201 in total after duplicates were removed. After screening for inclusion of both CdLS and otolaryngologic disease, a total of 15 primary reports, reviews, and book chapters were identified. Of these remaining sources all those citing prior data were excluded, which left 3 reports (Table 1).
Summary of Qualitative Data on CdLS With CRSwNP
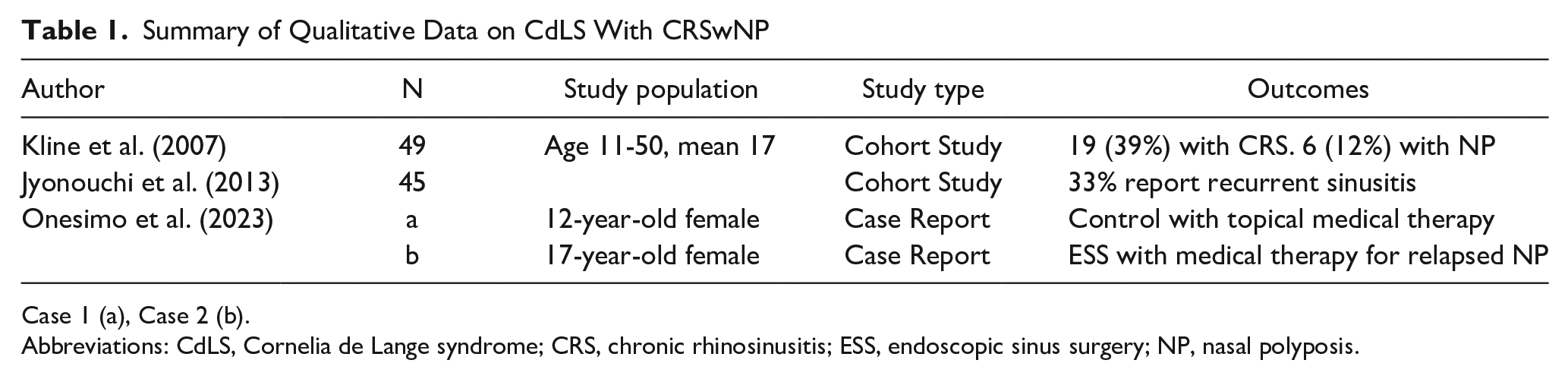
Case 1 (a), Case 2 (b). Abbreviations: CdLS, Cornelia de Lange syndrome; CRS, chronic rhinosinusitis; ESS, endoscopic sinus surgery; NP, nasal polyposis.
The first case series included 49 CdLS patients aged 11-50 and 39% of this cohort was diagnosed with CRS and 12%, or one-third of all CRS patients, with CRSwNP. 4 The second series included 45 CdLS patients and reported that 33% of their cohort had recurrent sinus infections. 8 The third report described two case reports of CdLS patients with CRSwNP as described below.
The first case described a female patient diagnosed with classic, NIPBL mutant, CdLS at 5 years of age. Her medical history was significant for GERD requiring Nissen fundoplication and obstructive sleep apnea (OSA) treated with continuous positive airway pressure (CPAP) therapy. At 12 years of age, the patient noted significant nasal congestion and worsening sleep prompting nasal endoscopy, which revealed a unilateral right-sided nasal polyp in the middle meatus. This was treated with nasal steroid sprays for 6 months with reported improvement in sleep quality and without relapse of polyps at 2 years. 9
The second case described was of a female patient diagnosed with CdLS at 1 year of age. Medical history was notable for GERD treated with proton pump inhibitor therapy, recurrent nasal obstruction, and OSA diagnosed at age 6. This patient was treated with CPAP until worsening nasal obstruction at age 17 when she was found to have endoscopic and radiographic evidence of unilateral polyposis consistent with CRSwNP. This patient was treated with ESS, recurrence was noted 1 year after surgery. Recurrence was treated with nasal steroid therapy with resolution of polyposis on nasal endoscopy. 9
Discussion
CdLS is a rare genetic syndrome characterized by distinctive facial and musculoskeletal malformations associated with numerous medical comorbidities that require multidisciplinary management. 2 Associations between CdLS and otolaryngologic disease have been documented, but have largely focused on the immediate sequelae of aerodigestive and otologic complications at birth and early childhood.10-13 Due to concerns about the life expectancy of CdLS patients, many manifestations of the disease have been historically neglected, including CRS, which is estimated to affect 39% of patients, with 12% of the total population having CRSwNP.1,4 As these patients are now understood to live well into adulthood, it is clear that proactive management of sinonasal disease when present can dramatically impact the quality of life. 14 By reporting on our experience and review of the literature, we seek to demonstrate that workup, including nasal endoscopy and treatment with sinus surgery and postoperative nasal debridement are safe and effective in this patient population.
The patient presented here had regularly scheduled otolaryngologic care shortly after birth. This allowed for comprehensive history, physical exam, and early recognition of NP with in-office nasal endoscopy. This guided the first stage of treatment, which involved medical management with topical steroids. After failure of medical therapy CT imaging was obtained, which corroborated these findings and provided information for surgical planning. Similar to other patients with CRSwNP, the reported approach included an initial trial of medical management with consideration of ESS if medication alone was ineffective to control the disease burden.7,15,16 Of the three patients reported, two met criteria for CRSwNP and went on to require ESS. Medical management was sufficient for one patient with isolated unilateral NP in setting of worsening sleep quality secondary to nasal obstruction.
Patients with CdLS and suspected CRSwNP should be evaluated by an otolaryngologist. Due to the nonroutine nature of this disease, increased consideration toward treatment with a rhinology subspecialist may be warranted. Workups, including nasal endoscopy and CT, are safe and important to treatment planning. An initial trial of medical management, including topical steroids, is recommended. This reinforces similar findings from the other two patients reported in literature.
For patients who do not respond to medical management, ESS is recommended. The goal of this is to decrease polyp burden and open the sinuses to allow both for egress of mucous and ingress of topical medication. 15 Because patients with congenital abnormalities can have anatomic variants that elevate risk to critical structures, including the skull base and orbit during ESS, it is important to understand the special considerations when performing surgery in this population. Our experience demonstrates normal relationships between structures in the nose and sinuses (Figure 1). However, the cross-sectional area of the nasal cavity was decreased compared to the norm for similarly aged patients, leading to increased challenges with instrumentation. Despite this technical challenge, comprehensive and thorough surgery was safe and successful with symptomatic improvement.
As there is a lack of prior reports on CdLS patients undergoing surgery for CRSwNP, consideration should be given to atypical inflammatory processes, particularly in patients with recalcitrant disease. The patient presented here had evidence of histiocytosis on NP histopathology and no evidence of a systemic histiocytic disease, such as Langerhans cell histiocytosis. Immunologic evaluation of individuals diagnosed with CdLS showed an increased frequency of antibody deficiency with a decrease of T regulatory cells and T follicular helper cells. 8 Previous hypotheses on the pathogenesis of sinusitis and/or NP in CdLS have postulated inflammatory changes secondary to GERD alter the midfacial development and health of the sinonasal mucosa; however, the question of whether there is any contribution from dysregulation of the immune system leading to CRSwNP in CdLS requires further investigation.9,17
This study has a few key limitations, including inherent weaknesses associated with reporting a small case series on a rare condition. Due to the small sample size, it is impossible to draw statistically backed conclusions generalizable to the overall population of patients with this disease. These cases warrant attention despite this due to the paucity of literature on this underappreciated entity. Future higher-powered studies are needed to better understand the link between these conditions to allow for early recognition and management of NP in this population.
Conclusion
Comprehensive otolaryngologic evaluation and treatment of patients with CdLS should include a high index of suspicion for CRSwNP. The existing evidence suggests that nasal endoscopy, medical management with topical steroids, and ESS are safe and effective interventions in CdLS patients with CRSwNP. Further reports of management considerations for CRSwNP in this unique patient population are warranted.
Supplemental Material
sj-tiff-1-ear-10.1177_01455613241284153 – Supplemental material for Management of Nasal Polyposis in Pediatric Patients With Cornelia de Lange Syndrome: A Case Series and Literature Review
Supplemental material, sj-tiff-1-ear-10.1177_01455613241284153 for Management of Nasal Polyposis in Pediatric Patients With Cornelia de Lange Syndrome: A Case Series and Literature Review by Ian F. Caplan, Michael Ye and Aaron N. Pearlman in Ear, Nose & Throat Journal
Footnotes
Author Contributions
A.N.P. was responsible for the conception of the presented project. A.N.P. and M.Y. were responsible for the clinical care of the patient described in this case report. I.F.C. was responsible for the literature review. I.F.C. took the lead in writing the manuscript with critical feedback provided by all authors.
Data Availability
Not applicable.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Considerations
A waiver of informed consent was granted by the Weill Cornell Medical Center IRB as this study was considered to be minimal risk to patients. All ethical guidelines and rules were followed to protect patient privacy.
Consent to Participate
Not applicable.
Consent for Publication
Telephone informed consent was obtained for deidentification and publication of this case report from the individual’s legal guardian and caregiver.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.