
Abstract
Introduction
Laryngeal cancer is a common head and neck tumor that usually originates from the laryngeal mucosa.1,2 Radiotherapy and other methods are widely used to preserve laryngeal function, but total laryngectomy (TL) becomes an ultimately effective therapeutic option when laryngeal cancer is at an advanced stage or other treatments have failed. 3 Unfortunately, TL is a complex procedure involving complete resection of the larynx, and the most common complication after TL is pharyngeal fistula (PF), 4 which has a prevalence rate of between 21% and 58%, 5 and may lead to severe infections, greatly prolonging the patient’s hospital stay and potentially delaying follow-up, which poses a physiological, psychological, and social significant challenges.
A study by Matsumoto et al 6 indicated that poor postoperative healing condition of the pharyngeal mucosal suture may be a precursor to the development of PF, on the other hand, if the mucosal suture is too tight, it can cause localized ischemic necrosis, which is also a risk factor for PF formation. 5 Therefore, postoperative pharyngeal mucosal closure is a critical step in TL, and its quality and choice of technique directly affect the patient’s postoperative recovery and functional reconstruction. Different pharyngeal mucosal closure techniques, such as hand sutures, linear suture devices, 7 and thyroid gland flap (TGF), 8 have been used in attempts to restore the integrity and function of the pharyngeal mucosa. It has been stated that the use of linear suture reduces the operative time and decreases the rate of PF formation compared to the traditional manual suturing technique. 9 TGF is an innovative technique for pharyngeal mucosal closure. 10 It was first introduced into 5 cases of vertical partial laryngectomy in 1990 (dissection and use of part of the upper pole according to the size of the defect). 11 At the last follow-up, all 5 flaps survived, with abundant TGF blood supply and less shrinkage than other flaps. It was also found that the length of the vascular pedicle of the superior thyroid artery (STA) made it easy for TGF to rotate and be used for laryngeal reconstruction. 11 This technique involves the use of partial thyroid tissue grafts to cover the defect area of the pharyngeal mucosa, which has the advantages of restoring the integrity of the pharyngeal mucosa and reducing postoperative complications while preserving thyroid tissue and related functions. 12 Several studies have shown that increased vascularized tissue reduces the overall rate of fistulas and fistulas requiring reoperation. 13 Flaps may reduce the incidence of PF or shorten the healing time of PF. Song et al 12 showed that TGF is an effective and reliable flap that can be used as a method for the reconstruction of the neopharynx. Our previous study14,15 also described the application of TGF in TL, and the results suggested that TGF can be used to repair neck defects when selective and appropriate, and its advantage of preserving upper pole vessels can be safely used for mucosal decompression after TL.
In clinical practice, physicians are faced with the dilemma of choosing between different pharyngeal mucosal closure techniques and lack sufficient scientific evidence to support their decisions. The aim of this study was to compare the clinical outcomes of 3 different pharyngeal mucosal closure techniques, namely, hand suture, linear suture device, and TGF, after TL through retrospective analysis. The results of the study will provide physicians with more comprehensive and accurate information to make informed decisions during surgery and provide better patient outcomes and postoperative rehabilitation.
Patients and Methods
Clinical Data
Collect data from laryngeal cancer patients hospitalized in a single center and treated with surgery from January 1, 2018, to December 1, 2021. The screening was performed according to the following inclusion and exclusion criteria.
Inclusion criteria: (1) Patients diagnosed with laryngeal squamous cell carcinoma who require undergoing TL; (2) Individuals in whom manual suture, linear suture device, or thyroid flap techniques were employed for closure; (3) Patients presenting with cervical lymph node metastasis; and (4) Participants who have provided their informed consent by signing the corresponding form.
Exclusion criteria: (1) Patients who had received radiotherapy, chemotherapy, or targeted therapy within one month prior to surgery, or who presented with distant metastasis. (2) The presence of any additional primary malignant tumors, excluding head and neck tumors. (3) Concurrent poorly controlled diseases, such as heart failure, diabetes, hypertension, thyroid disorders, or psychiatric conditions, in the patients. (4) Patients who had undergone other types of flap reconstruction, including pectoralis major myocutaneous flap or free flap procedures.
Grouping criteria: Grouping criteria were based on the distinct methods employed for closing the pharynx following TL. Patients were categorized into 3 distinct groups: Group A comprised those who underwent manual Y-shaped suture closure, group B included those who received linear stapler closure, and group C consisted of patients who underwent TGF closure. Comprehensive sociodemographic data, disease characteristics, surgical details, and follow-up information were systematically collected for all patients in these 3 groups to ensure a comprehensive comparison across the different closure techniques.
Operational Approach
In cases where necessary, based on the extent of cervical lymph node metastasis and other clinical factors, a neck lymph node dissection may be performed simultaneously during TL (ie, In case of suspicious or confirmed cervical lymph node metastasis, neck lymph node dissection could be performed according to the situation. This series is based on elective neck dissection, accessory nerve, internal jugular vein, and sternocleidomastoid muscle can be retained. Lymph node dissection in regions II, III, IV, V, and VI could be performed according to the situation.). According to the scope of tumor invasion, some patients in group A and group C underwent partial hypopharyngeal resection along with TL. Tracheostomy and other management were treated with a routine procedure under general anesthesia in supine position. Therefore, the following only introduces the relevant operation steps for pharyngeal mucosa closure in each group.
Group A: A classic laryngectomy was performed followed by a manual Y-shaped suture of the residual pharyngeal mucosa. For the mucosal closure of the pharyngeal cavity, a two-layer closure technique was utilized. First, the mucosal layer was sutured using 3-0 absorbable Vicryl sutures with interrupted stitches, typically requiring approximately 15 to 20 knots. This was followed by the closure of the soft tissue layer with 2-0 Vicryl sutures, using continuous sutures. Finally, the muscle layer was closed with 2-0 Vicryl sutures, followed by subcutaneous tissue closure with 3-0 Vicryl sutures, and the skin was sutured using 4-0 nonabsorbable nylon sutures with interrupted stitches, ensuring a secure and layered closure to promote optimal healing and minimize the risk of complications.
Group B: The tumor had no hypopharyngeal invasion and no pharyngectomy was performed. The hyoid bone and the thyroid horn were removed, the pharyngeal retractor attached to the outer edge of the thyroid plate was removed, the sublaryngeal trachea was cut, and the membrane was carefully separated upward to the level of the cricoid cartilage. A small incision was made at the upper edge of the thyroid cartilage, and Alice forceps entered from the end of the trachea under the larynx, assisted in holding the free edge of the epiglottis through the small incision, and the epiglottis was pulled down into the laryngeal cavity. After pulling the laryngeal body forward, the linear stapler (linear cutter GCLUC-75, 75 mm; JiangSu GuanChuang Medical Technology Co., Ltd.) was applied horizontally on the upper and lower sides of the soft tissue on the dorsal aspect of the laryngeal body for cutting and closure (Figure 1). After cutting and closing with linear stapler, the soft tissue layer was sutured, followed by muscle, subcutaneous, and skin sutures, all with interrupted sutures.
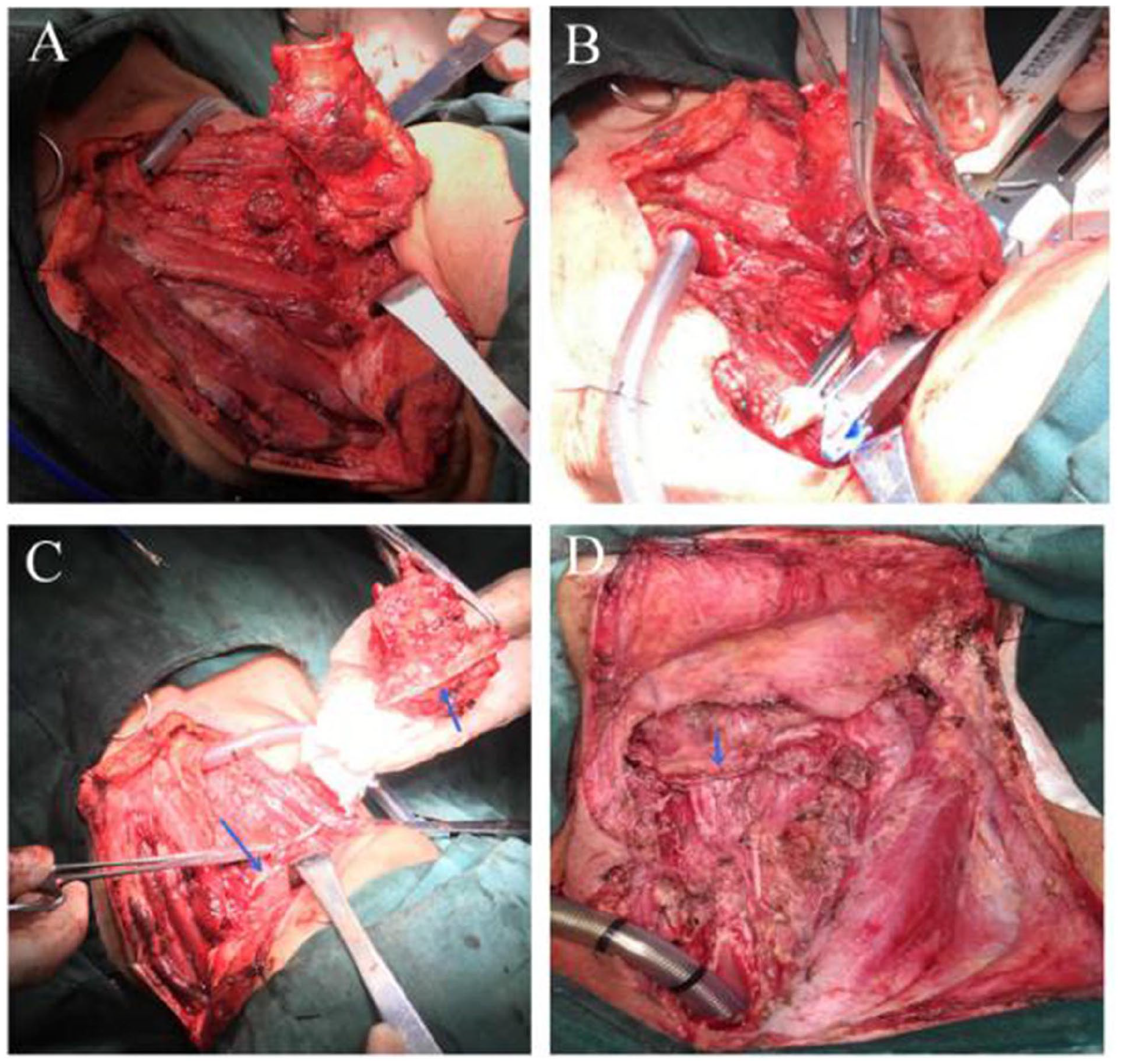
The operation of linear stapler group. (A) After Alice forceps clamp the free edge of epiglottis through the small incision assistant, the epiglottis was pulled down into the laryngeal cavity. (B) Free the dorsal tissue of the laryngeal body to the level of the dorsal side of the arytenoid cartilage, ensuring the tissue thickness suitable for placement using a linear stapler. (C) Using a linear stapler to complete the cutting and closure. Blue arrow: Closure line. (D) The horizontal cutting and closure. Blue arrow: Closure line.
Group C: A classic laryngectomy was performed. Semi-Y-shaped manual suture of the residual pharyngeal mucosa. The ipsilateral superior thyroid vessels were preserved as the vascular pedicle. If it is necessary to obtain a freer vascular tibia, the branches along the STA and vein may be incised and ligated. Then the unilateral glandular lobe was disconnected from the isthmus and separated. The TGF was rotated upward and inserted into the pharyngeal mucosal defect. The dorsal side of the gland faces inward and serves as a part of lining for the neo-pharyngeal cavity. The surrounding edge of the gland is sutured with the residual pharyngeal mucosa margin to close the pharyngeal cavity (Figure 2). When the pharyngeal mucosa was closed, the peripheral mucosal layer was sutured first, the mucosal defect was sutured with the edge of TGF, the soft tissue layer was sutured in the third step, and the muscle, subcutaneous, and skin were sutured finally.
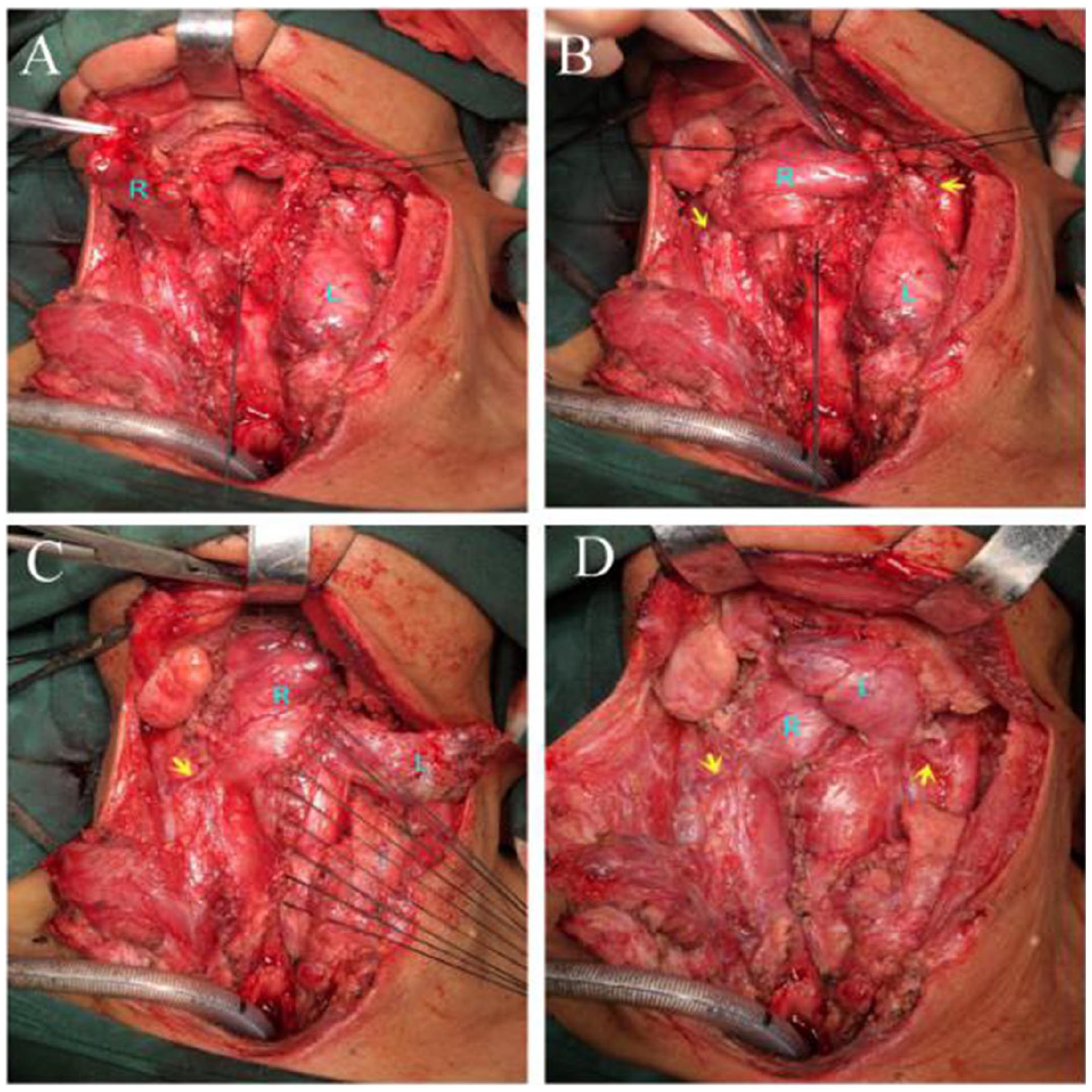
The operation of TGF group. (A) Semi-Y-shaped manual suture part of the residual pharyngeal mucosa after TL. The TGF on the right is lifted. R: Right TGF, L: Left thyroid gland. (B) TGF was lifted and rotated upward (R: right TGF, L: left TGF, yellow arrow: TGF pedicle vessels). (C) TGF inserted into the pharyngeal mucosal defect and sutured with surrounding residual tissue (R: Right TGF, L: left TGF, yellow arrow: TGF pedicle vessels). (D) Right TGF insert + left TGF overlap repair (R: right TGF, L: left TGF, yellow arrow: TGF pedicle vessels). TGF, thyroid gland flap.
Voice prosthesis insertion was not performed in all 3 groups. Gastric tube removal in the 3 groups was performed according to the following criteria: for patients without PF, gastric tube removal was performed in 10 to 14 days; for patients with PF, the time of gastric tube removal was determined according to wound healing.
Statistical Analysis
After collecting relevant indicators, the data were analyzed using IBM SPSS 26 statistical software. The description of quantitative indicators was shown with mean ± standard deviation, and the classification indicators were described as the number and percentage of various types. The Chi-square test was used in the univariate analysis. The length of stay, cost, operation time, and laboratory results among the groups were analyzed by T-test. P < .05 was statistically significant.
Results
The general information of patients is shown in Table 1. A total of 81 patients who underwent TL due to laryngeal cancer were collected in this study based on the inclusion and exclusion criteria, with a mean age of 64.09 ± 9.20 years. Notably, no statistically significant differences were observed in age, stature, body weight, or body mass index among the 3 distinct groups (P >.05), thereby ensuring the reliability of our study. The tumor stage and primary tumor location of the patients were shown in Table 2, and there were significant differences in the distribution of tumor stage and primary tumor location among the 3 groups (P = .002 and P < .001, respectively). In addition, there were no significant differences among the 3 groups in length of hospital stay, total cost, preoperative and postoperative leukocytes, hemoglobin, neutrophils, lymphocytes, total protein and albumin (P > .05), but it is worth noting that the total operation time of group B was significantly shorter than that of the other 2 groups (P = .006), and its total cost was slightly lower than that of the other 2 groups (Table 3). In terms of the incidence of PF, 14 of all cases had PF, and the incidence of PF was 17.28% (14/81), among which the incidence of PF was 12.35% (10/50) in group A, 12.5% (2/16) in group B, and 13.3% (2/15) in group c (Table 3). The rate of PF did not differ significantly among the 3 groups, and there were no complications of dysphagia observed in any of them (So far, during the follow-up period of 2 to 5 years in this series, no patients have complained of dysphagia.). In addition, Table 4 also showed that there was no significant difference in blood calcium level and thyroid function indicators between the 3 groups before and after surgery (P > .05).
Patient General Data.

Y: Years, representing the age of the patients in years. cm: Centimeters, indicating the height of the patients in centimeters. kg: kilograms, representing the weight of the patients in kilograms.
P < .05 indicated that the difference was statistically significant.
Primary Cancer Stage and Primary Tumor Location.

P < .05 indicated that the difference was statistically significant.
Preoperative and Postoperative Clinical Data of Patients.

Total cost encompassed surgical instruments/materials expenses, anesthesia and OR time efficiency, postoperative care costs (hospitalization, medications, rehabilitation), complication rates and treatment expenses (especially pharyngocutaneous fistula with linear suturing), and follow-up/miscellaneous expenses.
P < .05 indicated that the difference was statistically significant.
Comparison of Blood Calcium Level and Thyroid Function Indicators Between the 3 Groups.

P < .05 indicated that the difference was statistically significant.
Ca2+: blood calcium (reference range: 2.1-2.6 mmol/L). T3: free triiodothyronine (reference range: 3.1-6.8 pmol/L). T4: free tetraiodothyronine (reference range: 12-22 pmol/L). TSH: thyrotropin-releasing hormone (reference range: 0.27-4.2 mIU/L).
In group A, 2 patients with laryngeal tumor invading thyroid gland underwent thyroidectomy, and Thyroxine was taken after operation, which was excluded.
In group B, a patient underwent a follow-up examination of blood calcium and thyroid function after surgery in another hospital, which was excluded due to differences in the reference range.
Discussion
To evaluate the effectiveness of various pharyngeal closure techniques in patients undergoing TL for laryngeal cancer and their impact on postoperative complications, particularly PF, a common complication of TL, 16 a review was conducted on 81 patients who had undergone the procedure. TL is a major surgical intervention for advanced laryngeal cancer, 17 and the choice of closure technique is crucial for optimal outcomes. By comparing different methods, the study seeks to provide insights that inform clinical decisions, enhance surgical practices, and improve patient recovery. Understanding which techniques best prevent PF and other complications will guide surgeons in selecting appropriate methods, ultimately improving prognosis and quality of life for laryngeal cancer patients.
PF is a common complication of TL, with an incidence rate of 3% to 65% due to marginal vascular damage, as reported in recent studies. 5 PF increases infection risk, prolongs hospital stay, delays recovery, causes nutritional issues, reduces quality of life, and raises medical costs. 18 TGF is an innovative pharyngeal mucosal closure technique 19 that provides additional mucosal tissue, enhancing the feasibility and quality of pharyngeal closure. 12 This approach effectively prevents PF. Therefore, we focused on the incidence rate of PF among the 3 different closure techniques. The present study reported a PF rate of 17.28% (14/81) across all cases, with no significant difference in rates between the 3 groups. This suggests that all 3 techniques are fairly safe in terms of the occurrence of PF. Song et al 12 stated that the incidence of PF after TL was 21.1%, which was slightly higher than our results, which may be due to differences in surgeon’s skill and experience. Pharyngeal mucosal defects can also be repaired with TGF insertion + overlap to strengthen it (Figure 2D), which can be used as a pedicled flap for small-scale head and neck defects. Notably, there were no complications of dysphagia in all 3 groups, which is an encouraging finding. For patients undergoing TL, preserving the ability to swallow is essential to maintaining their overall quality of life. The absence of dysphagia complications underscores the success of these closure techniques in restoring or preserving swallowing function. However, the absence of dysphagia complications should be interpreted with caution, as the study may have been limited by the sample size or other unmeasured factors. In addition, the lack of differences in blood calcium levels and thyroid function indicators before and after surgery among the 3 groups suggests that the different pharyngeal closure techniques do not adversely affect these physiological parameters. This contributes to the patients’ rapid postoperative recovery.
This study found significant differences in the distribution of tumor stages and primary tumor locations among the 3 groups, likely due to the differing applicability of the 3 closure techniques. It is well known that manual suturing has a wide range of applicability. However, linear staplers are limited to tumors confined to the larynx and not extensively invading other areas.20,21 They are not suitable for complex tumors involving the thyroid cartilage or extending beyond the larynx. 22 Excessive suture tension and mucosal defects in the residual mucosa are significant contributors to the development of PF. 18 Flap repair is the most commonly employed strategy to prevent PF, as it provides additional vascularized tissue to support healing and reduce tension on the sutures, 23 and is crucial for the patient’s long-term health and postoperative recovery. The differences in these closure techniques likely explain the observed variations in tumor staging and primary tumor locations.
In this study, we found that using a linear stapler for pharyngeal closure in TL resulted in lower surgery time and costs compared to manual suturing and TGF techniques. Sofferman and Voronetsky 24 compared the time required for manual suturing and stapler closure, discovering that the use of a stapler indeed shortened the surgical time, which is consistent with our current study findings. The TGF procedure involves harvesting and transplanting thyroid tissue to prevent pharyngocutaneous fistula after TL. 12 The TGF procedure incurs higher costs due to its complexity, additional surgical steps, and need for more instruments and postoperative care resources. However, it results in the shortest hospitalization time, likely due to effective healing from well-vascularized tissue, reduced postoperative complications, and stable surgical outcomes. 12 These findings suggest that while linear staplers are cost-effective for quicker surgeries, TGFs, despite higher initial costs, offer faster recovery and potentially lower long-term healthcare costs, and improving patient outcomes.
It is important to acknowledge some limitations of this study. As a retrospective analysis, inherent biases and confounding variables may have influenced the results. The relatively small sample size could have restricted the statistical power to detect subtle differences among the groups. Additionally, the lack of long-term follow-up data limits the understanding of late complications associated with different closure techniques.
Conclusions
TGF is a safe option that can be used to repair mucosal defects and close the pharyngeal cavity after TL surgery, but in the absence of mucosal defects and widespread tumor invasion, linear staplers are the most time-efficient method. However, the choice of closure technique should be carefully considered and a multidisciplinary collaborative approach should be adopted, taking into account individual patient factors and surgical expertise. Larger prospective studies are needed to further strengthen the evidence base and provide clinical decisions for optimal patient outcomes.
Footnotes
Author Contributions
Guarantor of integrity of the entire study: Jixiang Wu and Zhengxue Han; Study concepts: Zhengxue Han, Jixiang Wu, and Jugao Fang; Study design: Jixiang Wu, Zhengxue Han, and LiZhen Hou; Definition of intellectual content: Jixiang Wu; Literature research: Bo Han; Clinical studies: Bo Han; Experimental studies: Jixiang Wu and Jugao Fang; Data acquisition: Sen Hao; Data analysis: Bo Han; Statistical analysis: Bo Han; Manuscript preparation: Bo Han and LiZhen Hou; Manuscript editing: Jugao Fang; Manuscript review: Jixiang Wu.
Data Availability
The simulation experiment data used to support the findings of this study are available from the corresponding author upon request.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by the 2022 Inner Mongolia Health Science and Technology Plan Project, Project No.: 202202287.
Ethical Approval
This meta-analysis is approved by the Ethics Committee of Beijing Tongren Hospital, Capital Medical University, and the need for informed patient consent for inclusion was waived.