
Abstract
Introduction
Nasopharyngeal carcinoma (NPC) is a malignant tumor originating from the nasopharyngeal epithelium, displaying notable geographical and ethnic variations in incidence and clinical behavior. In China, particularly in select southern provinces, NPC ranks among the top ten cancers, with an annual rate surpassing 25 per 100,000 population.1,2 Contrastingly, in the United States, NPC is relatively rare, with an annual incidence of 0.17 to 0.56 per 100,000, comprising approximately 0.08% of all malignancies.3,4 Approximately 64,165 patients were diagnosed in China and 1933 patients were diagnosed in the United States in 2022. 3 Histologically, NPC can be categorized into 3 subtypes: keratinizing squamous cell carcinoma (KSCC), differentiated non-keratinizing squamous cell carcinoma (DNKCC), and undifferentiated non-keratinizing squamous cell carcinoma (UNKCC), with varying distribution among different racial/ethnic groups.5-14 Chinese population exhibits a higher prevalence of UNKCC compared to White and African American patients, while KSCC is more common in the latter.
Existing studies have explored the impact of race/ethnicity on NPC survival, largely comparing Asian patients to other races/ethnicities.5-10 However, there were limited studies on specific Chinese populations, and these studies were primarily based on outdated data, failing to capture contemporary treatment paradigms.11-14 Recent shifts in lifestyle and NPC management have potentially influenced the disease’s epidemiology.15-18 Nonetheless, relative to other Asian ethnic groups, Chinese Americans exhibit a higher NPC incidence.12,19 The burgeoning Chinese immigrant population in the United States offers a unique opportunity to examine the histology distribution, tumor staging, and outcomes across diverse racial/ethnic groups impacted by NPC.20-22 Therefore, this study aimed to investigate and compare the distribution of histological subtypes, stage at presentation, and survival outcomes among Chinese American, Non-Hispanic White, and African American patients with NPC using data from the Surveillance, Epidemiology, and End Results (SEER) program.
Methods
Patients
The data were sourced from the 17 population-based cancer registries included in the SEER November 2022 submission. 23 We identified patients with NPC diagnosed between 2010 and 2017. The inclusion criteria for the analysis were: (1) a pathological diagnosis of primary NPC; (2) stage T1-4N0-3M0 disease according to the seventh edition of the American Joint Committee on Cancer (AJCC) NPC staging system; (3) KSCC, DNKCC, or UNKCC subtypes; (4) receipt of beam irradiation with or without chemotherapy. Patients without a positive pathological diagnosis or who did not receive beam irradiation were excluded. Since the SEER program contains only anonymized data, our study was exempted from the approval process by the ethics committee. Additionally, we also included a cohort of Chinese patients with NPC from the First Affiliated Hospital of Xiamen University to compare the patient characteristics between Chinese Americans in the SEER database and patients in mainland China. This cohort included patients with stage T1-4N0-3M0 NPC diagnosed between January 2013 and December 2021 according to the eighth edition of the AJCC staging system. The study was conducted in accordance with the Declaration of Helsinki (as revised in 2013).
Variables
The following variables were extracted from the database: age, gender, histological subtype, tumor (T) stage, nodal (N) stage, chemotherapy, race, survival time, cause of death, and vital status. Histology was categorized into three types: KSCC (codes 8070 and 8071), DNKCC (codes 8072 and 8073), and UNKCC (codes 8020, 8021, and 8082). Racial groups were classified as Non-Hispanic White, African American, or Chinese American. In the cohort of Chinese patients with NPC from the First Affiliated Hospital of Xiamen University, the following variables were included: age, gender, histology, clinical stage, T stage, N stage, and chemotherapy. The primary endpoints of this study were NPC-specific survival (NPCSS) and overall survival (OS). NPCSS was calculated as the date from NPC diagnosis to death specifically from NPC. OS was defined as the time from NPC diagnosis to death from any cause.
Statistical Analysis
Chi-square test was performed to compare statistical significance among racial groups. Propensity score matching (PSM) was employed to mitigate the effects of bias and confounding variables, enhancing comparability between groups. 24 We used 1:1 PSM to control for biases inherent in cohort studies, including variables such as age, gender, histology, T stage, N stage, and chemotherapy. Kaplan-Meier analysis was conducted to estimate survival rates among racial groups, with statistical significance determined by the log-rank test. Multivariate Cox proportional hazard models were constructed to identify independent factors associated with NPCSS and OS. Statistical analyses were performed using SPSS software (version 25.0, IBM Corporation, Armonk, NY, USA), with significance set at P < .05.
Results
Patient Characteristics
We included 1646 eligible patients with NPC from the SEER database (Figure 1). Among them, 1049 (63.7%) were Non-Hispanic White, 332 (20.2%) were African Americans, and 332 (20.2%) were Chinese Americans (Table 1). Of all patients, 1178 (71.6%) were men and 1120 (68.0%) had stage III to IV disease. The KSCC subtype was recorded in 739 patients (44.9%), the DNKCC subtype in 565 patients (34.3%), and the UNKCC subtype in 342 patients (20.8%). The highest incidence of the disease occurred in patients aged 50-59 years (Figure 2; Non-Hispanic White: 29.0%; Americans: 26.8%; Americans: 31.3%). However, regarding median age at NPC diagnosis, Chinese American patients were the youngest. The median age at diagnosis of NPC was 59, 55, and 53 years for Non-Hispanic White, African American, and Chinese American patients, respectively (P < .001).
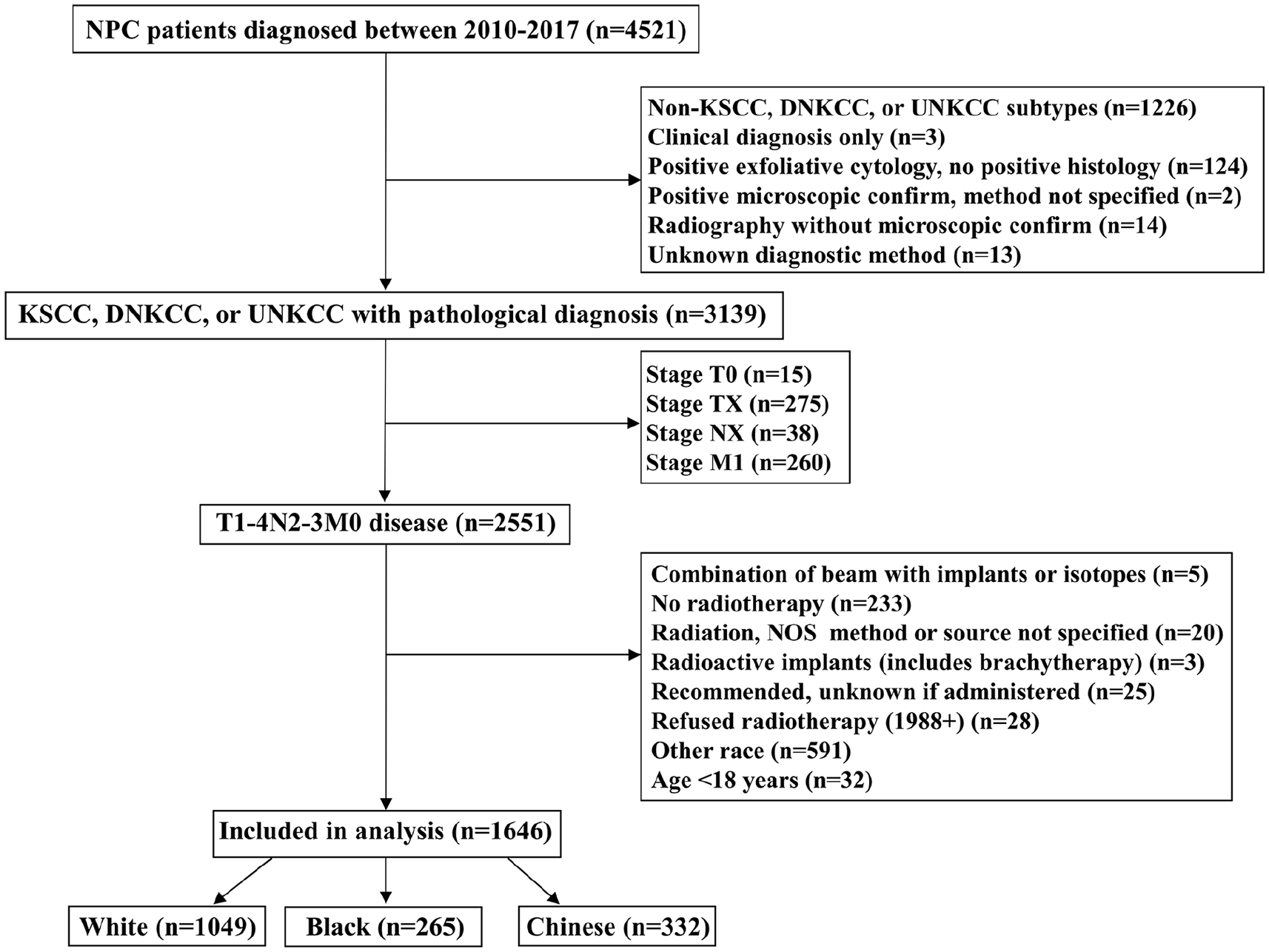
The flowchart of this cohort selection.
Patient Baseline Characteristics.
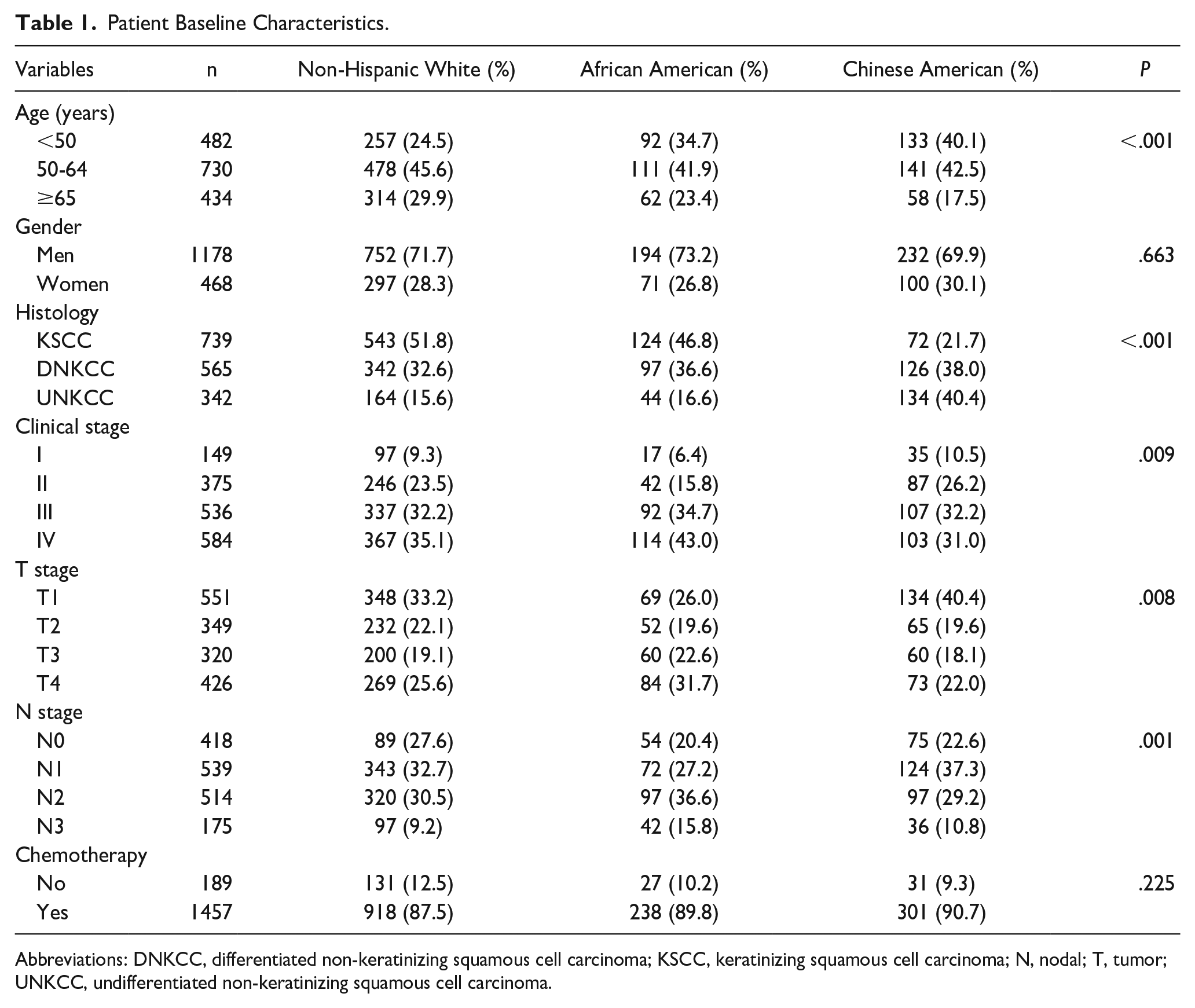
Abbreviations: DNKCC, differentiated non-keratinizing squamous cell carcinoma; KSCC, keratinizing squamous cell carcinoma; N, nodal; T, tumor; UNKCC, undifferentiated non-keratinizing squamous cell carcinoma.
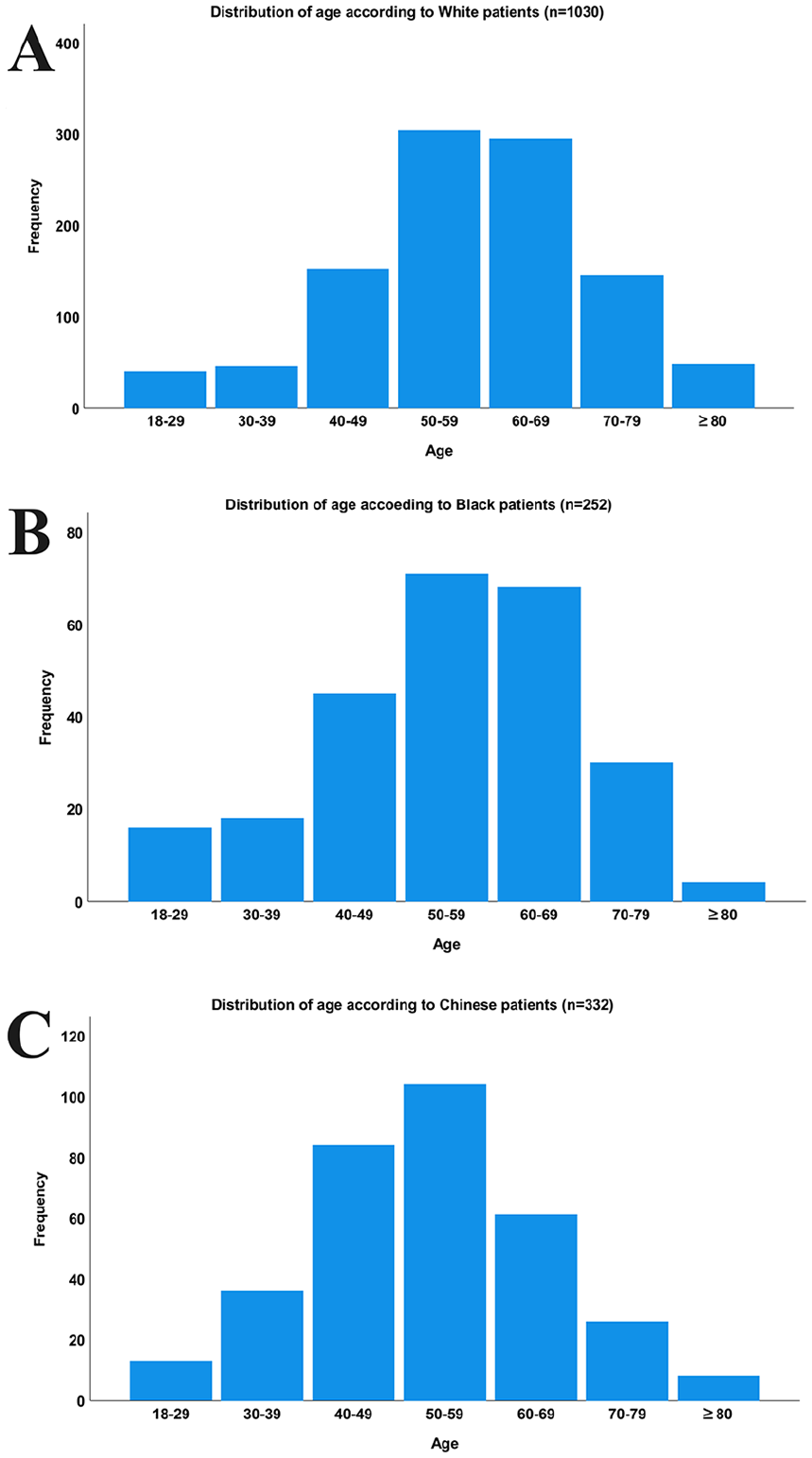
Histograms depicting age distribution according to race in nasopharyngeal carcinoma.
The Effect of Race on Histology Distribution
The distribution of histological subtypes showed significant racial differences (Figure 3). Chinese Americans more frequently had the UNKCC subtype (n = 134, 40.4%) compared to Non-Hispanic White (n = 164, 15.6%) or African American patients (n = 44, 16.6%) (P < .001). However, Chinese American patients had the lowest rate of the KSCC subtype (n = 72, 21.7%) compared to Non-Hispanic White (n = 543, 51.8%) and African American patients (n = 124, 46.8%) (P < .001). There was no significant difference in histological subtype distribution between Non-Hispanic White and African American patients (P = .338).
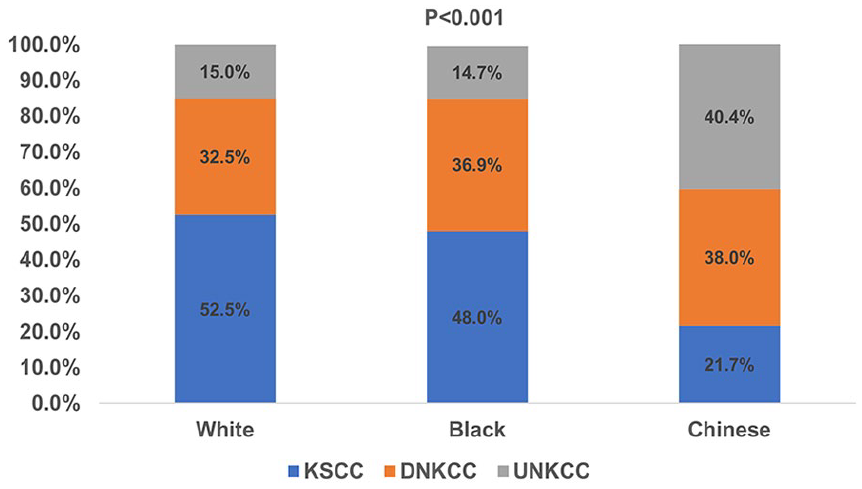
The histological subtype distribution according to race in nasopharyngeal carcinoma.
The Effect of Race on Stage Distribution
We first analyzed the effect of race on stage at presentation in the entire cohort (Figure 4A). African American patients showed the highest rate of stage III to IV disease (n = 206, 77.7%) compared to Non-Hispanic White (n = 704, 67.1%) and Chinese American (n = 210, 63.2%) patients (P = .009). No significant difference was found between Chinese American and Non-Hispanic White patients in terms of stage distribution (P = .494). In the second analysis, we examined the effect of race on stage distribution according to histological subtypes. In the KSCC subtype, there were no significant differences in stage distribution among the three race groups (P = .314; Figure 4B). Conversely, in the DNKCC subtype, African American patients exhibited lower rates of stage I disease (5.2%) but significantly higher rates of stage IV disease (44.3%) compared to Non-Hispanic White (10.8% and 34.2% for stage I and stage IV diseases, respectively) and Chinese American patients (12.7% and 25.4% for stage I and stage IV diseases, respectively) (P = .024; Figure 4C). For the UNKCC subtype, there was no significant difference in stage at presentation among the three race groups (P = .283; Figure 4D).
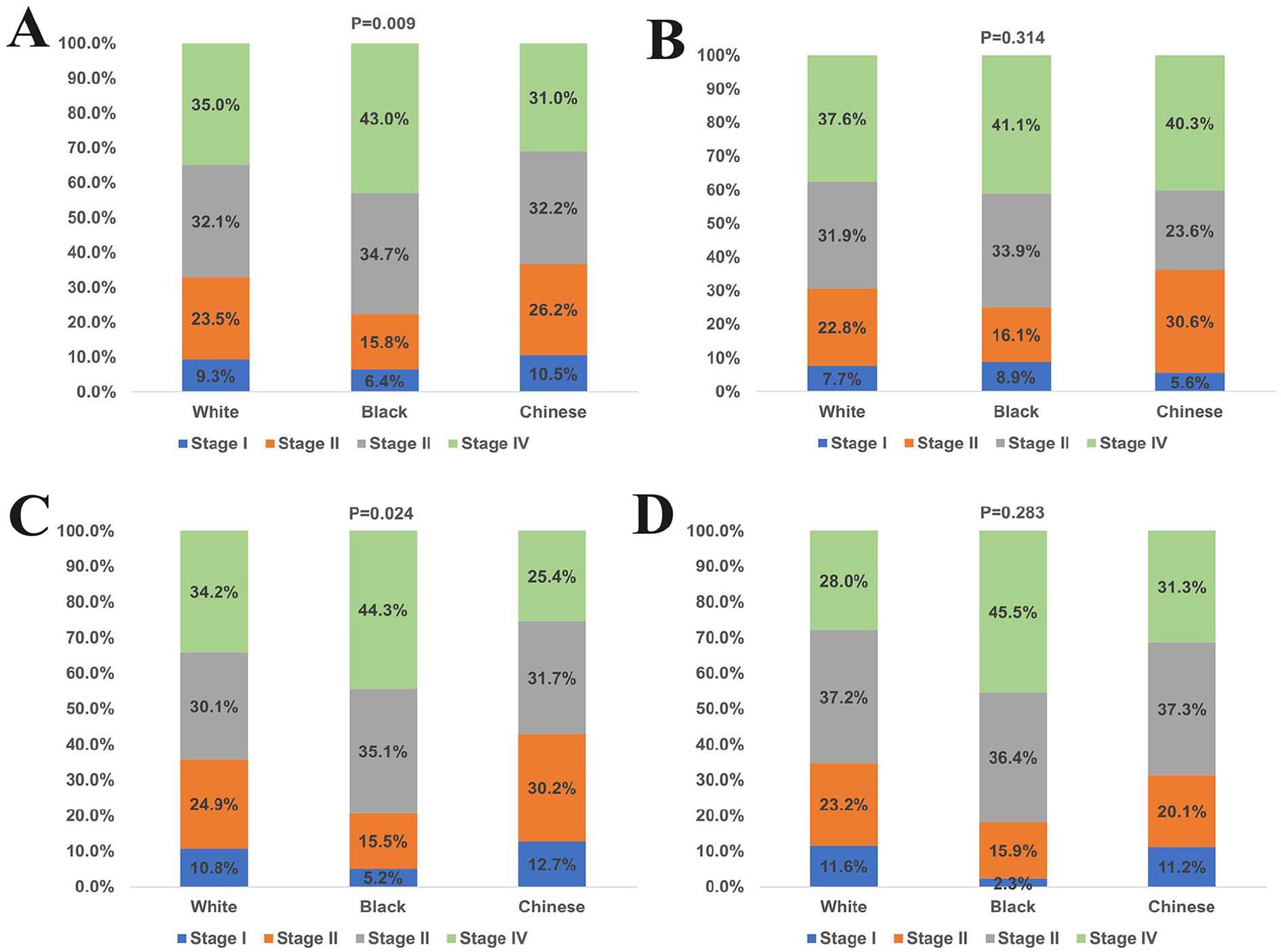
Stage at presentation according to race in the entire cohort (A), keratinizing squamous cell carcinoma (B), differentiated non-keratinizing squamous cell carcinoma (C), and undifferentiated non-keratinizing squamous cell carcinoma (D) cohorts.
Prognostic Analysis in the Entire Cohort
The median follow-up was 56 months. The 5-year NPCSS was 78.7%, 74.2%, and 86.0% in those with KSCC, DNKCC, and UNKCC subtypes, respectively (P = .030; Figure 5A). The 5-year OS was 61.4%, 56.9%, and 80.3% in those with KSCC, DNKCC, and UNKCC subtypes, respectively (P < .001; Figure 5B).
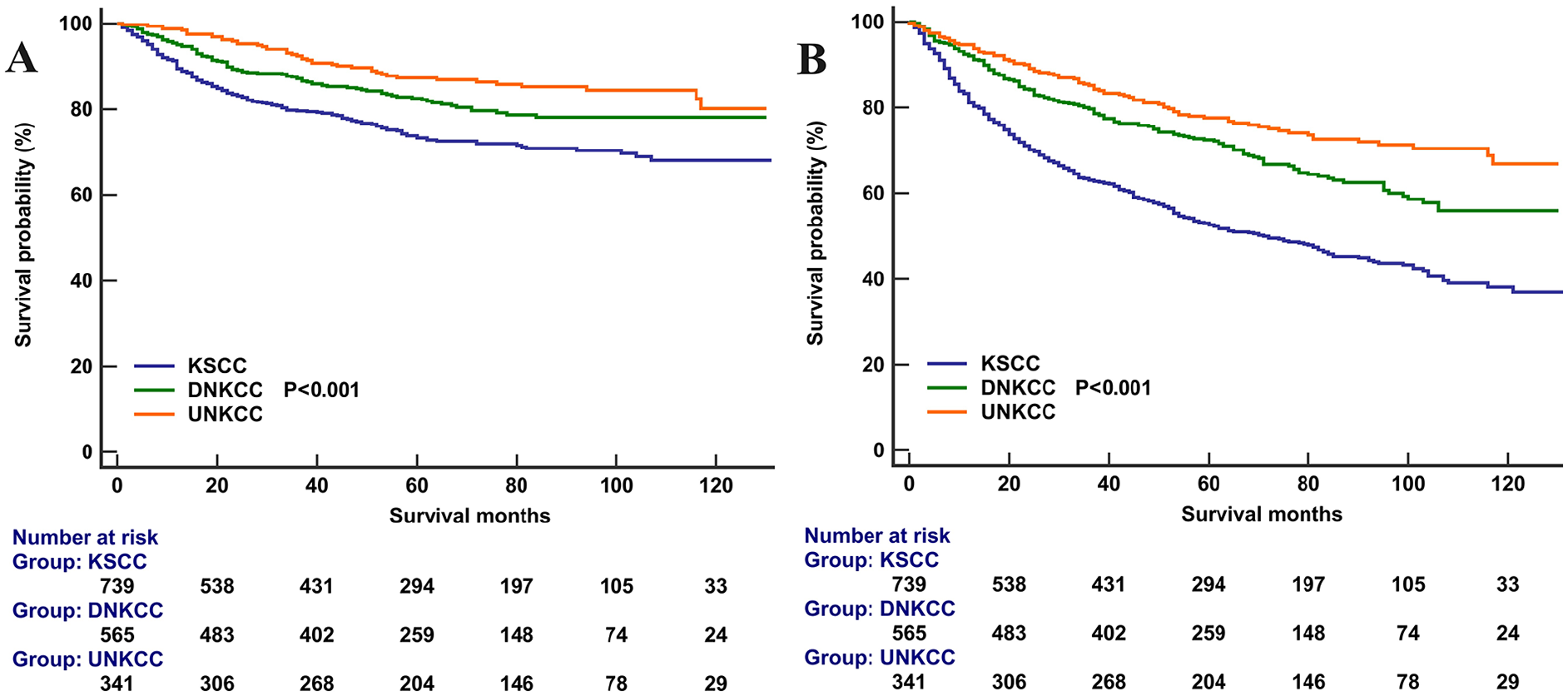
Nasopharyngeal carcinoma-specific survival (A) and overall survival (B) according to histological subtypes in nasopharyngeal carcinoma.
The result of the Cox multivariate analysis showed that race was an independent prognostic factor for OS (Table 2). Non-Hispanic White race [hazard ratio (HR) 1.425, P = .004] and African American race (HR 1.665, P < .004) had significantly poorer OS compared to Chinese American patients. However, race was not related to NPCSS in the multivariate analysis. Histology was also an independent prognostic factor for both NPCSS and OS. Patients with UNKCC (NPCSS: HR 0.715, 95% CI 0.558-0.916, P = .008; OS: HR 0.519, 95% CI 0.373-0.723, P < .001) and DNKCC (NPCSS: HR 0.626, 95% CI 0.524-0.748, P < .008; OS: HR 0.518, 95% CI 0.408-0.659, P < .001) had better NPCSS and OS compared to those with KSCC. Sensitivity analyses showed that histology remained an independent prognostic factor for NPCSS and OS after stratification by race groups (Supplemental Table 1). Survival curves for the effect of histological subtypes on survival outcomes by race groups have been listed in Supplemental Figures 1 to 3. Age, gender, T stage, and N stage were also independent prognostic factors for survival outcomes.
Cox Multivariate Analysis Regarding Independent Prognostic Factors Associated With Nasopharyngeal Carcinoma-Specific Survival and Overall Survival in the Entire Cohort.
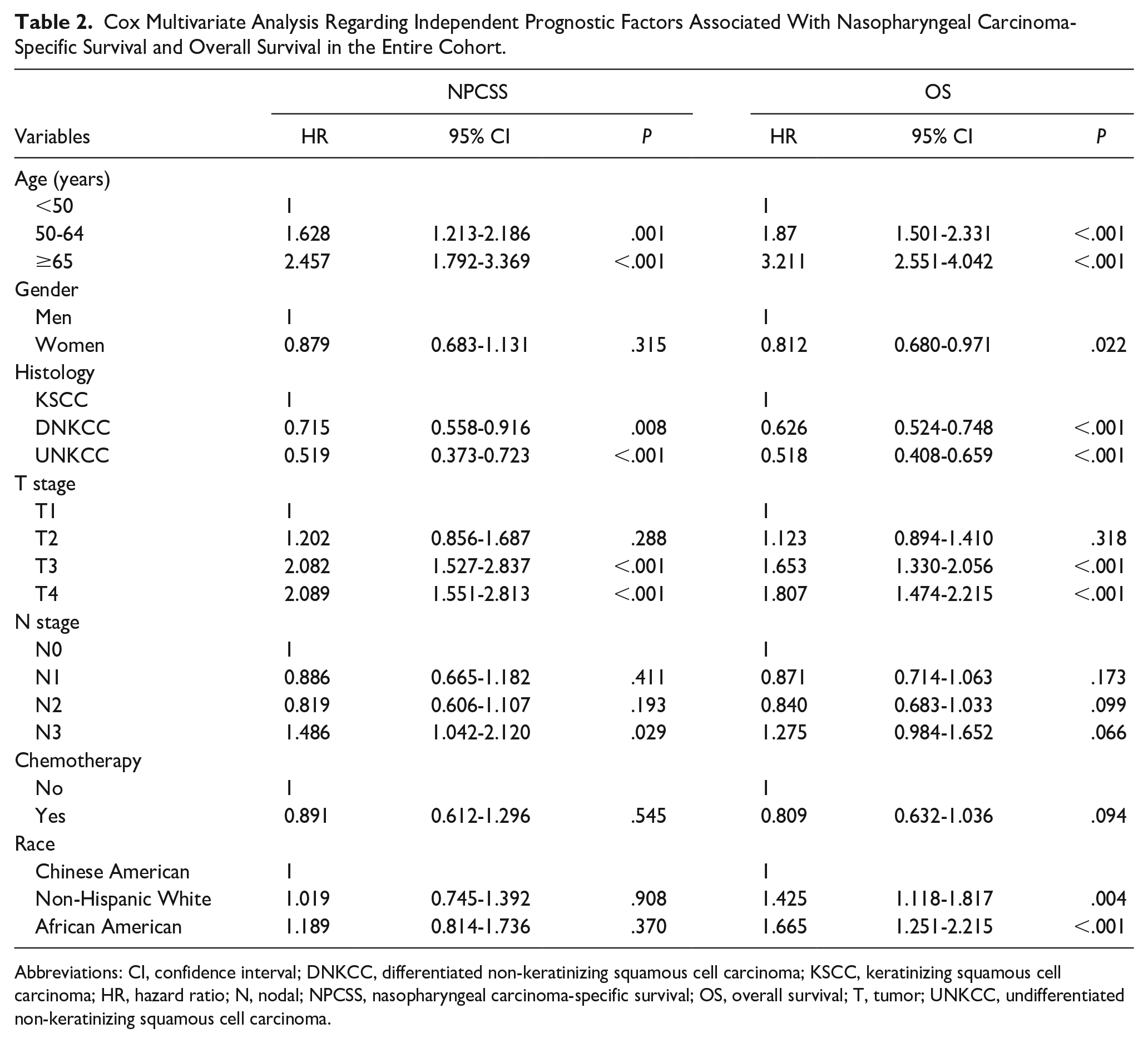
Abbreviations: CI, confidence interval; DNKCC, differentiated non-keratinizing squamous cell carcinoma; KSCC, keratinizing squamous cell carcinoma; HR, hazard ratio; N, nodal; NPCSS, nasopharyngeal carcinoma-specific survival; OS, overall survival; T, tumor; UNKCC, undifferentiated non-keratinizing squamous cell carcinoma.
Prognostic Analysis in the Non-Hispanic White and Chinese American Patients After Propensity Score Matching
After 1:1 PSM, 332 Non-Hispanic White and 332 Chinese American patients were included in the analysis (Supplemental Table 2). The 5-year NPCSS was 82.3% and 86.0% in those with Non-Hispanic White and Chinese American, respectively (P = .534) (Supplemental Table 2). The 5-year OS was 70.1% and 80.3% in those with Non-Hispanic White and Chinese American, respectively (P = .013; Figure 6B). The result of the Cox multivariate analysis showed that OS was significantly lower for Non-Hispanic White patients compared to that in Chinese American patients (HR 1.344, P = .045), while NPCSS was similar between Non-Hispanic White and Chinese American patients (HR 1.063, P = .754; Supplemental Table 3).
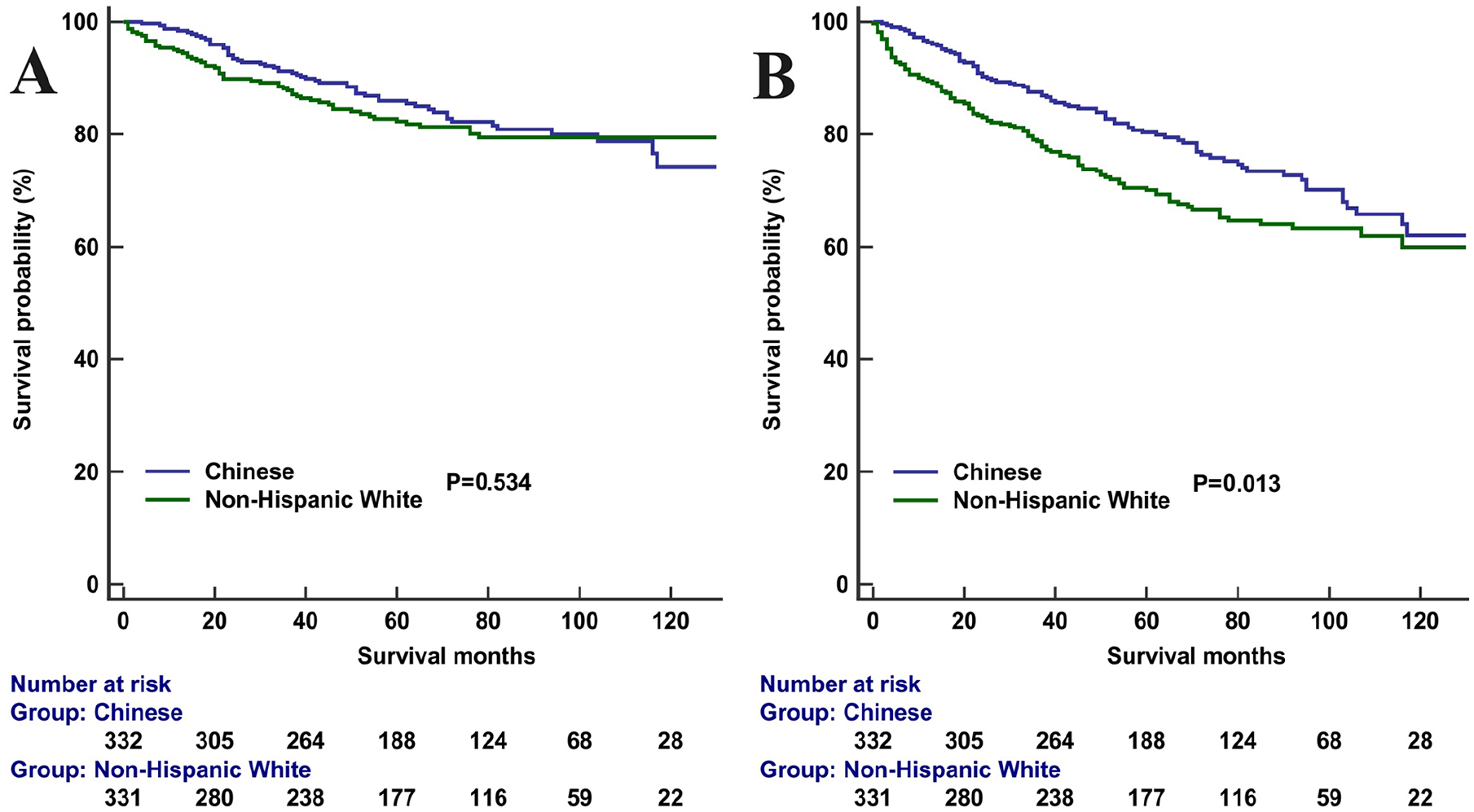
Nasopharyngeal carcinoma-specific survival (A) and overall survival (B) between Non-Hispanic White and Chinese American patients with nasopharyngeal carcinoma.
Prognostic Analysis in the African American and Chinese American Patients After Propensity Score Matching
After 1:1 PSM, 127 African American and 127 Chinese American patients were included in the analysis (Supplemental Table 4). The 5-year NPCSS was 84.9% and 89.0% in those with African American and Chinese American, respectively (P = .484; Figure 7A). The 5-year OS was 67.9% and 83.1% in those with African American and Chinese American, respectively (P = .002; Figure 7B). The result of the Cox multivariate analysis showed that OS was significantly lower in African American patients compared to that in Chinese American patients (HR 2.314, P < .001), while similar NPCSS was found between African American and Chinese American patients (HR 1.459, P = 0.300; Supplemental Table 5).
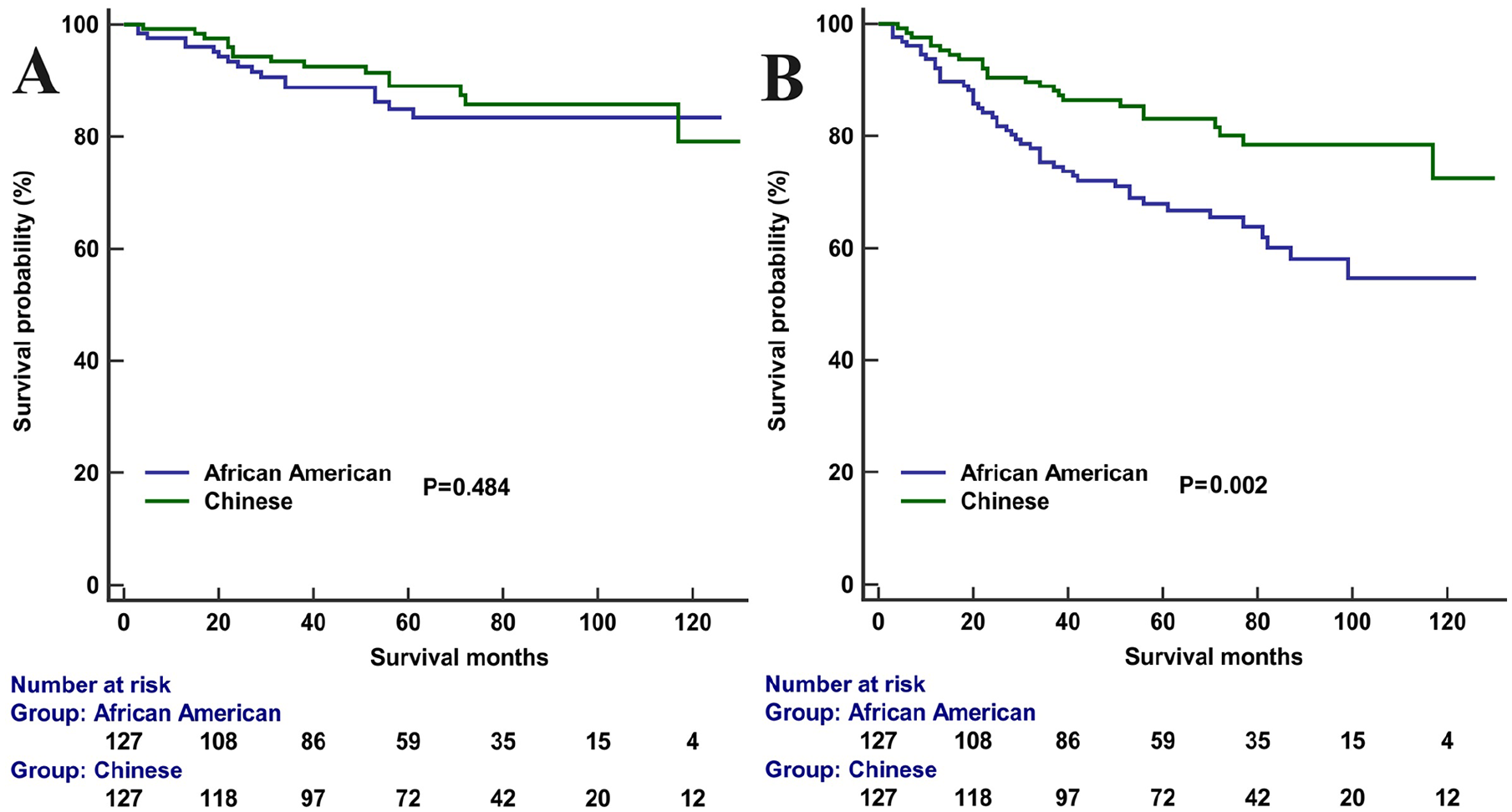
Nasopharyngeal carcinoma-specific survival (A) and overall survival (B) between African American and Chinese American patients with nasopharyngeal carcinoma.
Comparison of Patient Characteristics Between Chinese Americans in the SEER Database and Chinese Patients at the First Affiliated Hospital of Xiamen University
We further analyzed the patient characteristics of Chinese ethnicity diagnosed with NPC in the United States compared to those in mainland China (Supplemental Table 6). The results showed that patients in mainland China were more likely to be younger (P = .013), UNKCC subtype (P < .001), higher clinical stage (P < .001), advanced T stage (P < .001), and advanced N stage (P < .001) compared to Chinese American in the SEER database.
Discussion
By utilizing the SEER database, we aimed to perform a comprehensive analysis of NPC characteristics and survival outcomes, focusing on the ethnic disparities among Chinese American, Non-Hispanic White, and African American patients. This study has the potential to enhance our understanding of the complex interplay between ethnicity, histological subtypes, disease stage, and survival outcomes in NPC. Ultimately, it could inform clinical management strategies and highlight the need for equitable healthcare delivery across different racial and ethnic populations.
We observed that the median age of patients with NPC in our study was 59, 55, and 53 years in Non-Hispanic White, African American, and Chinese American patients, respectively. A recent study found a median age of 60 years in a Japanese cohort. 25 In contrast, the median age of NPC diagnosis in mainland China was found to be 45 years. 26 Additionally, our findings indicated that patients in mainland China were generally younger compared to Chinese American patients. Although the incidence of the disease among the Chinese population in the United States is still lower than that in mainland China, it remains higher than that of other Asian populations. Possible explanations for these racial disparities in NPC incidence may include variations in exposure to the Epstein-Barr virus (EBV) and lifestyle-related risk factors such as diet, smoking, alcohol consumption, pollution, and viral status.
There is a significant correlation between different pathogenic factors and the histological types of NPC. A study of the US population showed that the mean age of patients diagnosed with KSCC, DNKCC, and UNKCC was 57, 53, and 49 years, respectively. 27 The Chinese population is predominantly affected by undifferentiated subtypes, which are closely associated with EBV infection. Early exposure to carcinogens and EBV may contribute to a younger onset of NPC. 28 In non-endemic regions like the United States, cigarette smoking and heavy alcohol consumption have been linked to KSCC.29,30 Several studies suggest that the effects of smoking and alcohol consumption are more pronounced in individuals diagnosed at age 50 or older, indicating potential differences in disease etiology among younger patients.31,32 Therefore, active screening is necessary for Asian populations in the United States, particularly for Chinese individuals.
A previous study in the United States demonstrated that screening Asian American men aged 50 and older using EBV DNA could lead to earlier detection. 33 This may explain why Chinese patients in the United States had a higher probability of being diagnosed with stage I to II disease compared to patients in mainland China in our study. Moreover, a recent study in China identified P85-Ab as a promising novel biomarker for NPC screening, showing higher sensitivity, specificity, and positive predictive value compared to the standard two-antibody method. 34 However, further study is required to determine its value for Chinese Americans or other ethnic patient groups in areas with low incidences of NPC.
In this study, we observed a significant difference in the distribution of histological subtypes among Chinese American, Non-Hispanic White, and African American patients. Chinese American patients predominantly had the UNKCC subtype, while Non-Hispanic White and African American patients had a higher proportion of the KSCC subtype. This indicates potential variations in the underlying biology and molecular characteristics of NPC among different racial/ethnic groups. Genetic differences might make the Southern Chinese population more susceptible to EBV-associated NPC compared to other populations.14,35,36 However, a recent study from the United States found that although the overall incidence of NPC was decreasing, the EBV-related DNKCC subtype was increasing at a concerning rate across all race groups. 27 Studies from Hong Kong and Singapore found that environmental or lifestyle changes might be contributing to a downward trend in NPC incidence rates.16,37 There has been a noticeable decline in NPC incidence among Chinese migrants residing in countries with a low risk of the disease. 38 Similar trends have been observed among all race groups, including Chinese Americans. 39 The decline aligns with changes in population lifestyle, such as reduced alcohol consumption, decreased cigarette smoking, and lower intake of salted fish in Western countries. 40 However, an age-period cohort study from mainland China showed that the NPC incidence has been rising over the past three decades. 41 In our study, we found that the probability of Chinese patients in the United States being diagnosed with KSCC and DNKCC subtypes was significantly higher than that of patients in mainland China. According to the above studies, differences in EBV infection rates, diet, and lifestyle habits may account for variations in the incidence of pathological subtypes among the Chinese population in the two countries. The findings highlight the need for further research to clarify the potential etiological variances among these histological subgroups, which may help address the reasons behind the observed incidence differences.
Our analysis also revealed significant disparities in stage distribution based on race/ethnicity. For all histological subtypes examined, African American patients demonstrated the highest prevalence of stage III to IV disease, particularly among those with the DNKCC subtype. Specifically, stage I disease was less common and stage IV disease was more prevalent among African American patients compared to those Non-Hispanic White or Chinese American patients. This suggests that African American patients may have a higher likelihood of presenting with advanced-stage disease, potentially due to differences in healthcare access, socioeconomic factors, or other disparities. African American populations may face significantly lower odds of receiving screening, higher probability of delayed follow-up, decreased adherence, and loss to follow-up.41-44 Understanding these differences could illuminate potential disparities in healthcare delivery, access to treatment, and genetic factors that may contribute to variations in NPC outcomes.
A study published in the United States in 2002 showed that Chinese American patients had a higher risk of distant metastasis compared to the non-Chinese cohort. 11 Over the past 20 years, advancements in intensity-modulated radiotherapy, concurrent radiochemotherapy, and neoadjuvant chemotherapy have significantly altered the treatment strategies for NPC. However, many prospective studies have been conducted primarily on the Chinese population.17,18 Our results showed that Non-Hispanic White and African American patients had significantly lower OS compared to Chinese American patients. Several factors may contribute to the observed differences in survival outcomes among different racial groups. First, the well-established risk of developing NPC in the Chinese population might lead to more effective screening practices, resulting in earlier diagnosis and treatment. Second, treatment strategies may have varying impacts across different populations. Currently, neoadjuvant chemotherapy combined with concurrent radiochemotherapy is the standard treatment for locally advanced-stage NPC. 45 However, a study from the National Cancer Database (75.5% of patients were White or Black) found that neoadjuvant chemotherapy did not improve survival for locally advanced-stage patients. 5 This finding contrasts with results from prospective studies conducted in regions where NPC is prevalent.46,47 Third, certain genetic factors prevalent in Chinese populations, such as human leukocyte antigen types, may be associated with better treatment response and prognosis. 48 Finally, the onset age of NPC in Chinese Americans is generally younger compared to African American and Non-Hispanic White patients, and younger patients often exhibit higher treatment compliance, which may also contribute to the observed differences in survival outcomes among the three race groups. However, despite differences in OS among racial groups, there was no significant difference in NPCSS among these groups. This suggests that race may influence survival outcomes through factors beyond the specific characteristics of NPC itself.
The results of our study should be interpreted with consideration of its limitations. First, the SEER database lacks information on alcohol use, smoking history, EBV status, and the patterns of disease failures. Second, the SEER database lacks details regarding chemotherapy, such as the type of chemotherapy or the number of chemotherapy cycles. In addition, our study focused solely on Chinese American, Non-Hispanic White, and African American patient populations, and further study is required to explore the impact of race on NPC survival outcomes among other racial and ethnic groups. Moreover, several studies have shown that insurance status significantly affects patient survival, with higher insurance coverage among Asian Pacific Islanders and Non-Hispanic Whites compared to African Americans.49,50,51 Given that only 3.4% to 7.3% of patients were reported as uninsured, we did not analyze the relationship between insurance status and survival across different racial groups. Finally, although the data used in our study were from 2010 to 2017, providing an update from several previous studies,11-14 the patient cohort may not fully reflect the most current treatment practices for NPC. Recent advancements in chemotherapy and immunotherapy have led to substantial changes in the treatment of NPC in recent years.52,53
Conclusions
In conclusion, our study demonstrates that race influences histological subtype distribution, stage at presentation, and survival outcomes in NPC. Future research should focus on identifying the underlying factors contributing to these racial disparities and improving diagnostic and therapeutic strategies to improve survival outcomes among all racial and ethnic groups affected by NPC.
Supplemental Material
sj-pptx-1-ear-10.1177_01455613241282410 – Supplemental material for Racial Disparities in Nasopharyngeal Carcinoma Characteristics and Survival
Supplemental material, sj-pptx-1-ear-10.1177_01455613241282410 for Racial Disparities in Nasopharyngeal Carcinoma Characteristics and Survival by De Yu, Hai-Bo Xu, Gui-Ping Chen and San-Gang Wu in Ear, Nose & Throat Journal
Footnotes
Authors Contributions
Conception and design: S.G.W., H.B.X., D.Y., and G.P.C.; Administrative support: G.P.C. and S.G.W.; Provision of study materials or patients: D.Y., H.B.X., and G.P.C.; Collection and assembly of data: D.Y., H.B.X., and S.G.W.; Data analysis and interpretation: D.Y., H.B.X., and S.G.W.; Manuscript writing: All authors; Final approval of manuscript: All authors.
Consent for Publication
Not applicable.
Data Availability Statement
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethics Approval and Consent to Participate
As the SEER program only contains anonymized data, our study was exempt from the approval process by the ethics committee. The study was conducted in accordance with the Declaration of Helsinki (as revised in 2013).
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.