
Abstract
Introduction
Orthognathic surgery relies on careful preoperative planning, precise execution of the chosen surgical plan, and prevention of postoperative relapse to achieve the desired results for all oral, maxillofacial, and otorhinolaryngology surgeons. 1 Advancing over the last decades, orthognathic surgery has become safer, more rapid, less expensive, and more successful.2,3
This treatment is indicated when the patient’s jaws are incompatible with oral functions or have a severe malocclusion that makes the sole orthodontic treatment inadequate. 4 One of orthodontics’ foremost objectives is the treatment planning and execution of orthognathic surgery. A meticulous diagnostic protocol is required to simulate surgical displacements and predict the orthodontic movements necessary to conveniently achieve a stable and balanced surgical occlusion. 5
Preoperative planning is the most crucial phase in the workflow process for orthognathic surgery. 6 Combining the planning technique and the technique to transfer the plan ensures the accuracy of the diagnosis and analysis and the orthognathic surgery outcomes. 7 Orthognathic surgery has long embraced traditional surgical planning (TSP) encompassing clinical records, two-dimensional (2D) radiographs, the use of patients’ photographs, and manual model surgery as the standard preoperative procedure. Nonetheless, this approach has its drawbacks, especially for patients with significant facial deformities or asymmetry, as 2D cephalometric radiographs fail to provide complete information about three-dimensional (3D) structures.8,9
Due to the inherent difficulties in visualizing, planning, and predicting 3D structures and operations in 2D, there has been a recent trend toward working virtually on 3D, 10 and virtual surgical planning (VSP) has emerged as an alternative to TSP. 11
When the focal point is correcting dentofacial deformity, current advances in VSP have been considered valuable for diagnosis, treatment planning, and evaluation of the results.12,13 Since the late 20th century, the development of 3D technologies, such as computer-aided design/computer-aided manufacturing (CAD/CAM) and 3D CAD systems, has led to an expeditious rise of VSP in orthognathic surgery.14,15 VSP integrates fan-beam or cone-beam computed tomography (CBCT) with software tools that allow 3D treatment planning in orthognathic surgery. It enables surgeons to evaluate the predictable planning and the surgical outcomes through 3D virtual osteotomy, 3D soft tissue simulation, 3D surgical splint manufacturing, and 3D superimposition. 16 Computer-simulated osteotomy and prediction systems enable surgeons to simulate different surgical approaches to determine the best outcomes 17 while intraoperative computer navigation systems aid in repositioning the maxillo–mandibular complex accurately as planned.18,19 CAD/CAM surgical splints and patient-specific plates are broadly used to transfer VSP accurately. 7
Three-dimensional patient data provides a roadmap for a precise diagnosis, 3D cephalometric measurements, virtual planning of surgical technique, and prediction of the effect of these surgical movements on the dentoskeletal complex and soft tissue envelope 20 ; thus, VSP enables the orthodontist and surgeon to predict postoperative hard and soft tissue displacements and optimize orthodontic preparation for surgery. 21
Despite these advantages, a comprehensive review of the literature indicates that the superiority of VSP over TSP in terms of sagittal plane accuracy and patient satisfaction remains to be determined. 1 Various studies propose different methods to evaluate the precision of postoperative outcomes regarding VSP. The most frequently utilized method is linear and angular measurements based on cephalometric landmarks to calculate the difference between VSP and postoperative outcomes.16,22
Recent studies focus on the accuracy between VSP and surgical outcomes regarding various evaluation methods that cannot be compared and identified at the same level. In recent reviews, it was stated that the success of surgical outcomes depends on the accurate transfer of surgical planning, and deviations of less than 2 mm between VSP and actual outcomes are not considered clinically significant.23,24
Studies have illustrated that virtual planning is a precise and repeatable method for orthognathic surgical planning; however, further clinical studies are still needed. 9
Another focal point is surgical sequencing. The traditional surgical method primarily repositions and stabilizes the maxilla, followed by repositioning and stabilizing the mandible. Nevertheless, advances in rigid internal fixation methods have enabled the first mandible to be repositioned. 25 The more rigid attachment of the maxilla to the skull base, in contrast to the mandible connected to the skull base with movable joints, reveals that the upper jaw will potentially function as a more accurate guide for the first operated jaw, which is the mandible. 26 Repositioning the mandible first has the primary benefit of eliminating major mistakes in condylar position and malocclusion that result from using the maxilla-first technique. 25
The latest focus has been on mandible-first sequencing due to its recognized benefits in achieving significant maxillary advances and counterclockwise rotation. Moreover, numerous research examining the accuracy of VSP have identified constraints in interpreting findings in both surgical sequences. These limits stem from regions that require enhancement in the study design and the methodologies employed to assess the outcomes. Another area for improvement in mandible-first sequencing is the need for a greater understanding of surgical planning and procedures.9,22
Surgical sequencing can affect results in terms of accuracy; nonetheless, various studies indicate that both sequences offer comparable outcomes when properly planned and executed.27,28
A review of the literature on this topic has created relative indications of which mandible-first sequence is recommended. 29 Evidence-based experimental studies should address this question more objectively and search for a common ground to address this long-debated topic. 30
In light of the related literature above, the current article aims to evaluate whether the clinical outcome of VSP is affected by the mandible-first or maxilla-first treatment methods. This study tests the hypothesis that operating maxilla-first will provide more precise clinical results than the mandible-first technique.
Materials and Methods
The present retrospective and observational study included 45 individuals (aged 18–38, 20 men/25 women). Ethical approval of the study was obtained from the Istanbul Medipol University Non-Interventional Clinical Research Ethics Committee (File Number: # E-10840098-772.02-E.43589) and was carried out in accordance with the principles stated in the Declaration of Helsinki.
This retrospective study included patients who had undergone orthognathic surgery for dentofacial deformity, specifically either maxilla-first or mandible-first surgery. These patients’ diagnosis and treatment planning were done only through 3D-VSP (NemoFAB; Nemotec, Madrid, Spain). All computed tomography (CT) scans in this investigation were acquired with the condyles in a centric relation (CR), which was determined clinically and stabilized using a wax bite. The maxilla received classical Le Fort 1 osteotomy treatment, while the mandible was treated with bisagittal split ramus osteotomies Dalpont–Hunsuck modification. Rigid internal fixation was applied to the relevant jaws with mini plates and screws. Internal fixation was used, and the condyle was placed manually. An evaluation was conducted by comparing the displacements of specific landmarks and preoperative and postoperative conventional computed tomographies 31 with the displacements of landmarks derived via VSP through the software, following the recommendations of Gaber et al. 22
Patients diagnosed with craniofacial syndrome, cleft lip-palate, degenerative condylar disease, or facial trauma, as well as patients who underwent additional surgical procedures, such as multi-segment Le Fort I osteotomy, were excluded from the study. This study focused exclusively on single-piece Le Fort I and bilateral sagittal split osteotomy procedures to accurately assess deviations without interfering with other variables.
Each case is characterized by age, gender, malocclusion, type of dentofacial deformity, facial proportion (symmetry or asymmetry), surgical treatment planning (clockwise or counterclockwise rotation of the maxillomandibular complex and anteroposterior movements), and surgical sequence (maxilla first, typical sequence; mandible first, reverse sequence) in the database.
Orthodontic Phase Prior to Surgery
Prior to surgery, all patients received orthodontic treatment to correct the alignment of both dental arches, resolve overcrowding, and establish a stable bite.
Clinical Evaluation Prior to Surgery
Every patient received a comprehensive clinical assessment, which involved taking images of the face and mouth from outside as well as inside and capturing detailed digital scans of the mouth using TRIOS 3 technology (3Shape, Copenhagen, Denmark). Clinical measurements obtained from the patients were recorded in the CR, which is one of the most reliable and repeatable positions of the condyle within the fossa.32,33 The CR was recorded using the chin tip guidance technique and bite registration material (Cavex Holland BV, RW Haarlem, The Netherlands).
Clinical photography and videos
Following the suggestion of Lundström et al, 34 the patients were positioned in the natural head position. The set of images included a frontal photo of each patient smiling and reposing on a black background, along with 45° and profile shots taken from the right and left of the patient. Patient instructions aided standardization.
Intra-oral optical surface scans
Due to CT’s limited 3D resolution, maxillary and mandibular arches and bite registration were scanned directly with an intra-oral optical scanner. In our study, the TRIOS 3 scanner was used because TRIOS 3, a confocal scanner, generally showed the best performance considering both the scanning speed and the accuracy. 36 The upper and lower arches and the bite registration were digitally converted to standard triangle language (STL) files.
Pre-Operative Radiographic Evaluation
Maxillofacial CT scans of the patients were taken in the supine position with a CT device (iCT 256 Slice; Philips, Amsterdam, Holland) in the Radiology Department of Medipol Mega University Hospital, 7 to 10 days before (T0) and approximately 6 months after (T1) the operation, which is our clinical protocol. The head was oriented so that the Frankfurt Horizontal Plane was perpendicular to the ground. Then, with the help of the laser markers on the CT device, the midline was checked and the head and neck were placed in the desired position. To ensure that the CT images were obtained when the mandible was in the CR, the CR registration wax was placed in the patient’s mouth and checked that it was in the correct position. It was noted that the soft tissues of the patient were not deformed by the bite registration. The patient was instructed that his eyes and mouth should be closed, his lips should be at rest, and that he should remain motionless, breathing through his nose and without swallowing. After these scans were obtained, the images were encrypted in the Digital Imaging and Communications in Medicine (DICOM) format. To recreate jaws and dental arches, STL files were overlaid onto a DICOM file from CT scans using a specialized software (Mimics® Innovation Suite; Materialise NV, Brussels, Belgium). The software was used to segment the mandible and maxilla semi-automatically.
Three-dimensional lateral cephalometric measurements were obtained and analyzed using Arnett analysis to ascertain the degree of malposition in each jaw and the motions necessary for correction.
Virtual Surgical Planning
In terms of the mandible-first group, bilateral sagittal split osteotomies were executed. Following the repositioning of the mandible to the intended position, the intermediate splint was designed. Subsequently, Le Fort I osteotomy of the maxilla was performed, and the maxilla was repositioned to the intended position. Consequently, the final splint was created.
The maxilla-first group adhered to the same protocols as the mandible-first group. Nevertheless, it is crucial to note that, for this group, the maxilla was repositioned before the intermediate splint was designed. Subsequently, the mandible was repositioned, and subsequently, the final splint was devised. Both splints were fabricated via a commercial stereolithography printer, namely the FormLabs 3B+ model from FormLabs, located in Somerville, MA, USA.
Surgical interventions
All surgical interventions were performed under general anesthesia. Intraoral injection of local anesthetic (Articaine HCl, 40 mg/mL, Alfacaine; Weimer Pharma GmbH, Rastatt) was administered along the incision lines to achieve local hemostasis.
Mandible-first group
Intraoral incisions on planned sites were made by electrocautery. The inferior border of the mandible buccally, the temporal tendon superiorly, and the sigmoid notch and lingula posteriorly were dissected. The surgical technique of this group involved a mandible-first sequence with a bisagittal split osteotomy performed following the Dalpont–Hunsuck modification. The mandibular distal segment was then positioned in its final position utilizing an intermediate splint and rigid intermaxillary fixation (IMF) with heavy elastic bands. Bivectoral seating was performed to reposition the condyles in the fossae appropriately. 36 To achieve a better bone-to-bone fit while keeping the condyle in the proper position with a bivectorial maneuver during plating, any premature bone contact that would get in the way of passive proximal segment positioning was eliminated. Then 2 titanium mini plates were placed on each side to stabilize the osteotomy passively. Following the completion of osteosynthesis, the IMF was removed and the proper mandibular position was confirmed by ensuring that it corresponded to the intermediate splint when manipulated in a CR.
Then a vestibular intraoral incision was made for the maxilla by electrocautery. The maxilla was dissected at the level of the infra-orbital foramen superiorly and the pterygoid plates posteriorly. After the maxilla was completely released from its bony attachments, it was fractured downward and mobilized. The final splint was then used as a guide to reposition the upper jaw to achieve the desired final position and occlusion. To achieve the planned vertical position of the maxilla, we used a surgical pen to mark a point on the glabella region. Then we measured the distance between this point and the bracket of tooth 11 and, based on this measurement, adjusted the planned amount of impaction or down-grafting intraoperatively. Titanium mini-plates were used to stabilize the maxilla to its new position. Once again, the IMF was removed and the proper maxillary position was confirmed by ensuring that it corresponded to the final splint when manipulated in a CR. There was no use of a rigid maxillo-mandibular fixation after surgery. If needed, elastic bands were used to stabilize the results.
Maxilla-first group
The procedures performed for the maxilla-first group were identical to those performed for the mandible-first group, except that the maxillary surgical procedures were performed first, followed by the mandibular surgical procedures.
Measurement of Surgical Movements
Our method involved surface-based superimposition on the cranial base of pre-operative and post-operative 3D virtual models to measure surgical movements and to compare them with those planned to obtain clear and clinically interpretable results.
Firstly, pre-operative and post-operative CT data in DICOM format were transferred to Mimics software to create 3D models. The models were then transferred to 3-matic software (Materialise NV) in STL format. Surface-based registration was executed on the cranial bases of the pre-operative and post-operative models. The superimposed 3D models were then transferred back to Mimics software. Skeletal and dental landmarks were located 3-dimensionally on both models for each patient to measure surgical movements.
The landmarks where the fiducials were placed on the models and taken sagittal, vertical, and lateral movements into consideration are as follows: anterior nasal spine (ANS), posterior nasal spine (PNS), B Point, Pog (skeletal landmarks), and the mesio-incisal angle of the upper and lower right central incisors (Max 1R and Mand 1R, respectively), the cusp tips of the upper and lower canines (Max 3R, Max 3L, Mand 3R, and Mand 3L, respectively), and the mesio-vestibular cusp tips of the upper and lower first molars (Max 6R, Max 6L, Mand 6R, and Mand 6L, respectively).
We utilized the coordinate difference to assess the surgical movements relative to the positioned landmarks after exporting the X, Y, and Z coordinates of each landmark to a spreadsheet (Microsoft Excel; Microsoft Corp., Redmond, WA, USA). Next, we examined the data obtained by superimposing the 3D models with similar measurements that were automatically computed for each example using the virtual planning application.
Statistical Analysis
The sample size was calculated according to the previous research (field 38) investigating the accuracy of VSP in orthognathic surgery. The software program (G*power version 3.1, Los Angeles) was used to measure the mean movements of the study groups. The effect size was found to be 0.38 and α = .05. In the sample size analysis carried out with a power value of 0.80, the total number of samples required to be taken was found to be 45.
In this study, statistical calculations were performed with the NCSS (Number Cruncher Statistical System) 2007 Statistical Software (Utah, USA) program for Windows. Besides standard descriptive statistical calculations [mean and standard deviation (SD), median, interquartile range (IQR)], the distribution of the variables was examined with the Shapiro–Wilk normality test. The Mann–Whitney U test was used in the comparisons of the planned and analysis results of the variables that did not show a normal distribution, the Kruskal–Wallis test was used in the comparisons between multiple groups, the Dunn multiple comparison test was used for the subgroup comparisons, and the Wilcoxon test was used for comparisons of paired groups. The compatibility of planned and analysis results was determined by intra-class correlation coefficient (ICC), 95% confidence interval, and Bland–Altman tests. The results were evaluated at the significance level of P < .05.
Results
The study included a total of 45 participants, with 20 being men and 25 being women. The age range of the individuals varied from 18 to 38 years. There were a total of 6 patients who underwent orthognathic surgery on a single jaw, with 3 of them being men and the other 3 being womene. Orthognathic surgery including both the upper and lower jaws was conducted on a total of 39 patients. The maxilla-first approach group consisted of 8 male and 13 female patients, all of whom were 21 years old. The mandible-first approach group included of 9 male and 9 female patients, all of whom were 18 years old (Tables 1 and 2).
ICC of Skeletal and Dental Landmarks Measurements.
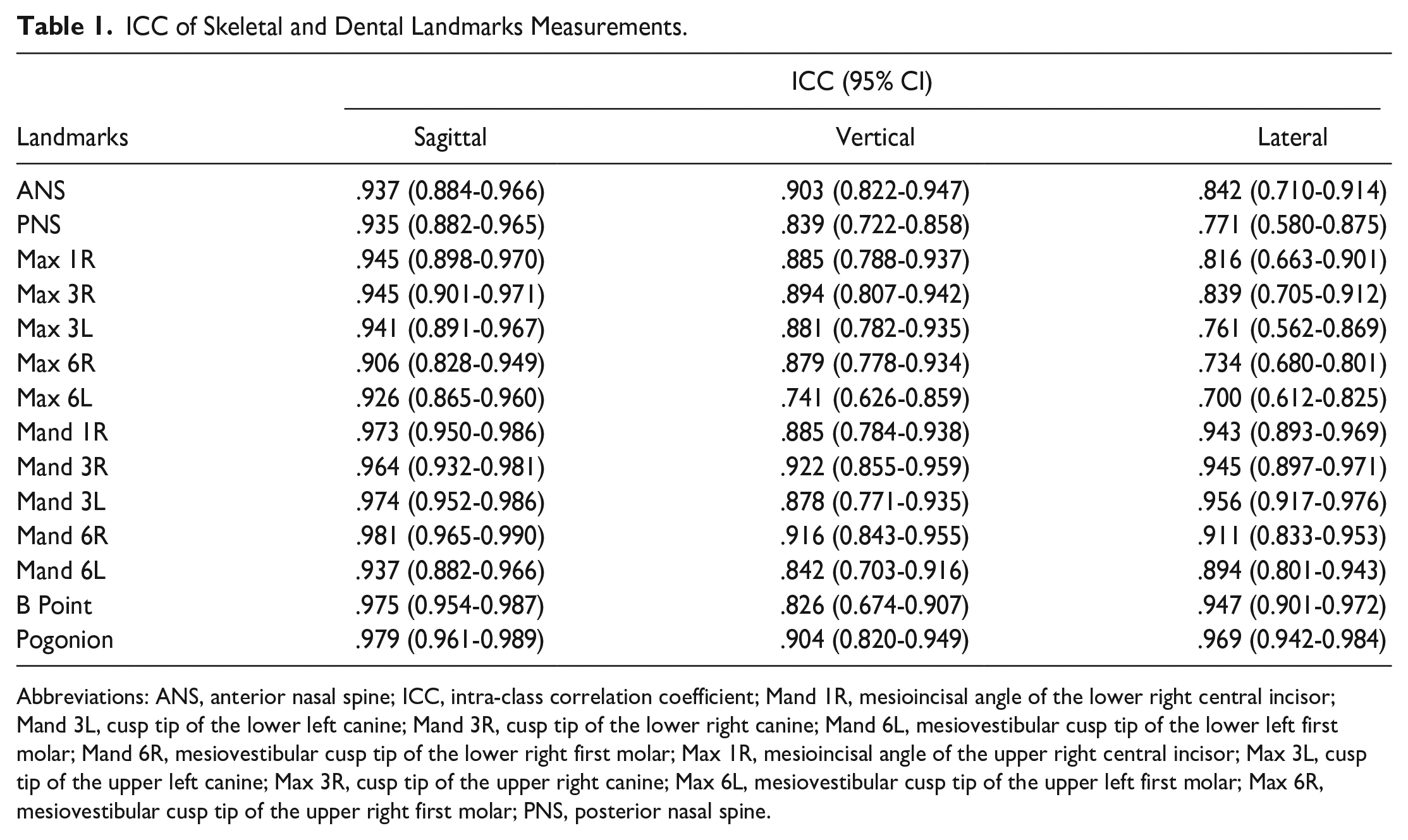
Abbreviations: ANS, anterior nasal spine; ICC, intra-class correlation coefficient; Mand 1R, mesioincisal angle of the lower right central incisor; Mand 3L, cusp tip of the lower left canine; Mand 3R, cusp tip of the lower right canine; Mand 6L, mesiovestibular cusp tip of the lower left first molar; Mand 6R, mesiovestibular cusp tip of the lower right first molar; Max 1R, mesioincisal angle of the upper right central incisor; Max 3L, cusp tip of the upper left canine; Max 3R, cusp tip of the upper right canine; Max 6L, mesiovestibular cusp tip of the upper left first molar; Max 6R, mesiovestibular cusp tip of the upper right first molar; PNS, posterior nasal spine.
The Bland–Altman Analysis of Skeletal and Dental Landmarks Measurements, the Mean Difference, and Compliance Limit of the Values Between the Planned and Analysis Results.
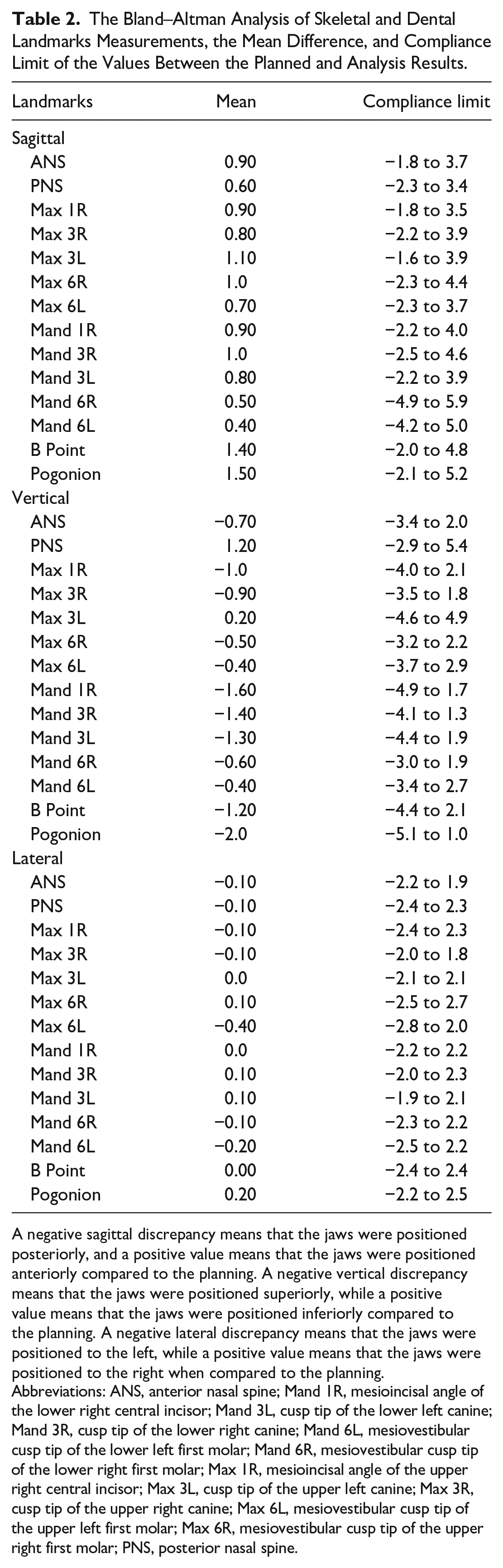
A negative sagittal discrepancy means that the jaws were positioned posteriorly, and a positive value means that the jaws were positioned anteriorly compared to the planning. A negative vertical discrepancy means that the jaws were positioned superiorly, while a positive value means that the jaws were positioned inferiorly compared to the planning. A negative lateral discrepancy means that the jaws were positioned to the left, while a positive value means that the jaws were positioned to the right when compared to the planning.
Abbreviations: ANS, anterior nasal spine; Mand 1R, mesioincisal angle of the lower right central incisor; Mand 3L, cusp tip of the lower left canine; Mand 3R, cusp tip of the lower right canine; Mand 6L, mesiovestibular cusp tip of the lower left first molar; Mand 6R, mesiovestibular cusp tip of the lower right first molar; Max 1R, mesioincisal angle of the upper right central incisor; Max 3L, cusp tip of the upper left canine; Max 3R, cusp tip of the upper right canine; Max 6L, mesiovestibular cusp tip of the upper left first molar; Max 6R, mesiovestibular cusp tip of the upper right first molar; PNS, posterior nasal spine.
The desired limit value for the ICC of all skeletal and dental landmark measurements was found to be above .700. Measurements are compatible (Table 1).
A “negative sagittal discrepancy” indicates a posterior positioning of the jaws, while a positive number indicates an anterior positioning of the jaws in relation to the planning. A negative vertical discrepancy means that the jaws were positioned superiorly, whereas a positive value means that the jaws were positioned inferiorly compared to the planning. A negative lateral discrepancy means that the jaws were positioned to the left, whereas a positive value means that the jaws were positioned to the right compared to the planning (Table 2).
Regarding the Bland–Altman chart, it can be seen that in sagittal measurements, all comparison differences of the results measured by the 2 methods for the ANS, PNS, Max 1R, Max 3R, Max 3L, Max 6R, Max 6L, Mand 1R, Mand 3R, Mand 3L, and B Point variables are within this range. Most of the Mand 6R, Mand 6L, and Pogonion variables are within this range (Table 2).
It can be seen that in vertical measurements, all comparison differences of the results measured by the 2 methods of the ANS, Max 1R, Max 3R, Max 6R, Max 6L, Mand 1R, Mand 3R, Mand 3L, Mand 6R, Mand 6L, B Point, and Pogonion variables are within this range. Most of the PNS and Max 3L variables are within this range (Table 2).
In lateral measurements, all comparison differences of the results measured by the 2 methods of the ANS, PNS, Max 1R, Max 3R, Max 6R, Max 6L, Mand 1R, Mand 3R, Mand 3L, Mand 6R, Mand 6L B Point, and Pogonion variables are within this range. Most of the Max 3L variable is within this range (Table 2).
This study showed a statistically significant relationship between the measurements performed with the 2 methods (r = .944; P = .0001). The fact that the ICC value is statistically significant and relatively high and that most of the differences in the Bland–Altman chart fall between the limits of compliance indicates a correlation between the measurements of the 2 methods. A high ICC suggests that the difference between the values measured by the 2 methods is always constant or very close to each other. Concerning the Bland–Altman chart, it is seen that the mean difference between the results measured by the 2 methods is −1.3, the upper and lower limits of compliance of these differences are between 4.0 and −6.5, and all comparison differences are within this range (Tables 1 and 2).
Although 45 patients participated in this study, only 39 underwent bimaxillary surgery. The maxilla-first approach group included 8 male and 13 female patients of 21. The mandible-first approach group included 9 male and 9 female patients of 18. Six patients who underwent single jaw orthognathic surgery were excluded from the analysis of comparison of surgical sequencing in virtual planning evaluation (Tables 3-5).
Comparison of Planning-Analysis Absolute Mean Differences of Skeletal and Dental Landmarks Measurements of Mandible-First and Maxilla-First Groups in the Sagittal Direction.
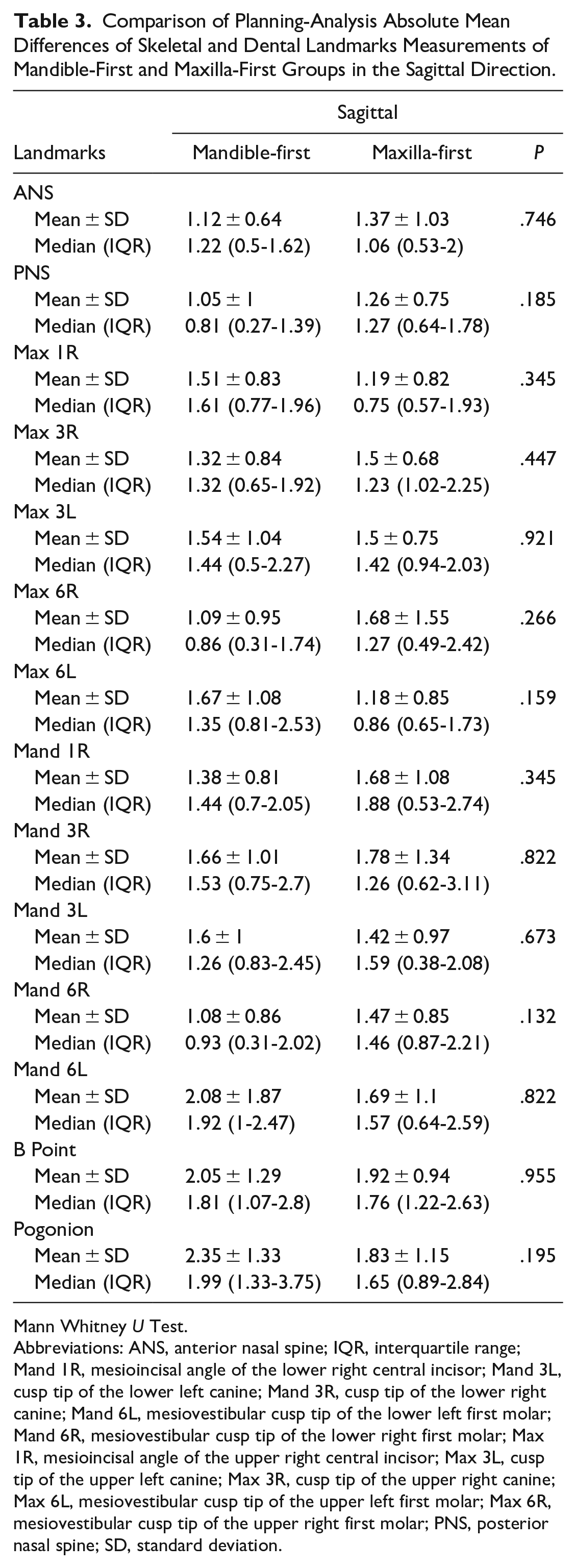
Mann Whitney U Test.
Abbreviations: ANS, anterior nasal spine; IQR, interquartile range; Mand 1R, mesioincisal angle of the lower right central incisor; Mand 3L, cusp tip of the lower left canine; Mand 3R, cusp tip of the lower right canine; Mand 6L, mesiovestibular cusp tip of the lower left first molar; Mand 6R, mesiovestibular cusp tip of the lower right first molar; Max 1R, mesioincisal angle of the upper right central incisor; Max 3L, cusp tip of the upper left canine; Max 3R, cusp tip of the upper right canine; Max 6L, mesiovestibular cusp tip of the upper left first molar; Max 6R, mesiovestibular cusp tip of the upper right first molar; PNS, posterior nasal spine; SD, standard deviation.
Comparison of Planning-Analysis Absolute Mean Differences of Skeletal and Dental Landmarks Measurements of Mandible-First and Maxilla-First Groups in the Vertical Direction.
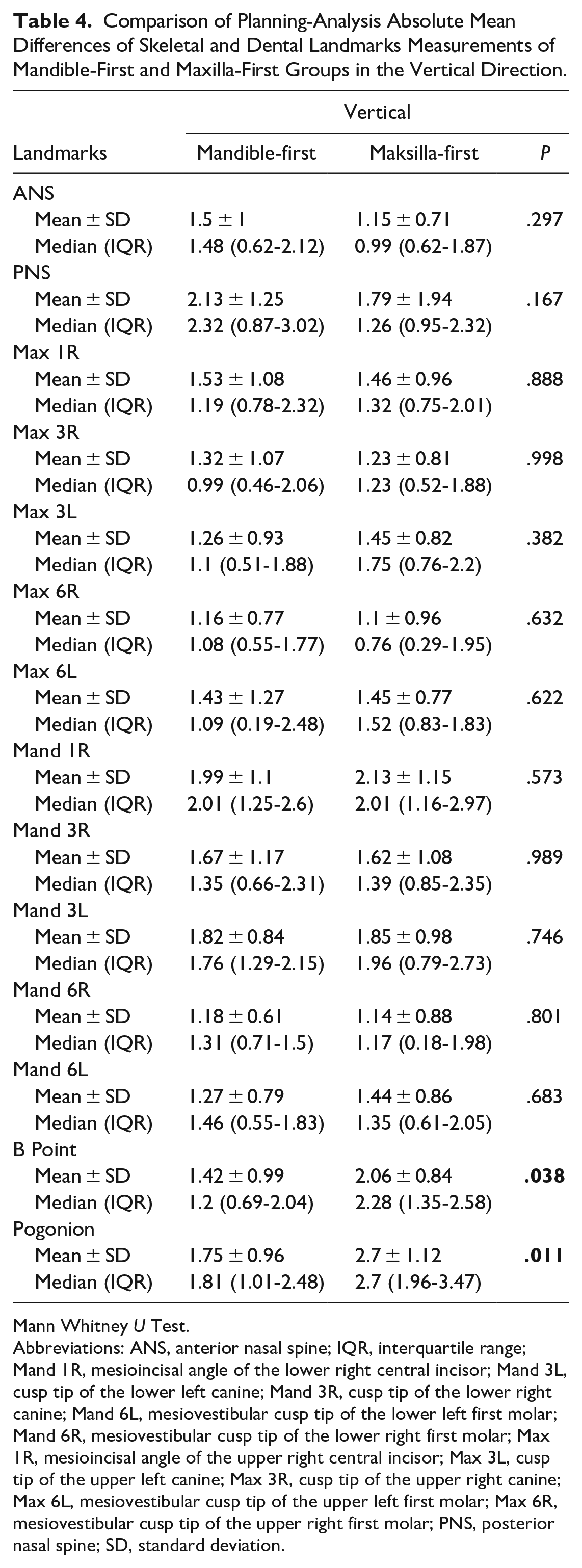
Mann Whitney U Test.
Abbreviations: ANS, anterior nasal spine; IQR, interquartile range; Mand 1R, mesioincisal angle of the lower right central incisor; Mand 3L, cusp tip of the lower left canine; Mand 3R, cusp tip of the lower right canine; Mand 6L, mesiovestibular cusp tip of the lower left first molar; Mand 6R, mesiovestibular cusp tip of the lower right first molar; Max 1R, mesioincisal angle of the upper right central incisor; Max 3L, cusp tip of the upper left canine; Max 3R, cusp tip of the upper right canine; Max 6L, mesiovestibular cusp tip of the upper left first molar; Max 6R, mesiovestibular cusp tip of the upper right first molar; PNS, posterior nasal spine; SD, standard deviation.
Comparison of Planning-Analysis Absolute Mean Differences of Skeletal and Dental Landmarks Measurements of Mandible-First and Maxilla-First Groups in the Lateral Direction.
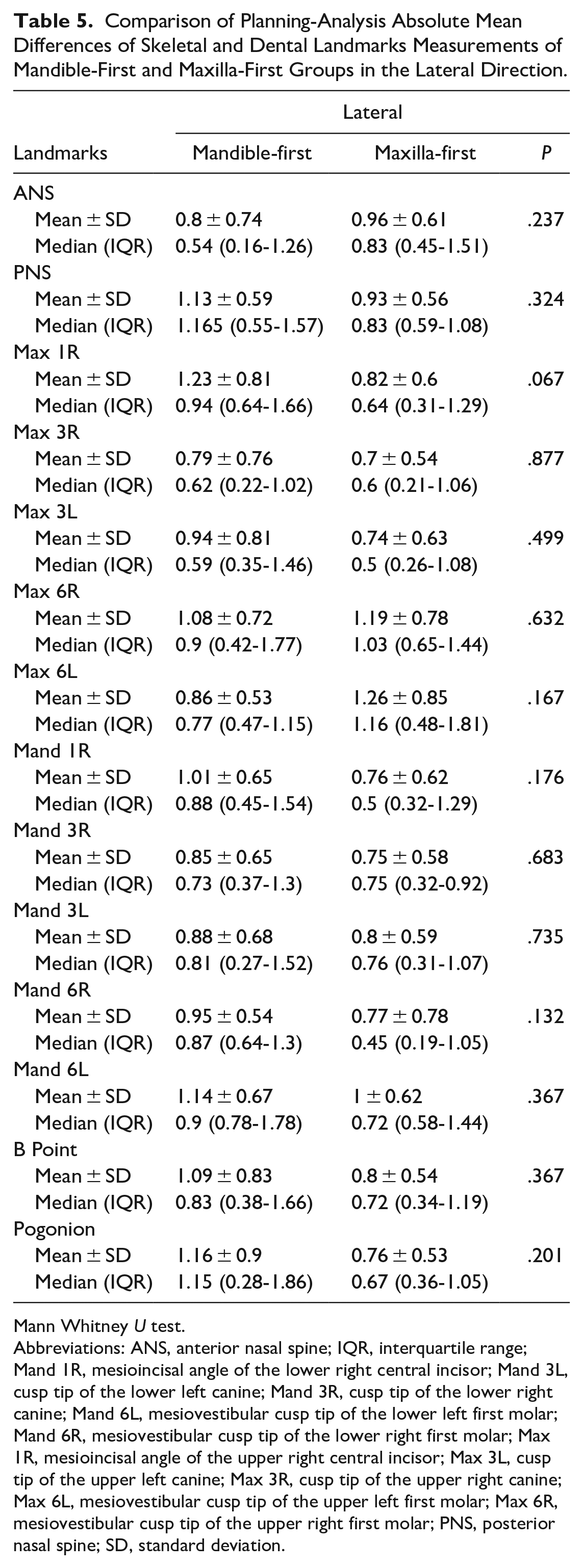
Mann Whitney U test.
Abbreviations: ANS, anterior nasal spine; IQR, interquartile range; Mand 1R, mesioincisal angle of the lower right central incisor; Mand 3L, cusp tip of the lower left canine; Mand 3R, cusp tip of the lower right canine; Mand 6L, mesiovestibular cusp tip of the lower left first molar; Mand 6R, mesiovestibular cusp tip of the lower right first molar; Max 1R, mesioincisal angle of the upper right central incisor; Max 3L, cusp tip of the upper left canine; Max 3R, cusp tip of the upper right canine; Max 6L, mesiovestibular cusp tip of the upper left first molar; Max 6R, mesiovestibular cusp tip of the upper right first molar; PNS, posterior nasal spine; SD, standard deviation.
In vertical measurements, the absolute mean difference of the B Point and the Pogonion between the planning and analysis in the Maxilla-first group were statistically significantly higher than in the Mandible-first group (P = .038, P = .011). No statistically significant differences were observed in the remaining landmarks in all spatial dimensions (P > .05) (Tables 3-5).
Discussion
Orthognathic surgeries done by oral, maxillofacial, and otorhinolaryngology surgeons dedicated to correcting jaw deformities have significantly improved with computer-aided diagnosis and treatment planning techniques. 37 VSP has emerged as a powerful tool that offers enhanced precision and improved surgical outcomes. There are various advantages of VSP. Fawzy and Choi stated that using 3D-VSP enhanced the predictability of specific components of the planning process, including the rotational movement of the maxillo-mandibular complex around the Y axis (yaw movement), which is impossible to control with conventional planning. 20
According to the findings of Zinser et al, the mandibular condyle remained centrally located in the temporomandibular joint, which was not observed with traditional planning. 37 On the other hand, according to Lee et al, the condylar position may have been altered during surgery by gravity and muscle tone due to the patient’s supine position, influencing the ideal condylar seating. 38 Regarding this matter, Stokbro et al share the same viewpoint. 39
Accurate quantification of surgical movements remains paramount for objective assessment of surgical technique and outcome analysis. The current study implemented surface-based registration of pre-operative and post-operative 3D virtual models, achieving exceptional ICC (ICC > .99) across all evaluated parameters. This approach offers a significant advantage by minimizing operator dependency and potential bias inherent in subjective evaluations. It surpasses the limitations associated with methods such as iterative closest point (ICP) analysis. Although ICP is a frequently employed technique, it exhibits limitations in capturing subtle 3D deviations in surgical manipulation. Additionally, ICP algorithms may only be universally applicable across some anatomic regions due to their inability to account for the entirety of the 3D mesh generated from CBCT/CT scans. 40 De Riu et al pointed out that simple superimposition techniques, often used in superimposition, can lead to significant errors, particularly in scenarios involving substantial surgical manipulation. These errors become even more concerning when dealing with delicate procedures that require high precision. 41 Surface-based registration, on the other hand, offers a robust and objective solution for quantifying surgical movements. This method provides a more comprehensive assessment of surgical manipulation, overcoming the limitations observed with traditional techniques.
A further potential cause of inaccuracy could be the use of landmarks located on 3D radiographic volumes, where positioning errors can vary from 0.02 to 2.47 mm in all directions, contingent on the landmark identification technique. 42 In our study, the landmarks we used were straightforward and easy to locate, so the positioning errors were minimal. For instance, we utilized easily identifiable anatomical landmarks such as the mesioincisal angle of the central incisors or the intersection of specific bone structures, which reduced the margin of error in our measurements. This approach ensured that our data were more reliable and precise compared to using ambiguous or difficult-to-locate landmarks.
The mean error differences in superimposition between the virtual plan and the postoperative outcomes are frequently utilized methods to assess the precision of virtual planning. Ho et al evaluated precision using the root mean square difference (RMSD) between 3D simulations and post-operative CBCT scans. They reported acceptable errors with maxillary and mandibular RMSDs of 0.63 ± 0.25 mm and 0.85 ± 0.41 mm, respectively. 8 Baan et al employed a similar approach to evaluate the correspondence between planned and achieved positions, additionally investigating surgical repeatability among surgeons. Their findings suggested that the vertical positioning of the maxilla and mandible showed the greatest discrepancies between the VSP and the post-operative outcomes, potentially reflecting limitations in intraoperative vertical control. 16 De Riu et al also reported good accuracy for most parameters assessed in VSP. They found a mean error of 1.98 mm for linear measurements and 1.19° for angular measurements. In particular, they observed statistically significant differences (P = .033) between the planned and actual anterior facial heights, which were not present in the absence of genioplasty (U test; P = .45). 41 Unlike Ho et al, in our study, we assessed the deviations of landmark movement values after surgery by superimposing the actual pre-operative and post-operative tomography data and comparing it with the data obtained from our VSP. By this way, we were able to accurately assess the precision of the surgical procedure in our patients. Our results showed that the surgical transfer of VSP is highly accurate in all spatial dimensions when comparing planned and actual performed movements. The reference marker placed on soft tissue instead of fixed hard tissue for intraoperative control of anterior facial height on the glabella may have caused potential deviations in the vertical direction observed in our study.
Several studies support the accuracy of computer-aided planning (CAP) 43 for maxillary translation in orthognathic surgery. Hsu et al reported high precision with less than 1 mm maxillary translation errors. This technology facilitates not only precise maxillary positioning but also correction of complex deformities involving yaw deviations, segmental alignments, and mandibular asymmetry. 44 Stokbro et al demonstrated an average linear accuracy of 0.5 mm or less for the maxilla, mandible, and chin segments in the 3 spatial planes. Notably, their analysis revealed the greatest precision in the superoinferior direction, followed by the mediolateral and anteroposterior directions. 39 Baan et al observed the lowest absolute mean difference in the right/left translations for both the maxilla (0.49 mm) and the mandible (0.71 mm) compared to VSP and postoperative outcomes, indicating the superiority of CAP in this aspect. Furthermore, their findings suggested a posterior positioning of the maxilla (1.41 mm) in 7 of 10 patients relative to the VSP plan, with a similar trend seen in the mandible (1.17 mm posterior displacement in 8 of 10 patients). 16 In addition, Sun et al reported good accuracy in the right/left positioning with mean deviations of 0.32 and 0.75 mm for the maxilla and mandible, respectively, in their analysis of 23 patients using (OrthoGnathic Analyser software, Gyeonggi-do, Republic of Korea). Their study indicated a lower RMSD for the maxilla (0.6 mm) than for the mandible (0.85 mm). 45
Since the introduction of internal rigid fixation, concerns have been generated about the most appropriate sequence of osteotomies to correct dentofacial abnormalities and produce stable clinical results. Sequencing in bimaxillary orthognathic surgery has been a topic of considerable debate. 29 VSP has allowed surgeons to tailor sequence selection according to individual preferences by offering detailed preoperative planning and simulations. Despite ongoing discussions on the pros and cons of maxilla-first and mandible-first approaches and research on accuracy and surgical outcomes, a definitive consensus still needs to be reached due to conflicting findings and interpretations. Due to inconclusive results and varying outcomes, the existing data do not definitively favor either the maxilla-first or mandible-first sequence. 46 A scoping review by researchers identified key decision-making factors prior to implementing maxilla-first or mandible-first sequencing. These acknowledged determinants include the magnitude of sagittal movement (small vs large), rotational direction of the maxillomandibular complex [clockwise vs counter-clockwise (CCW)], reliability of the CR registration, the need for maxillary segmentation, and the thickness of the splint. 46 In this investigation, we implemented a decision-making algorithm for sequence selection based on these factorsto determine the most appropriate treatment plan for each patient. The strict selection criteria for the sequencing protocol may have contributed to the accurate results observed in our data’s coronal and sagittal directions. This approach minimized the potential for errors and inconsistencies in our surgical outcome.
Mandible-first sequencing provides advantages in specific scenarios. It facilitates large maxillo-mandibular advancement and CCW rotation, potentially improving dental contacts and enabling a thinner and more stable intermediate splint due to reduced interarch distance. In multi-segmental maxillary osteotomies, the mandible provides a stable occlusal reference for fragment positioning, promoting precise and deep intercuspation without a palatal splint. 25 Similarly, the mandible-first sequence is recommended in maxillary down-grafting cases since the intermediate splint would be excessively thick and the Temporomandibular Joint (TMJ) could become dislocated during the surgery. 25 The mandible can be accurately repositioned in its distal segment, independent of the CR of the condyles during IMF, by using the non-operated maxilla as a fixed reference point. However, proper condylar positioning within the fossa during plating remains crucial for determining the final mandibular position at IMF release.29,47,38 Posnick recommended mandible-first sequencing when reliable pre-operative bite registration is unattainable 48 or when temporomandibular joint surgery precedes orthognathic procedures, as the latter inevitably alters condylar position.25,28 However, the mandible-first approach is not without limitations. During surgery, challenges may require a switch to a maxilla-first sequence, such as difficulties with passive condylar positioning or managing a bad split of the mandible. 46
The maxilla-first sequence is indicated in the clockwise rotation of the maxillo-mandibular complex, small maxillo-mandibular advancements when performing a single-piece Le Fort I osteotomy, or when internal rigid fixation is not possible. When maxillary impaction is necessary, this sequencing is also preferred because it makes it possible to manufacture an intermediate splint that is thin enough to enable intraoperative rigid IMF. 49
The degree to which surgical sequence selection may affect the accuracy of treatment is another factor to take into account. Several studies claimed that because both sequences execute VSP with a similar level of precision, they are equally accurate.27,50 Other researchers, on the other hand, claimed that the conventional approach, with variations in particular surgical movements, yields more accurate findings. 51 The mandible-first technique was reported by Stokbro et al to be more precise when rotation was carried out in a CCW direction, whereas the conventional sequence seemed to provide more accurate findings when rotation was carried out in a clockwise (CW) direction. 52
According to Shah et al and Abel et al, maxillo-mandibular advancement in the sagittal direction was mostly underachieved by the mandible-first technique.53,54 According to Salmen et al, the maxilla-first approach resulted in more aesthetically pleasing results because the vertical position of the upper incisors was more accurately determined. 49 On the contrary, Borikanphanitphaisan et al stated that the heterogeneity of the selected experimental studies in their study had allowed a meta-analysis of the accuracy of the surgical outcome of a single landmark (at upper central incisors), and this meta-analysis concluded that the accuracy produced at upper central incisors was not different between both approaches. 27
On the other hand, for the vertical position of Pogonion, the mandible-first approach was more accurate. Our results are also parallel to this study; in vertical measurements, the absolute mean difference of the B Point and the Pogonion between the planning and analysis in the Maxilla-first group were statistically significantly higher than in the Mandible-first group (P = .038, P = .011). Besides these landmarks, it should be emphasized that both sequences may be regarded as equally accurate because the discrepancies observed by all investigations are clinically not significant. 46
A further concern is the degree of mandibular auto-rotation necessary to form the intermediate splint. A higher degree of inaccuracy is thought to result from a greater mouth opening. Nonetheless, a recent research disproves this theory by not being able to find a correlation between mandibular autorotation and the inaccuracy of the final result. 38
Trevisiol et al concluded that, based on indications and contraindications for sequencing, the mandible-first sequence seems to be the superior alternative in most cases of bimaxillary surgery. 46 The surgeon’s knowledge and experience are crucial in selecting the surgical sequence, which is determined by evaluating each case separately regarding which jaw should be operated first. 46
Effective VSP planning significantly influences accurate surgical outcomes, although it is not the sole determinant. Various factors can affect the final position of the mandible, potentially leading to disparities between the planned and actual results. These factors include pre-operative data acquisition techniques, surgical sequence selection, fixation methods, surgeon experience, and crucially, intraoperative condylar position management.51,55,56 Regardless of the VSP method employed, an inaccurate repositioning of the condyle within the fossa during osteosynthesis can significantly deviate the final mandibular position from the planned one.16,56 Current studies in this area appear to under-emphasize or inadequately address the impact of these variables. Incorrect repositioning of the condyle, regardless of the planned movement’s type or extent, can create consistent disparities between VSP and surgical outcomes. 46
Conclusion
VSP has emerged as a valuable tool in orthognathic surgery, demonstrably improving surgical precision and achieving desired outcomes. This study employed surface-based registration, a robust and objective method for quantifying surgical movements, and yielded exceptional ICC. Our findings corroborate the high accuracy of VSP reported in previous studies for the sagittal and coronal planes and less accuracy for the vertical planes for all cases. Our study demonstrates that VSP with both maxilla-first and mandible-first sequencing achieves high accuracy and reproducibility in the sagittal and coronal planes.
Although VSP offers significant advantages, achieving optimal surgical outcomes hinges on various factors beyond planning accuracy. Intraoperative considerations such as condylar positioning and fixation methods can influence the final mandibular position and introduce discrepancies between planned and actual results.16,39 Future research should devote greater attention to intraoperative variables to refine surgical techniques and minimize discrepancies. Ultimately, surgeon expertise and a comprehensive evaluation of each case are paramount to selecting the most appropriate surgical sequence and achieving optimal clinical outcomes.
Footnotes
Acknowledgements
None.
Author Contributions
All authors contributed to the planning, designing, literature survey, surgery, writing, active intellectual support, and English editing.
Data Availability Statement
The available data of the study may be sent upon request for scientific purposes.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Statement
This study was approved by The Istanbul Medipol University Non-Interventional Clinical Research Ethics Committee (File Number: # E-10840098-772.02-E.43589).
Grant Number
Not applicable.
Informed Consent
Informed consent was obtained from the patients before they were included in the study.
Trial Registration Number/Date
Not applicable.