
Abstract
Introduction
The World Health Organization (WHO) recommends that school hearing screening programs should be implemented in all member states.1,2 Early identification and intervention for children with hearing loss should reduce the well-known adverse effects of hearing loss on childhood development and social well-being.1,2 The Sustainable Development Goal Project offers an opportunity for the implementation of school ear and hearing programs in the Pacific Islands. 3
The Pacific Island region has among the highest rates of ear disease and hearing loss in the world.4,5 This is largely attributed to lack of access to healthcare services generally, 4 limited ear and hearing health services specifically,6,7 as well other health indices that increase the risk of developing chronic ear disease.8,9 Otitis media begins early in life and may progress to chronic and possibly life-threatening complications if poorly managed.8,10 A survey of primary school students in the Melanesian nation of the Solomon Islands found that 56.6% did not pass their ear health examination, with otitis media with effusion (OME) and impacted cerumen as the leading ear pathologies diagnosed. 11 A review of students attending a school for people with disabilities in the Polynesian nation of Samoa found that 61% required intervention for an ear health condition, most commonly cerumen removal. 12 The literature suggests goodwill and momentum among Pacific Island nations to address ear disease. 13 Previous work from Samoa and the Solomon Islands found that there was high parental awareness of ear disease as a major cause of hearing loss in children (88.7%-94%), as well as overwhelming support for school-based ear and hearing programs (97.3%-99.3%).14,15 Further studies from Samoa have also found high professional support for childhood ear and hearing health programs among educators, 16 and current and future health professionals.17,18 It is also clear that ear and hearing health initiatives should embrace their Pacific Islander cultural contexts to achieve optimal outcomes.19,20 At this time, there is no research from the Pacific Islands investigating for differences in ear disease presentation based on geographic location, and it is well-established from research in other low- and middle-income settings that ear disease is likely to be significantly more prevalent among rural/remote populations than urban counterparts. 2
Samoa is a Polynesian nation of the Pacific Islands (Figure 1). The Ear, Nose & Throat (ENT) Clinic of the Tupua Tamasese Meaole Hospital in Samoa was re-established in 2017 under the leadership of General/ENT Surgeon (SP), and it is the only ENT Clinic in the country. Public health, development, and research audiologist (AK) joined the Samoan ENT Clinic team in 2019. Given that school-aged children represent a significant proportion of the daily ENT clinical caseload, there was goodwill and momentum among ENT Clinic staff members to implement routine school outreach visits. Improving the rate of early detection and management of ear disease among schoolchildren in Samoa should in turn reduce the rate of preventable hearing loss and its impact on social well-being and educational outcomes.

Map of Samoa (image developed by authors).
The aim of this study is to describe the prevalence and pattern of ear disease among primary school students in urban, rural, and remote areas of Samoa. The results of the study should provide evidence for the implementation and protocol development of a national School Ear and Hearing Program.21,22. It will expand on the previous work from the Solomon Islands by assessing primary school students from both urban and rural/remote settings, and it will also enable comparison between 2 different Pacific Island nations, possibly providing insights into ear and hearing health differences between Melanesian and Polynesian populations.
Methods
Ethical Approvals
Ethical approval for this study was granted by the Health Research Ethics Committee of the Government of Samoa Ministry of Health, including approval to publish. Approval was also granted by the Government of Samoa Ministry of Education, Sports & Culture, as well as the University of Queensland Health and Behavioural Sciences, Low & Negligible Risk Ethics Sub-Committee (Approval Number: 2020000255). Gatekeeper approval was also obtained from the participating schools during the ENT Clinical outreach visits.
Study Design: Retrospective Clinical Data Review
A retrospective clinical data review was performed of all primary school students seen by the ENT Clinic of Samoa during school-based outreach visits in 2022 to 2024. This time frame included periods of lockdown during the COVID-19 pandemic, as well as closure of the ENT Clinic while staff were seconded to support COVID-19 prevention and management efforts. The ENT school outreach visits were also dependent on competing interests of the ENT Clinic staff as well as participating school availability. The clinical records of all students seen during the school outreach service were eligible for inclusion in the study, and there were no exclusion criteria. The ENT Specialists (SP, MAK) performed all ear examinations and recorded their findings on the clinical record of each student. Any procedures (ie, wax removal) were performed by the ENT nurses.
The following de-identified information was extracted from the clinical records of each student and entered into a purposefully designed IBM Statistical Package for the Social Sciences (SPSS) spreadsheet: school location (urban, rural, remote), gender (male, female), age (years), age category (0-4, 5-9, 10-14, 15+ years), right/left ear diagnosis [no abnormalities detected, acute otitis media (AOM), acute otitis media with perforation (AOMwiP), chronic suppurative otitis media (CSOM), dry tympanic membrane perforation, eustachian tube dysfunction (ETD), OME, wax, foreign body, fungal otitis externa, bacterial otitis externa, other], nurse intervention (wax removed, foreign body removed, otorrhea removed), and action required (no further action, review with primary care, review at ENT Clinic).
School location (urban/rural/remote) was defined to align with current Ministry of Health practice, where the capital city Apia is “urban,” the rest of the island Upolu is “rural,” and the island of Savai’i is “remote”.
Given the design of this study (retrospective review of clinical records), data collection was based on ear examination diagnosis as recorded on the clinical records. Routine diagnostic criteria used by the ENT Clinic of Samoa defines (1) CSOM as a suppurating tympanic membrane perforation for more than 2 weeks, (2) dry TM perforation as a perforation of the tympanic membrane with no suppuration, and (3) ETD as a retraction of the tympanic membrane with no other abnormalities observed (ie, no OME, cholesteatoma).
Data Analysis
Data analysis was performed in collaboration with the Hearing Research Unit for Children at the University of Queensland (Brisbane, Australia; CD). Student demographic information was summarized using descriptive statistics. For each ear, the ear examination diagnoses, nurse interventions, and action required were tallied. Association tests of significance were performed to assess for any significant differences between location, age, and gender variables. Further chi-squared tests of significance were performed as required. The age variable categories for comparison were the 5 to 9 and 10 to 14 year-old age groups: this aligns with the WHO Ear and Hearing Survey Handbook, 23 and is appropriate given the low numbers outside the 5 to 14 years age range in the study population.
Results
Overview of Study Population Demographic Information
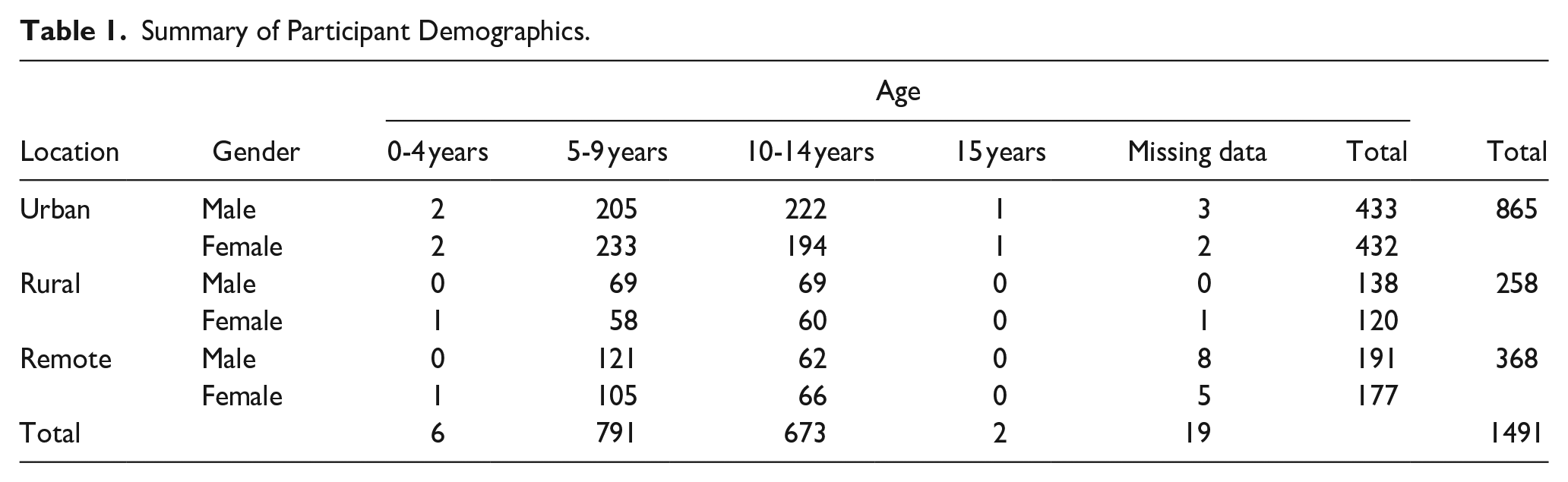
Five schools were attended by the ENT Clinic during the study period, and a total of 1491 primary school students were seen for ear health examinations (51.1% male, 48.9% female). The age range was 4 to 15 years, with a median of 9 years, and a mean age of 9.1 years (SD = 2.3). Participating students represented urban (n = 865, 58%), rural (n = 258, 17.3%), and remote (n = 368, 24.7%) settings. Study population demographics are summarized in Table 1.
Summary of Participant Demographics.
Overview of Ear Examination Results
Overall, 682 (45.7%) students had normal ear examination results for both ears, 237 (15.9%) had an ear pathology in 1 ear only, and 568 (38.1%) had ear pathology in both ears. The most common pathology was cerumen requiring removal (n = 549 or 36.8% of students), followed by OME (n = 113 or 7.5% of students). Overall prevalence of CSOM was 2.6% (n = 39 students). An overview of ear examination results is summarized in Figures 2 and 3, and an overview of tests of significance results is summarized in Table 2.
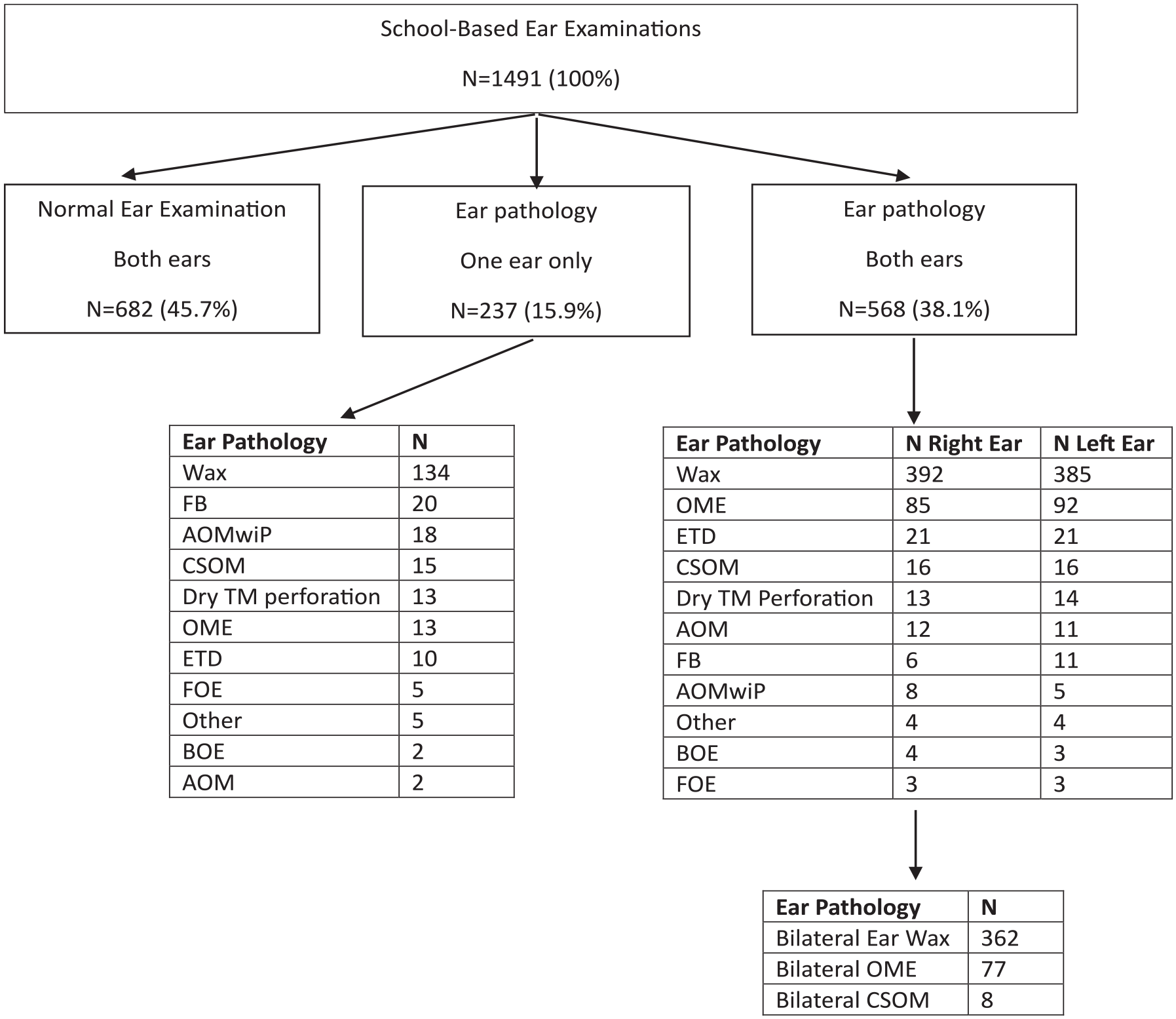
Overview of study results.
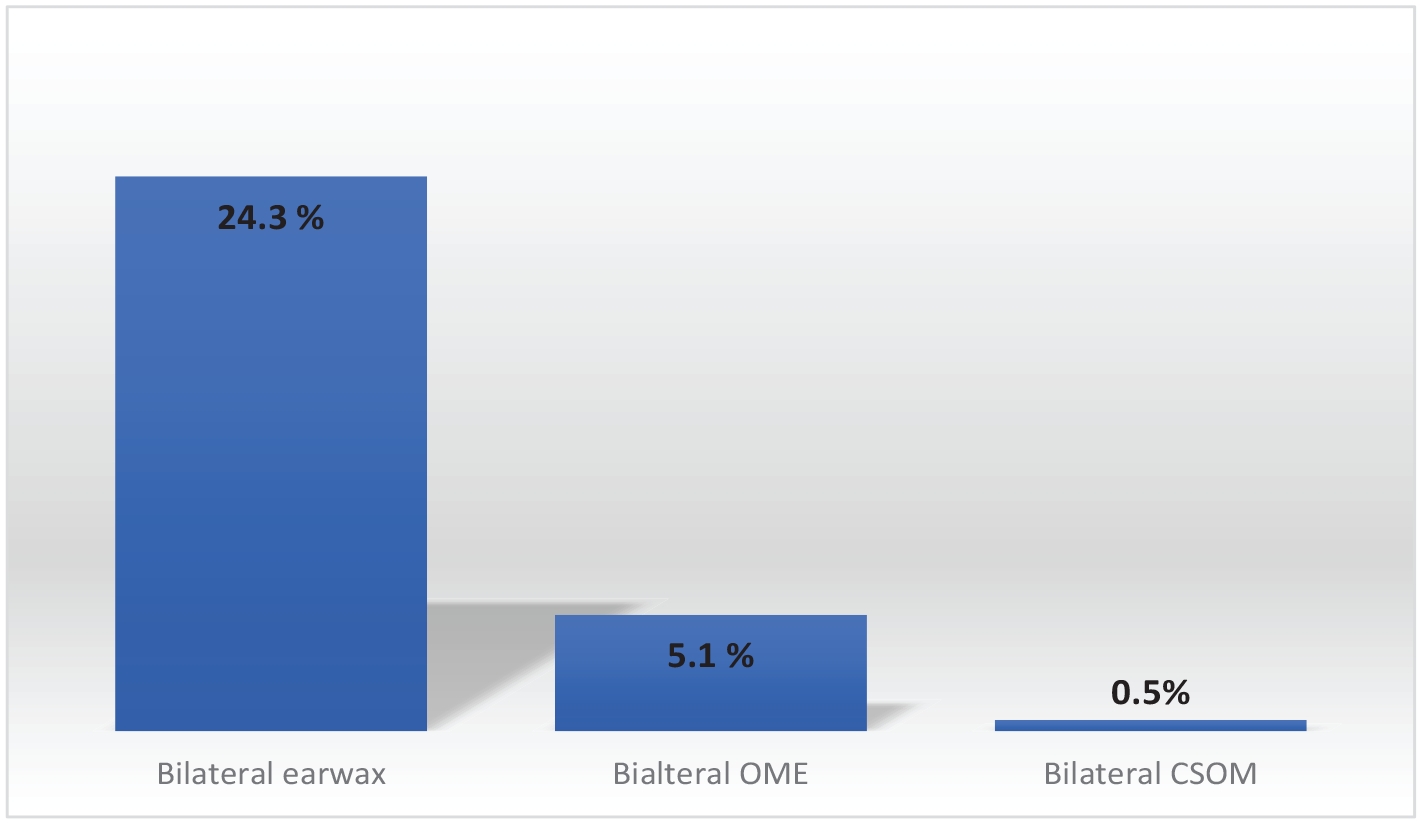
Overview of bilateral ear pathology data.
Summary of Chi-Squared Tests of Significance.
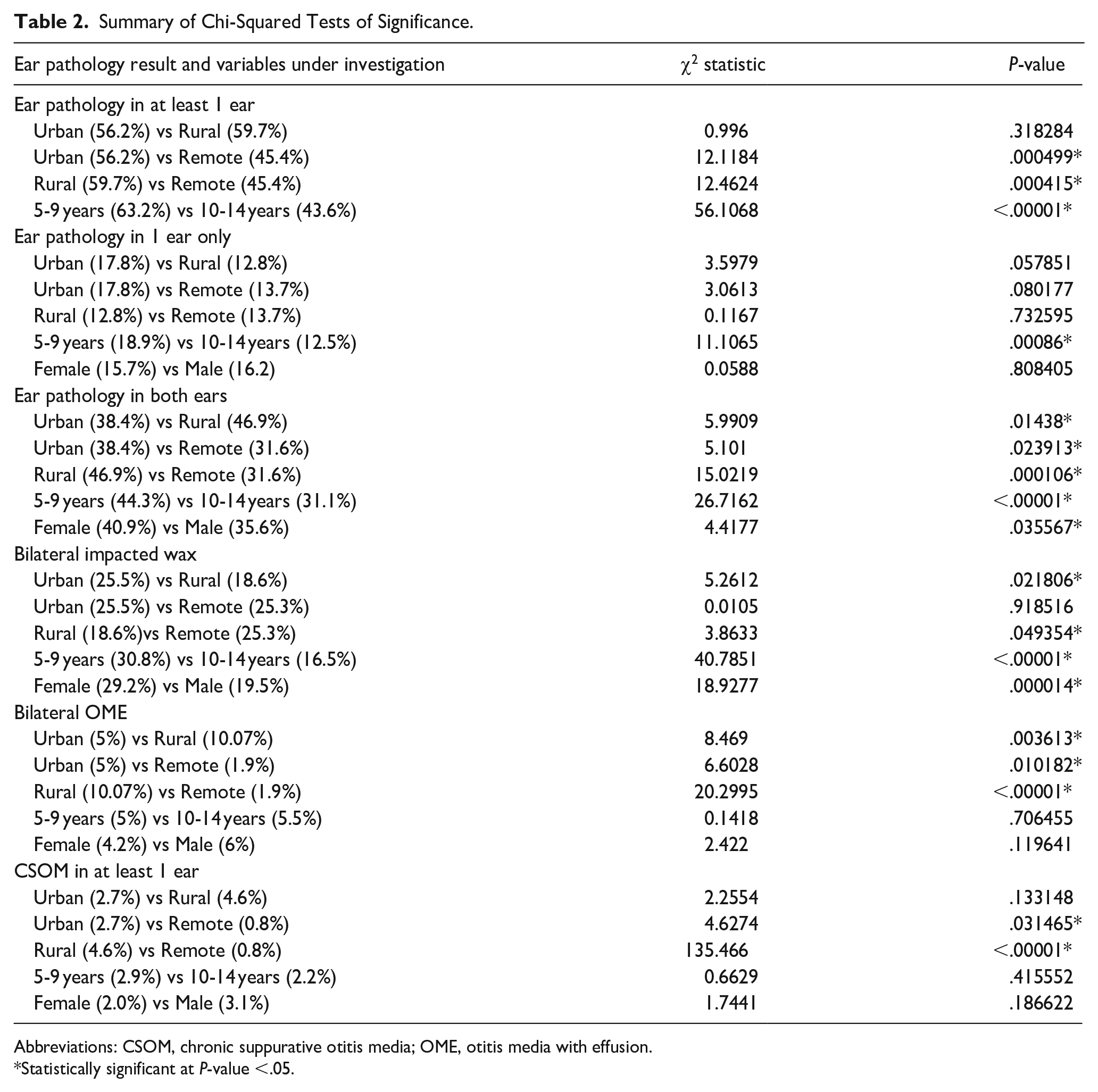
Abbreviations: CSOM, chronic suppurative otitis media; OME, otitis media with effusion.
Statistically significant at P-value <.05.
Bivariate correlation tests revealed that there was a significant association between at student having an ear pathology in at least 1 ear and the location (P = .002) and the age (P < .001) variables, but not for gender (P = .061). Further chi-squared tests of significance found that that the proportion of students with pathology in at least 1 ear was significantly higher in rural (59.7%; P < .001) and urban (56.2%; P < .001) settings than in remote settings (45.4%). There was no significant difference between the rural and urban settings. There was a significantly higher proportion of students in the 5 to 9 age group with ear pathology in at least 1 ear (63.2%) than in the 10 to 14 age group (43.6%; P < .00001).
Bivariate correlation tests revealed that there was a significant association between a student having normal ear examination, pathology in only 1 ear, pathology in both ears, and the location (P = .011), gender (P = .03), and age (P < .001) subgroup variables. Chi-squared tests of significance found that the proportion of students with pathology in both ears was significantly higher in rural settings (46.9%) than either remote (31.6%; P < .001) or urban settings (38.4%; P < .05). There were also significantly more students with pathology in both ears in urban than remote settings (P < .05). There was a significantly higher proportion of female students with pathology in both ears (40.9%) than male students (35.6%; P < .05). There was a significantly higher proportion of 5 to 9 year-old students (18.9%) with ear pathology in 1 ear only than 10 to 14 year olds (12.5%; P < .01), and also higher proportion of 5 to 9 year-old students (44.3%) with ear pathology in both ears than 10 to 14 year olds (31.1%; P < .00001). No significant differences for pathology in 1 ear only, and location and gender subgroups.
Bilateral Impacted Cerumen
Bilateral impacted cerumen was diagnosed for 362 students (24.3%), unilateral impacted wax with no pathology in the opposite ear for 134 students (9%), and unilateral wax with a different pathology in the opposite ear for 53 students (3.5%). Among students with bilateral impacted wax, there was a significant difference in prevalence rates between location, gender, and age variables. There were significantly higher proportion of students with bilateral impacted wax living in remote (25.3%; P < .05) and urban settings (25.5%; P < .05) than those living in rural settings (18.6%), and no significant difference between remote and urban settings. There were significantly more female (29.2%) than male (19.5%) students with bilateral impacted wax (P < .01). The proportion of 5 to 9 year-old students (30.8%) with bilateral wax was significantly higher than 10 to 14 year-old students (16.5%; P < .00001).
Following cerumen removal and re-examination of the affected ear (n = 549), additional ear pathology was able to be diagnosed in 30 (5.46%) of right ears and 27 (4.9%) of left ears. The most common pathology was OME, which was diagnosed for 21 right ears and 19 left ears. The remaining diagnoses were foreign bodies (n = 4), dry tympanic membrane perforations (n = 3), ETD (n = 3), otitis externa (n = 1), and AOMwiP (n = 1).
Bilateral OME
Bilateral OME was diagnosed for 77 students (5.1%), unilateral OME with no pathology in the opposite ear for 13 students (0.9%), and unilateral OME with a different pathology in the opposite ear for 23 students (1.5%). Among students with bilateral OME, a significantly higher proportion of students were from rural settings (10.07%) than either urban (5%; P < .01) or remote settings (1.9%; P < .00001). The proportion of students with bilateral OME in urban settings was also significantly higher than those from remote settings (P < .05). There were no significant differences in bilateral OME proportions for either the gender or age variables.
Chronic Suppurative Otitis Media
CSOM was diagnosed for 39 students (includes students diagnosed with CSOM in either one or both ears). Chi-squared tests showed that the proportion of students diagnosed with CSOM in at least 1 ear was significantly lower in remote settings (0.8%) than either urban (2.7%; P < .05) or rural settings (4.6%; P < .00001). There was no significant difference in proportions of students with CSOM between urban and rural settings. There was no significant difference in CSOM proportions based on gender or age group variables.
Further Invention Following the School Outreach Visits
Following the ENT clinic visit, 1180 students (79%) required no further intervention, mostly due to the successful intervention by the ENT nurses of wax removal (n = 425) and foreign body removal (n = 43). The remaining cases consisted of students with ETD secondary to an upper respiratory tract infection, as well as 2 cases of unilateral atresia who were advised that surgical options will be investigated once the child is older (ie, for review by a visiting ENT Surgical Team to Samoa which should include audiology assessment).
Following the ENT clinic visit, 311 students (21%) required further intervention. This consisted of students referred for primary health care (15%) for management of AOM or wax removal following application of coconut oil, and students referred to the ENT Clinic (6%) for management of CSOM, possible myringoplasty surgery for dry tympanic membrane perforations, and possible myringotomy or grommet insertion for bilateral OME.
Discussion
This study found that more than half (54.3%) of primary school students in Samoa required ENT intervention for an ear pathology in at least 1 ear, and usually for both ears. This is similar to the findings from the Solomon Islands where 56.6% of primary school students did not pass their ear examination in at least 1 ear. 11 The most common pathology in our Samoan population was overwhelmingly impacted cerumen (36.8%), followed by OME (7.5%). This differs from the Solomon Islander study where the leading pathology was OME (34.2%), followed by impacted cerumen (22.8%). Among students with impacted wax in at least 1 ear, a further diagnosis of OME was made following cerumen removal for 5.46% right ears and 4.9% left ears, similar to results from the Solomon Islands (7.61%). The prevalence of CSOM between the Samoan (2.6%) and Solomon Islander (3.1%) studies were similar, and both fall within the WHO definition of “an avoidable burden of disease that must be addressed” (ie, CSOM prevalence of 2%-4%). 24
The Solomon Islander study was based in the capital city Honiara, while the Samoan study extended the research literature for the Pacific Islands by including primary school students from urban, rural, and remote settings. Audiology literature from low- and middle-income countries has long acknowledged significantly higher prevalence rates of ear disease in rural/remote settings in comparison to urban counterparts, and usually attribute this to a combination of factors including lower socioeconomic status and lack of access to health services.25-28 Although this study found that location was a significant variable for the prevalence and pattern of ear disease among our students in Samoa, there were some contrasting results with the established literature. In contrast to findings from other low-middle income nations, the prevalence of ear pathology in at least 1 ear was similar in the rural and urban settings of Samoa. Again, in contrast to the literature, prevalence of ear disease was significantly lower in our remote (Savai’i) setting compared to the urban (Apia) and rural (Upolu) settings: this was true for the proportion of students with pathology in at least 1 ear, pathology in both ears, bilateral OME, and CSOM in at least 1 ear. Anecdotally, based on conversations during professional collaborations between ENT Specialists in the Pacific Islands and overseas (ie, Australia and New Zealand), this may be explained by the fact that children in Savai’i swim in clean ocean water almost every day, thereby reducing their risk of ENT infectious diseases (ie, they are essentially undergoing a full body “saline wash”).
Age was a significant variable in this study, with ear pathology diagnoses more prevalent among younger (5-9 years) than older (10-14 years) students. This is similar to the results from the Solomon Islands. For students with bilateral impacted wax, age was a significant factor in our Samoan population, with impacted wax significantly more common among the younger than the older students, similar to the findings from the Solomon Islands. For students with bilateral OME, age was not a significant factor in our Samoa population (ie, it was equally common among our younger and older students), which differed from the Solomon Islander study where bilateral OME was significantly more common in the younger age group. Age was not investigated as a significant variable for CSOM diagnosis in the Solomon Islander study; however, our findings from Samoa found that again there was no significant difference between age groups for CSOM diagnosis (ie, it was equally common among the younger and older students).
Gender was also a significant variable in this study, with more female students diagnosed with ear pathology in at least 1 ear than male students. This differs from the Solomon Islander findings where gender was not a significant variable to ear pathology diagnosis. Given that bilateral impacted wax was overwhelmingly the most common pathology in our population, it was unsurprising to find that bilateral impacted wax was therefore significantly more common among female than male students. A possible explanation for the significance of gender on the present results may be that female students are more attentive to personal care, whether of their own initiative or their carers’, and, therefore, cotton buds are used more regularly as a personal grooming routine for the ears. It is noted that gender was not a significant variable for OME or CSOM diagnosis.
Given that impacted wax is overwhelmingly the most common ear pathology (36.8%) in our Samoan primary school population, the further development of school-based health programs should consider the inclusion of (1) health education on eliminating the use of cotton buds, as well as (2) a staff member skilled in cerumen removal. Impacted wax often causes a mild to moderate degree of hearing loss, which may be classified as an educationally disabling hearing loss. 29 Reducing the prevalence of impacted wax among our primary school students should positively impact not only their ear health, but optimize hearing levels for their learning and academic achievement. This is an option to be explored as Samoa aims to strengthen the school-based component of their national public health initiative PEN Fa’aSamoa.21,22
Cerumen removal is one of the leading skills the ENT clinic would like to improve among our colleagues working in primary care settings across the whole country, and the ENT clinical staff regularly facilitate WHO Primary Ear and Hearing Care workshops to achieve this goal. 30 Anecdotally, again based on conversations during professional collaborations between ENT Specialists in the Pacific Islands and overseas (ie, Australia and New Zealand), impacted wax is thought to be prevalent among both children and adults in Samoa not only due to the use of cotton buds but also due to the coral-shell-based dust in the environment, which enters the ear canals and contributes to hardening of cerumen and preventing its natural expulsion from the ears.
The results of this study should also facilitate greater collaboration with the Health Promotion Unit of the Ministry of Health. Changing mindsets about the use of cotton buds is a goal that may be achieved through well-planned health promotion activities, ultimately leading to health behavior changes that should reduce the prevalence of impacted cerumen among both children and adults. Health promotion activities should also include general health and well-being advice (ie, nutrition, hygiene, and hand-washing) that should not only reduce infectious ear pathology but also reduce the number and severity of precipitating upper respiratory tract infections.
The results of this study should also encourage current efforts to fully transition to a national digitally based health information system. The inclusion of school ear health examination data in the Tamanu Health Information System would facilitate future prevalence and pattern surveys of this kind, including monitoring and evaluation studies.
Limitations
This study was a retrospective review of clinical records of school outreach visits, and therefore limited by the inherent features of this chosen research design. An epidemiology study with a prospective design and stratified cluster-sampling would be beneficial in the future and address limitations such as appropriate regional representation and the inclusion of children who may not be attending school.
A greater sample size over the 2-year study period would have been desirable; however, the ENT Clinical outreach visits were dependent on key staff availability and competing priorities. This limitation serves to underscore the fact that ear health cannot be the sole responsibility of the ENT Clinic, and that indeed strengthening our existing primary and public health care services is the best and most cost-effective strategy for reducing the prevalence of ear disease and associated hearing loss among our primary school students.
Conclusion
Impacted cerumen is a significant issue among the primary school students of Samoa, and future school-based health services should include a team member skilled in cerumen removal. The prevalence of CSOM suggested an avoidable burden of disease that must be addressed.
Footnotes
Acknowledgements
We wish to thank the following ENT Clinic staff members, both past and present, who participated in the ENT Clinic outreach visits: Zeming Fu (Visiting ENT Specialist), Ferila Figao (RN), Mesepi Fotu (RN), Abraham Fatupaito (RN), Marjorie Liaga (RN), Annie Lilo (RN), Serita Mealoi (RN), and Juanita Collins (RN).
Author Contributions
Annette Kaspar: Conceptualization, Data Curation, Formal Analysis, Investigation, Methodology, Project Administration, Visualization, Writing – original draft, Writing – review and editing. Sione Pifeleti: Investigation, Writing – review and editing. Carlie Driscoll: Formal analysis, Supervision, Validation, Writing – review and editing. Maria Ah Kuoi: Investigation, Writing – review and editing.
Data Statement
Requests for data may be made to the corresponding author and are subject to approval from the Government of Samoa Health Research Ethical Committee. This is a condition of the approval to publish this research findings.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval and Informed Consent Statement
Ethical approval for this study was granted by the Health Research Ethics Committee of the Government of Samoa Ministry of Health, including approval to publish. Approval was also granted by the Government of Samoa Ministry of Education, Sports & Culture, as well as the University of Queensland Health and Behavioural Sciences, Low & Negligible Risk Ethics Sub-Committee (Approval Number: 2020000255). Gatekeeper approval was also obtained from the participating schools during the ENT Clinical outreach visits. The study design was a retrospective review of de-identified clinical records and informed consent was not required.