
Abstract
Chronic cough is a common troublesome symptom in otolaryngology head and neck surgery practice. In rare cases, chronic cough may be related to anatomical abnormalities. In this article, we report the history of a 64-year-old female with a chronic course due to a curved superior cornu of the thyroid cartilage and related irritation of the laryngeal superior nerve. The cough was atypical and resolved after the surgical resection of the abnormal cornu. There was no recurrence at 9 months post-surgery. The findings of the present case report highlight the need to explore the laryngeal anatomy in patients with chronic cough to identify potential abnormalities, which may be treated surgically.
Introduction
Chronic cough is defined as a cough lasting longer than 8 weeks. Chronic cough concerns 9% to 33% of patients from Western countries. 1 The most prevalent upper airway causes of chronic cough include laryngopharyngeal reflux, allergy, chronic rhinosinusitis, asthma, and nonasthmatic eosinophilic bronchitis. 2 However, the practitioners do not identify the cause in up to 42% of cases. 3 In this article, we report the history of a female who developed a chronic cough related to an uncommon anatomical laryngeal abnormality.
Case Report
A 64-year-old female was referred to the Division of Laryngology and Broncho-esophagology of EpiCURA Hospital for a history of chronic cough, mild dyspnea, and globus sensation lasting for 18 months. The patient reported a mild-to-moderate coronavirus disease infection 2 weeks before the development of the symptoms. The infection was characterized by nasal and throat symptoms without pulmonary findings. The medical and surgical history was unremarkable. She had no trauma, no allergy, and she did not smoke. The patient had consulted several otolaryngologists and pulmonologists who excluded the most common etiologies, that is, asthma, nonasthmatic eosinophilic bronchitis, obstructive, or restrictive lung disorders. The lung volume evaluations and chest and neck computed tomography (CT) scans were normal. The patient did not have laryngopharyngeal reflux disease at the impedance-pH monitoring. At the nasofibroscopic examination, the left superior cornu of the laryngeal thyroid cartilage appeared to touch the laryngeal posterior commissure (Figure 1), which was associated with an uncommon cough sound (Supplemental Video 1). The patient received several empirical medical treatments (eg, inhaled corticosteroids, bronchodilators, clarithromycin, sodium alginate, and neuromodulators) without symptom relief. The origin of the cough was suspected to be an irritation of the external branch of the superior laryngeal nerve by the superior cornu of the thyroid cartilage. The patient underwent the surgical resection of the left superior cornu through an open surgical approach. The steps of the surgery included a lateral neck skin incision (4 cm), the dissection of tissue to control the vessels (jugular vein, Faraboeuf trunk, and carotid artery), the dissection of the lateral part of the larynx, the identification of the sternohyoid and thyrohyoid muscles, the palpation of the hyoid bone and the superior cornu of the larynx, and the resection of the cornu.
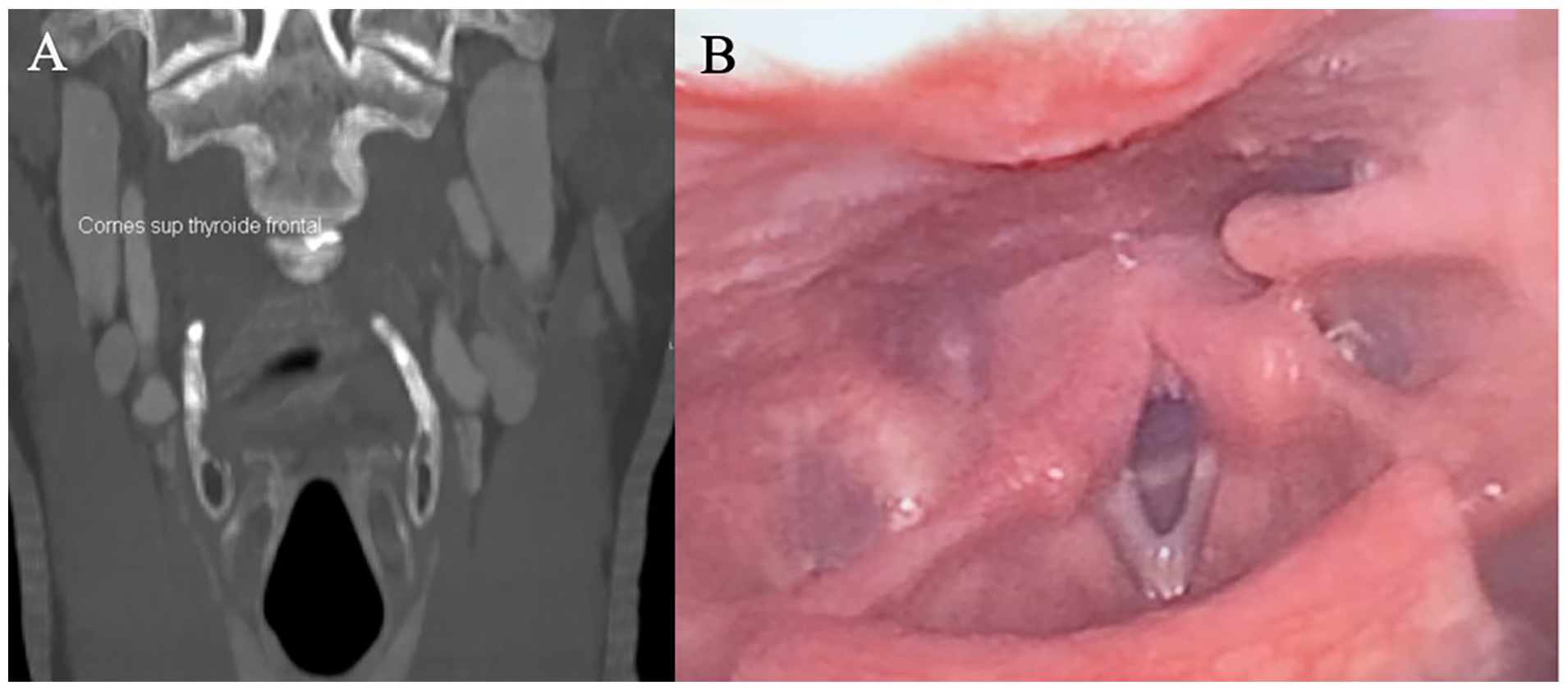
Nasofiberoptic and imaging findings of the patient. (A) The CT scan supported that the abnormality concerned the laryngeal superior cornu, which was incurvated into the median plane. (B) The nasofibroscopy and the exploration of the larynx reported an abnormal contact between the left superior laryngeal cornu and the posterior commissure, resulting in an atypical cough noise. CT, computed tomography.
The surgery led to a resolution of cough and dyspnea. There was no recurrence of the cough at 9 months posttreatment.
Discussion
It is well established that chronic cough may be related to some anatomical abnormalities, including tracheoesophageal fistula, laryngeal web, tracheal diverticulum, tracheomalacia, bronchogenic cysts, vascular rings, or other laryngotracheal malformations.4-6 The pathophysiological mechanisms depend on the anatomical malformations. The role of the superior laryngeal nerve has been extensively studied in the development of chronic neurogenic cough in the past decades. The superior laryngeal nerve dysfunction can be related to laryngeal sensory neuropathy, postviral neuropathy, laryngeal hyperresponsiveness, or neurological conditions (Parkinson, stroke, or multiple sclerosis). To the best of our knowledge, the present case is the first to report a chronic cough due to the irritation of the superior laryngeal nerve by a laryngeal cartilage abnormality. In the current literature, we only found one case of globus sensation related to a post-traumatic curved thyroid cartilage superior cornu. 7 In the present case, the neurogenic trigger was the anatomical deformity. The atypical cough noise was attributed to the contact between the superior cornu and the laryngeal posterior commissure tissue (Figure 1). The surgical excision of the superior laryngeal cornu can support the diagnosis because both cough and dyspnea resolved post-surgery. In addition, the noise of the forced cough was normalized after the surgery. While the symptom’s relief after the surgical excision of the superior cornu can support the diagnosis, the timing of the symptom’s development remains an unelucidated point. Indeed, it is probable that the patient had had the anatomical laryngeal abnormality for a long time. Thus, it remains unclear why she developed the symptoms at this time. The primary hypothesis could involve COVID-19, which is suspected to sensitize/injure the mucosa and the nerve endings. 8 Because the COVID-19 infection was characterized by an ear, nose, and throat clinical pattern, it was suggested that the mucosa inflammation had led to an increase in the laryngeal mucosa sensitivity and the development of the neurogenic cough.
Conclusion
The findings of the present case report highlight the need to explore the laryngeal anatomy in patients with chronic cough to identify potential abnormalities, which may be treated surgically.
Footnotes
Acknowledgements
Dr Johnson for proofreading the article.
Author Contributions
J.D., A.B., J.R.L., A.L., S.S.: conception and design, analysis and interpretation of data, drafting of the manuscript; J.R.L., A.L., S.S.: revising the manuscript for important intellectual content, and final approval of the version to be published; A.B., J.D.: conception and design of the manuscript.
Data Availability
NA.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Statement
The institutional review board approval was not required for the publication of this case report. Patient agreed for publishing the case and the informed consent was obtained.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.