
Abstract
Keywords
Introduction
Hearing loss is prevalent among the elderly population, with approximately three-quarters of individuals aged ≥70 years experiencing some degree of hearing impairment in at least 1 ear. 1 While gradual, bilateral, symmetrical sensorineural hearing loss is the most common type observed in the elderly, asymmetrical sensorineural hearing loss (ASNHL) can also manifest in this demographic. In the general UK population, the prevalence of ASNHL was reportedly 1% at ages 18 to 80 years. 2 However, studies using criteria from the American Academy of Otolaryngology-Head and Neck Surgery (AAO-HNS) have estimated the overall prevalence of ASNHL at 4.05% in 0.5 to 4 kHz and 13.97% in 4 to 8 kHz range among individuals aged 60 to 69 years. 3 This indicates a higher prevalence of ASNHL among the elderly compared to younger individuals. 2
The clinical manifestation of ASNHL raises concerns regarding potential retrocochlear pathology, such as vestibular schwannoma (VS) or other cerebellopontine angle (CPA) tumors, necessitating further investigation. While audiological testing methods such as impedance audiometry, auditory brainstem response testing (ABR), and electrocochleography have been used to identify the cause of ASNHL, their utility is often limited to academic institutions. Comparative studies evaluating the accuracy of ABR versus contrast-enhanced magnetic resonance imaging (MRI) in diagnosing retrocochlear lesions have shown a sensitivity of 71% and a specificity of 74%, potentially leading to missed or delayed diagnoses of small intracanalicular tumors. Owing to these limitations, MRI has emerged as the recommended screening test for ASNHL 4 and has become a gold standard, replacing computed tomography or ABR for determining retrocochlear pathology after thorough clinical examination and audiological assessment. However, despite a persistent trend toward increased MRI usage as the initial investigation for ASNHL, MRI is associated with high medical costs with relatively low diagnostic yield in evaluating ASNHL. 5
Elderly patients with ASNHL often present with multiple medical comorbidities, experience prolonged recovery times after investigations, and may not be suitable candidates for aggressive treatment. In addition, postoperative care in this population can pose significant challenges, particularly due to potential contraindications to MRI, such as metallic implants. These factors necessitate a reevaluation of criteria for investigating ASNHL among elderly individuals, as the existing literature lacks sufficient evidence to recommend a standard management approach for this demographic.
Therefore, this study aimed to investigate the differences in clinical characteristics and audiometric patterns among elderly patients having ASNHL with and without CPA tumors.
Materials and Methods
This retrospective study was conducted at Songklanagarind Hospital (a tertiary referral center), Prince of Songkla University, and received approval from the institutional review board at our center. Electronic medical records of patients aged ≥65 years diagnosed with ASNHL between January 2012 and December 2022 were extracted from our center’s Information System database. The definition of ASNHL followed the criteria established by the AAO-HNS 6 and Cueva et al 4 as follows: ASNHL was diagnosed when a difference ≥15 dB in pure tone averages (PTA) at 2 or more frequencies between ears, or a ≥15% difference in speech discrimination existed. An otologic examination was performed on all patients using an otoscope, yielding negative findings. The exclusion criteria encompassed documented histories of ototoxic agent exposure, chronic ear infections, acoustic trauma, intracranial infections, chemotherapy or radiation affecting the head and neck, ear trauma, moderate or severe traumatic head injuries, diagnoses of neurofibromatosis type 2, and any clearly identifiable mechanism of hearing loss.
Demographic and clinical data, including age, sex, presenting symptoms, duration of symptoms, the severity of hearing loss, associated symptoms, cranial nerve deficits, other neurological deficits, and medical comorbidities [eg, hypertension, diabetes mellitus (DM), and dyslipidemia], were recorded. Audiometric data comprised air and bone conduction PTA at frequencies of 0.25, 0.5, 1, 2, 3, 4, and 8 kHz in both ears, speech recognition thresholds, speech discrimination scores, and calculation of PTA differences between ears. ABR results were interpreted by highly experienced audiologists. Abnormalities in ABR were considered significant if (1) the difference in interaural interpeak latencies of wave V exceeded 0.4 milliseconds, adjusted by subtracting 0.1 milliseconds for every 10 decibels (dB) of hearing depletion beyond 50 dB at 4 kHz or (2) the I-V interval exceeded 4 milliseconds or interwave latencies of I-III and III-V exceeded 2 milliseconds. All patients underwent radiological assessments using MRI scans of the temporal bone, interpreted by a highly experienced neuroradiologist. For patients with identified CPA tumors, data on lesion type, tumor size (measured as the maximum diameter in any plane), location, expansion within the internal auditory canal, and treatment were collected. Surveillance imaging with MRI was conducted at 6-month intervals following the initial scan, with subsequent annual scans for 5 years. Tumor growth and patterns thereof were measured by a neuroradiologist. Clinical and demographic data were compared between the groups with normal and abnormal MRI findings.
Statistical Analyses
The statistical software R (version 3.6.2; R Foundation for Statistical Computing, Vienna, Austria) was used to analyze the data. Statistical significance was set at P < .05. Continuous data are described using means with standard deviations or medians with interquartile ranges, and discrete variables are expressed as percentages. Clinical and demographic data were compared between the non-CPA tumor and CPA tumor groups using Pearson’s Chi-squared test, Fisher’s exact test, Wilcoxon rank-sum test, or Student’s t-test, as appropriate.
Results
Demographic and Clinical Data
A total of 284 elderly patients with a first diagnosis of ASNHL were initially identified, and 119 of them met the previously described criteria and were subsequently included in the study. The median age at diagnosis was 71 years (range: 65-89 years), and no significant differences in sex or age were observed between the 2 groups (P = .526, .476, respectively; Table 1). In addition, no difference in the affected side was noted. The mean duration from initial symptom onset to diagnosis was 322.8 days. The most characteristic feature of ASNHL was its gradual onset, with commonly associated symptoms including tinnitus, vertigo, and disequilibrium (see Table 1). Notably, 1 patient presented with facial weakness, which resolved completely within 2 months without evidence of a retrocochlear lesion, and was diagnosed with Bell’s palsy. Patients without tumors had a history of type 2 diabetes in 33.3% of cases, compared to 9.1% in those with CPA tumors (P = .021; Table 1).
Demographic Characteristics of the Included Patients.
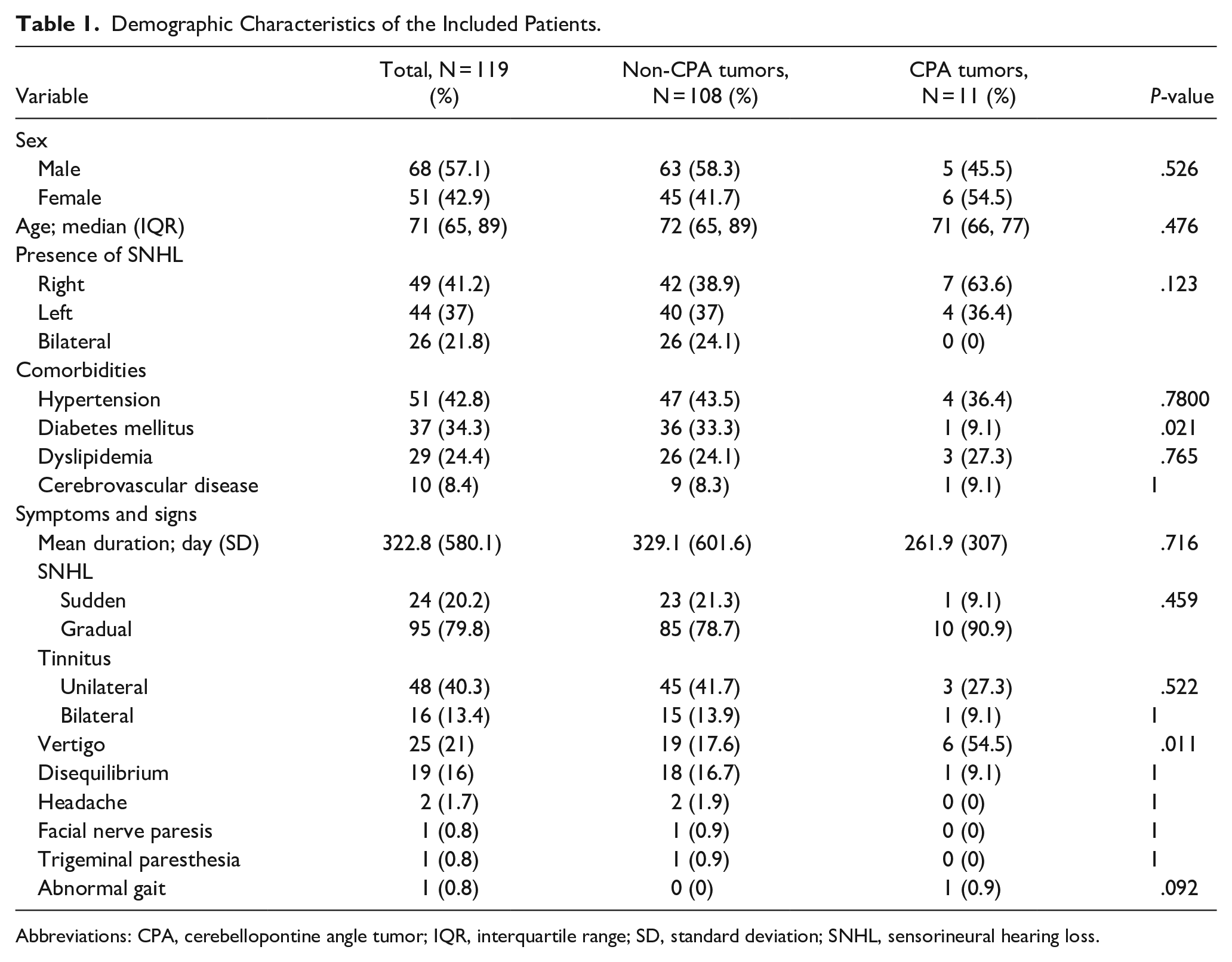
Abbreviations: CPA, cerebellopontine angle tumor; IQR, interquartile range; SD, standard deviation; SNHL, sensorineural hearing loss.
Audiological Assessment Outcomes
Table 2 presents the mean hearing thresholds and the mean asymmetry of hearing loss between patients with and without CPA tumors. No significant differences were observed in either the hearing thresholds or the asymmetry of hearing loss between the 2 groups. In addition, there were no statistically significant differences in the distribution of asymmetries at each frequency between the non-CPA tumor and CPA tumor groups (Table 3). The mean speech discrimination score was 36.8% in the non-CPA tumor group and 45.1% in the CPA tumor group, with no significant difference (P = .431). ABR abnormalities were found in 50 patients. Of them, 42 patients had negative results on the MRI without remarkable pathology. Two patients had normal ABR results but showed small CPA tumors on the imaging. The parameters for assessing the performance of ABR were calculated using a 2 × 2 table. ABR sensitivity was 80%, specificity was 59.6%, false-negative rate was 20%, and false-positive rate was 80%. Negative and positive predictive values of ABR were 86.9% and 16%, respectively.
Mean Hearing Threshold and Mean ASNHL Between Ears Based on Frequency.
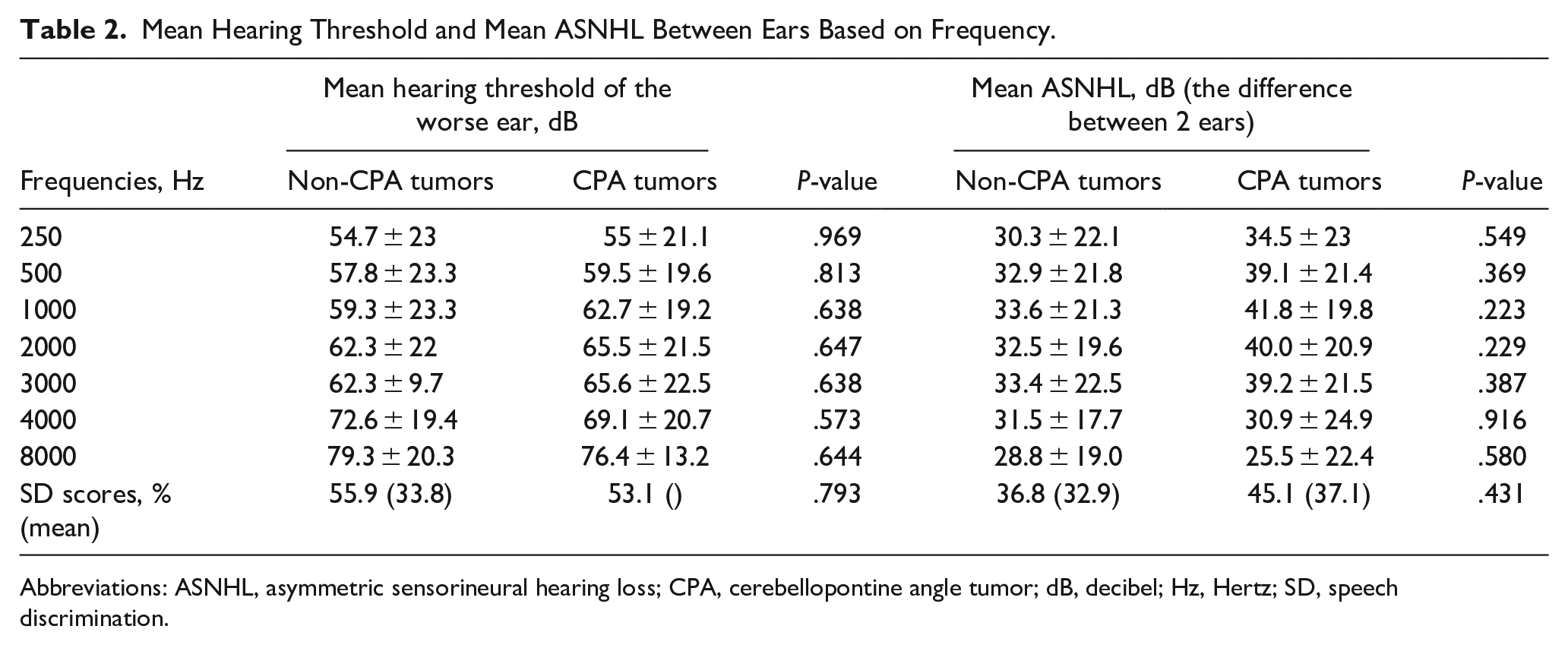
Abbreviations: ASNHL, asymmetric sensorineural hearing loss; CPA, cerebellopontine angle tumor; dB, decibel; Hz, Hertz; SD, speech discrimination.
Hearing Asymmetry Between the Non-CPA Tumor and CPA Tumor Groups.
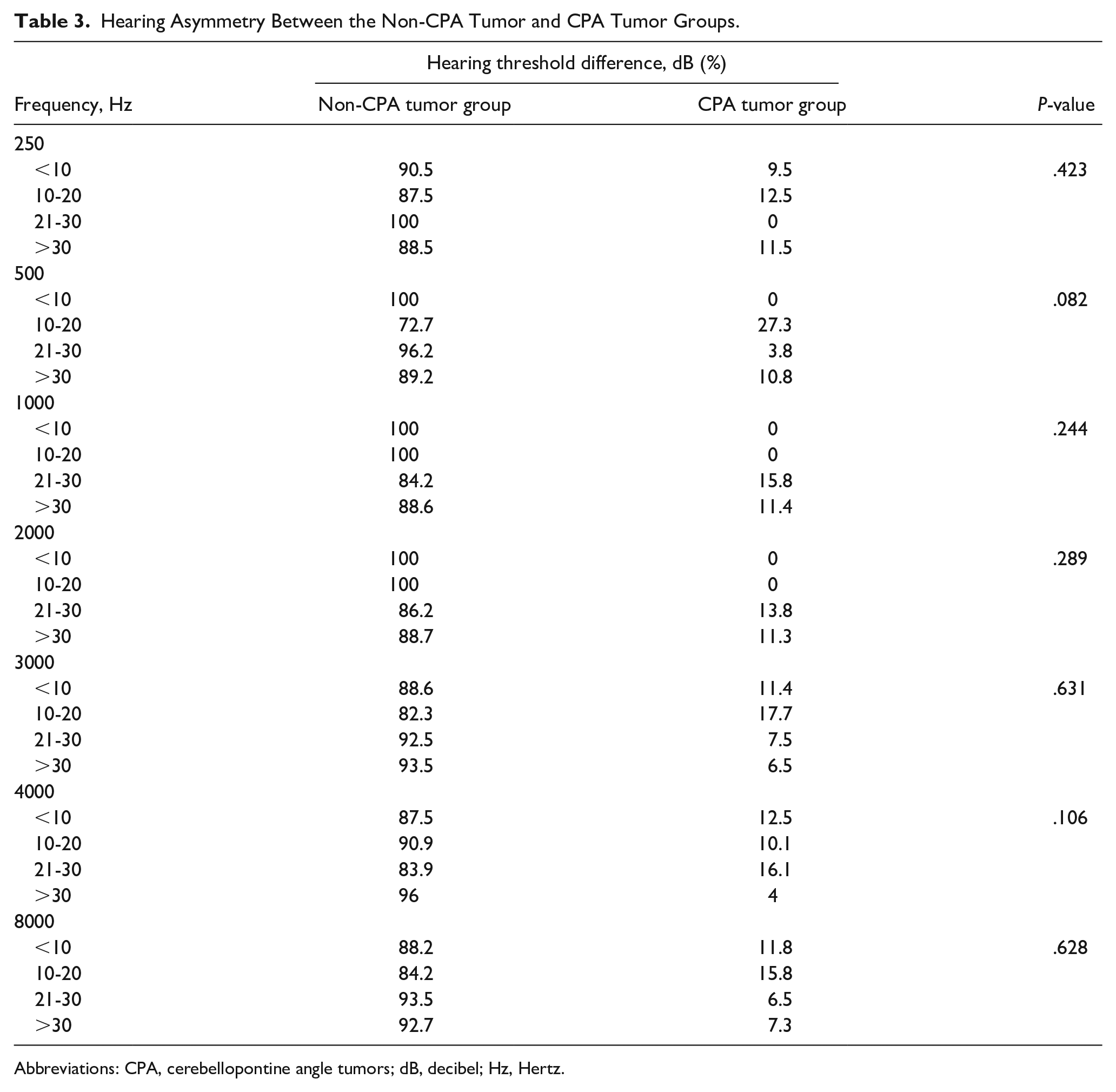
Abbreviations: CPA, cerebellopontine angle tumors; dB, decibel; Hz, Hertz.
Tumor Characteristics
Among the 119 patients, 11 (9.2%) exhibited pathological findings on MRI. The most common abnormality detected was VS in 7 patients (63.6%). Other lesions included 2 meningiomas (18.2%), 1 epidermoid cyst (9.1%), and 1 arachnoid cyst (9.1%). One patient with meningioma did not undergo follow-up after the initial diagnosis. Among patients with VS, the mean average annual growth rate was 0.53 mm/year (range: 0-1.33 mm/year), with 1 patient exhibiting a reduction in tumor size on subsequent MRI surveillance. One patient exhibited VS extension beyond the internal auditory canal, whereas the remaining cases were confined within the intracanalicular tumors. The mean follow-up period for this group was 62.3 months (range: 29-110 months), with 9 patients opting for conservative treatment through observation with serial MRI testing, and 1 patient undergoing surgery.
Discussion
The management of patients with ASNHL remains debatable, with no consensus on optimal protocols and cost-effectiveness. The increasing utilization of MRI in patients with ASNHL has resulted in the identification of a growing number of retrocochlear pathologies. The prevalence of ASNHL in elderly individuals has progressively increased, 3 likely due to improvements in healthcare accessibility and longer life expectancies, posing challenges in the appropriate management of elderly individuals with ASNHL and ruling out vital CPA tumors. Screening criteria for elderly individuals need to be developed to select patients with ASNHL who should undergo radiologic assessment, as performing an MRI evaluation in aging patients is expensive, time-consuming, and may be challenging due to medical conditions or claustrophobia.
We identified vertigo as the only symptom associated with the presence of CPA tumors. This finding is consistent with that of Ahsan et al, 7 who found that dizziness/vertigo in ASNHL could increase the diagnostic yield of MRI testing. Myrseth et al 8 also indicated that unsteadiness related to a tumor size of >20 mm was associated with vertigo, consistent with previous studies on the conservative management of VS, which found that tumor growth was related to vertigo. 9 Various causes of vertigo accompanied by ASNHL, such as posterior circulation stroke, VS, posterior fossa tumors, or labyrinthine infarction, 10 highlight the importance of further assessment in aging patients with ASNHL presenting with vertigo to reduce the risk of dangerous misdiagnosis of serious medical conditions.
Moreover, there is considerable disparity among previous results regarding the clinical manifestation of tinnitus with ASNHL as a predictive factor for CPA tumors or tumor growth.11-14 Choi et al 13 reported a low incidence of retrocochlear pathology in patients with tinnitus and ASNHL. Judicious use of radiological assessment is suggested in patients with ASNHL and tinnitus according to clinical practice guidelines on tinnitus. 14 However, we found that tinnitus did not significantly predict CPA tumors in elderly patients with ASNHL. The etiology of tinnitus in the elderly is often associated with age-related hearing impairment, making it difficult to differentiate between tinnitus caused by aging and other pathological causes. Furthermore, previous studies on the presentation of tinnitus with retrocochlear pathology did not focus on differences across younger age groups and the elderly.11-14
VS is one of the most common CPA tumors, with an average tumor growth rate of 0.99 to 2 mm/year.12,15,16 Several studies have evaluated age as a predictor of VS growth with inconsistent results. However, some studies of VS in elderly patients have shown a tendency for slower growth rates and smaller sizes compared to younger patients.11,16,17 Consistent with our findings of an average growth rate of only 0.53 mm/year in elderly patients undergoing MRI based on presenting with ASNHL and without focal neurological deficits, conservative management is suitable for use due to the potential for medical comorbidities and delayed recovery after intervention in elderly patients. Previous literature supports surveillance protocols for a minimum of 4 to 5 years, with the risk of growth after 5 years falling to less than 2%.18,19
Notably, in this study, the prevalence of CPA tumors was significantly lower in patients with DM and ASNHL than in those without DM. Many studies have revealed a higher prevalence of sensorineural hearing loss in patients with DM.20-22 The potential mechanism by which ASNHL manifests in patients with DM is as follows: hyperglycemia results in diabetic microangiopathy and stria vascularis or outer hair cell degeneration, altering the morphology of the cochlea 23 ; this is a part of the natural course of DM and may affect hearing acuity.22,24 In addition to cochlear changes, DM can also cause degeneration of auditory nerve fibers, resulting in neural hearing loss (diabetic neuropathy). 25 Furthermore, elderly patients with DM have a higher incidence of hearing loss, particularly at 6000 to 8000 Hz.26,27 Vu et al 28 reported that the chances of abnormal MRI findings are slightly lower for hearing loss at 6 kHz. Moreover, the severity of sensorineural hearing loss in patients with DM correlates with the increasing ages of these patients, blood sugar levels, and DM duration and severity.20-22 Thirty diabetic patients in the non-CPA group had abnormal ABR recording, consistent with the findings reported by Sheikhzadeh et al, 29 who showed that the absolute latency of wave III and the interpeak latency (IPL) of waves I to III, which measured the conduction time from the auditory nerve to the cochlear nucleus, was higher in the diabetic patients. Previous research has revealed that diabetic patients, even with normal hearing, can have prolonged absolute wave latency and IPL with abnormal Distortion product otoacoustic emissions (DPOAE) results due to diabetic neuroangiopathy. 30 Therefore, elderly patients with ASNHL and DM should be initially managed by thoroughly reviewing the clinical DM information to evaluate the effects of DM on progressive hearing loss as well as annually monitoring other associated neurological symptoms and signs that can help physicians precisely differentiate between benign lesions and life-threatening conditions. The rapidly emerging type 2 DM epidemic and the possibility of patients with DM meeting the ASNHL criteria is high, and decreasing the number of MRI scans with negative results should be considered. Several studies have revealed that cardiovascular risk factors, including hypertension and dyslipidemia, adversely affect hearing status31-33; nevertheless, in our study, we could not demonstrate an association between these risks as a clinical predictor of CPA tumors. Furthermore, using multivariate analysis, Oh et al 27 reported hypertension as an insignificant predictor of hearing loss in elderly individuals.
Many studies have indicated that the criteria for audiometric characteristics should be defined to consider MRI for diagnosing retrocochlear pathologies.7,34 However, in the present study, no significant differences were observed in the audiometric patterns between patients with and without CPA tumors in terms of the interaural mean hearing threshold or interaural mean asymmetry based on frequency. Saliba et al 34 reported that “Rule 3000” is a more reliable universal referral guide for detecting abnormal MRI results in individuals with ASNHL, with sensitivity and specificity of approximately 73% and 76%, respectively; however, it is challenging to apply it to the elderly to detect isolated ASNHL of ≥15 dB at 3 kHz because the aging process may produce hearing loss at multiple high frequencies; in contrast, significant losses are limited or loss may be observed at lower frequencies and specific frequencies for younger patients. Notably, no specific audiometric characteristic can be used as a predictor of CPA tumors in elderly patients. Although in our study, the sensitivity of ABR was 80%; the specificity was 59.6%, which is low. Furthermore, although ABR has a high sensitivity, it also has a high false-positive rate, with a large proportion of the cases (42/104) showing abnormal ABR and negative MRI findings. This may be because age-related changes in the central auditory pathway affect abnormal ABR findings, including increasing absolute wave latency and interpeak intervals,35,36 degeneration of the cochlear nerve, for example, caused by a viral infection as well as “probable age-related auditory neuropathy” (PARAN).37,38 Although auditory neuropathy is commonly considered in infants in which abnormal ABR with preserved outer hair cell functions are observed, 7 it can occur in the elderly, a phenomenon known as PARAN. PARAN was first described in 2003 37 and later defined with the findings of poor SD scores and abnormal ABR but normal MRI in elderly patients. 39 Specifically, PARAN may involve dysfunction in spiral ganglion cells and afferent inner hair cells synapses or auditory nerves in elderly37,40 which affect abnormal ABR findings as a neural ABR-pattern, including increased absolute wave latency and interpeak intervals. These aspects make ABR a low-yield screening tool for ASNHL in elderly individuals. Although 42/104 cases in the present study could be considered PARAN based on the earlier definition, our findings showed no statistically significant correlation between SD scores and ABR latencies. Therefore, the explicit conclusion regarding the correlation between SD scores and ABR latencies in PARAN warrants further studies with larger sample sizes. ABR and MRI tests are available to identify non-CPA or CPA tumor groups with ASNHL. Although imaging with MRI is certainly superior to ABR for diagnosing patients with CPA tumors, we believe that ABR findings are helpful in patients who are contraindicated for MRI evaluation. ABR findings could be used for diagnostic criteria in the PARAN group with abnormal ABR but normal MRI.
We hypothesize that the criteria for ASNHL in elderly patients can be optimized by combining clinical data for vertigo and non-DM in ASNHL, increasing suspicion and warranting further MRI investigation. Using these criteria would not only decrease the number of MRI referrals but also avoid the risk of missed diagnosis of CPA tumors.
Our study has some limitations. First, its retrospective nature made it impossible to collect all clinical information. Second, the non-CPA group showed abnormality in the ABR recording. Determining ABR abnormality in the elderly with ASNHL requires more prospective investigation and clinical correlation data to prevent hearing loss progression. Third, selection bias was present because not all elderly patients with ASNHL underwent imaging and a limited number of patients completed health screening; additional prospective studies with a higher number of patients will help elucidate this problem. Moreover, additional studies should be conducted to investigate the long-term consequences of conservative treatment for ASNHL in elderly individuals to develop guidelines for managing this condition.
Conclusion
In our study, we observed that ASNHL with vertigo was significantly associated with CPA tumors in elderly patients. For such patients, radiological assessments should be performed. Furthermore, abnormal MRI findings were less likely in patients with ASNHL and DM, suggesting that clinical observation with serial follow-up may be considered for these patients because of the low diagnostic yield of MRI. Finally, our findings indicate no differences in the audiometric characteristics of elderly patients having ASNHL with and without CPA tumors.
Footnotes
Acknowledgements
Author Contributions
Yuvatiya Plodpai: Conception, design, and supervise the study, data analysis and interpretation, manuscript editing, corresponding author, and final approval of the study. Kittisak Thepwongsa: Data collection and analysis, and final approval of the study.
Data Availability Statement
Data supporting this study will be available on request at the data owner’s repository via
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Faculty of Medicine, Prince of Songkla University, Thailand, the funding organization had no role in the design or conduct of this research.
Ethics Approval
The institutional review board of the Faculty of Medicine, Prince of Songkla University approved this study.