
Abstract
Introduction
Vestibular-evoked myogenic potential (VEMP) is used to assess the functioning of the otolithic organs in the vestibular system using an acoustic stimulus. It is a short latency potential which is evoked either from the sternocleidomastoid muscle (known as cervical VEMP or cVEMP) or from the inferior oblique muscle (known as ocular VEMP or oVEMP). 1 The cVEMP assesses the integrity of sacculo-collic reflex pathway and oVEMP assess that of utriculo-ocular reflex pathway. VEMPs are typically performed in air conduction mode; however, it has significant limitations. Additionally, when exposed to air conduction stimuli, individuals with conductive hearing loss or air-bone gaps (ABG) may not elicit VEMPs. The literature reported VEMPs elicited by both air-conducted stimulus (AC-VEMP) and bone-conducted stimulus (BC-VEMP). VEMPs (cVEMP and oVEMP) is also used in cases of benign paroxysmal positional vertigo and in differential diagnosis of utricular and sacular involvement in cases of vestibular pathologies. 2
Otosclerosis, also called otospongiosis, is a gradual primary bone ailment of the otic capsule. It involves abnormal localized resorption and subsequent recalcification of the endochondral layer of the temporal bone. It may lead to conductive loss, usually a progressive type which in severe cases can eventually result in a mixed hearing loss. 3 There are 2 main types of otosclerosis namely the Fenestral otosclerosis and the Retrofenestral otosclerosis. Fenestral otosclerosis primarily affects the region anterior to the oval window near the fissula ante fenestram. Involvement of the stapes footplate in this condition leads to stapes fixation, resulting in conductive hearing loss. When the disease progresses beyond this region to involve the pericochlear otic capsule, it is referred to as retrofenestral otosclerosis. However, there is variability in the definitions and their use in the literature, particularly regarding whether round window involvement is considered fenestral or retrofenestral. Due to this variability, some researchers prefer to use the terms “fenestral otosclerosis” and “cochlear otosclerosis” to avoid ambiguity. 4 Cochlear otosclerosis is characterized by progressive sensorineural hearing loss and persistent balance issues. 5 Otosclerosis shows a higher occurrence in women compared to men and women also seem to be notably more susceptible to experiencing vestibular symptoms. Additionally, deafness escalates with age, and as deafness progresses, there is a greater degree of cochlear involvement. 6
Vestibular symptoms have been documented in up to 40% individuals with cochlear otosclerosis. 7 The involvement of vestibular system in patients with otosclerosis can be due to the coexistence of endolymphatic hydrops. This may occur due to extension of otosclerotic lesions into the endolymphatic duct or sac, leading to malabsorption of fluid. Another potential scenario involves the direct intrusion of otosclerotic lesions into the saccular macula or its afferent nerves. 8 A temporal bone study found that there is an overall reduction in the number of vestibular neurons due to the otosclerotic damage to the dendritic fibers in the cribrose areas, which is responsible for the vestibular symptoms experienced in some otosclerotic patients. 9 Otosclerosis primarily impacts the conductive system; hence, numerous studies have utilized bone-conducted stimuli to elicit VEMPs. Due to the typical balance disturbances experienced by individuals with otosclerosis, VEMP findings often indicate abnormal responses, which can vary depending on factors such as the severity of the condition and any surgical interventions performed. The aim of this systematic review is to explore the VEMP findings in patients with otosclerosis.
Methods
The present systematic review followed the Preferred Reporting Items for Systematic Reviews and Meta-Analysis (PRISMA) 2020 guidelines. 10
A literature search was conducted on VEMP findings in otosclerosis patients using PubMed, Scopus, and Cochrane databases to find relevant papers published within the past 2 decades. In total, 199 hits were obtained across all the databases. After eliminating duplicates, 176 studies were retained. Following title screening and abstract screening, 14 studies were selected for full-text review and all studies were including in the for the review. Two independent authors screened the title and abstract. The full text was extracted by the first author, and if there was any disagreement, it was resolved by discussion between coauthors.
The keywords “vestibular evoked myogenic potential,” “VEMP,” and “otosclerosis” which were combined using appropriate Boolean operators such as “AND” and “OR” was used for the search. Additional filters applied was language filters (English).
The following inclusion criteria was used:
- Articles that incorporated VEMP findings in patients with Otosclerosis;
- Articles including any type of VEMP;
- Studies in English language.
Exclusion criteria
- Articles reporting vestibular tests other than VEMP.
- Case reports & letter to editor
A customized data extraction form was created for the purpose of this review based on the aim of the review and discussion among the authors. The following information was extracted from the included studies: authors names, publication year, study design, participants, type of VEMP, outcome measures, and findings related to VEMP.
Information extracted from the studies encompassed details such as the author names, publication year, study design, participants, type of VEMP, outcome measures, and findings related to VEMP.
Quality Appraisal of the Included Study
Mixed Method Appraisal Tool (MMAT) version 2018 was used for the quality assessment of the included studies. 11
Results
The initial search from PubMed, Scopus, and Cochrane database yielded 199 hits. Eighteen abstracts were screened for the eligibility, total 14 article was included for the review which met the inclusion criteria. The steps followed is represented by PRISMA flowchart as depicted in Figure 1.
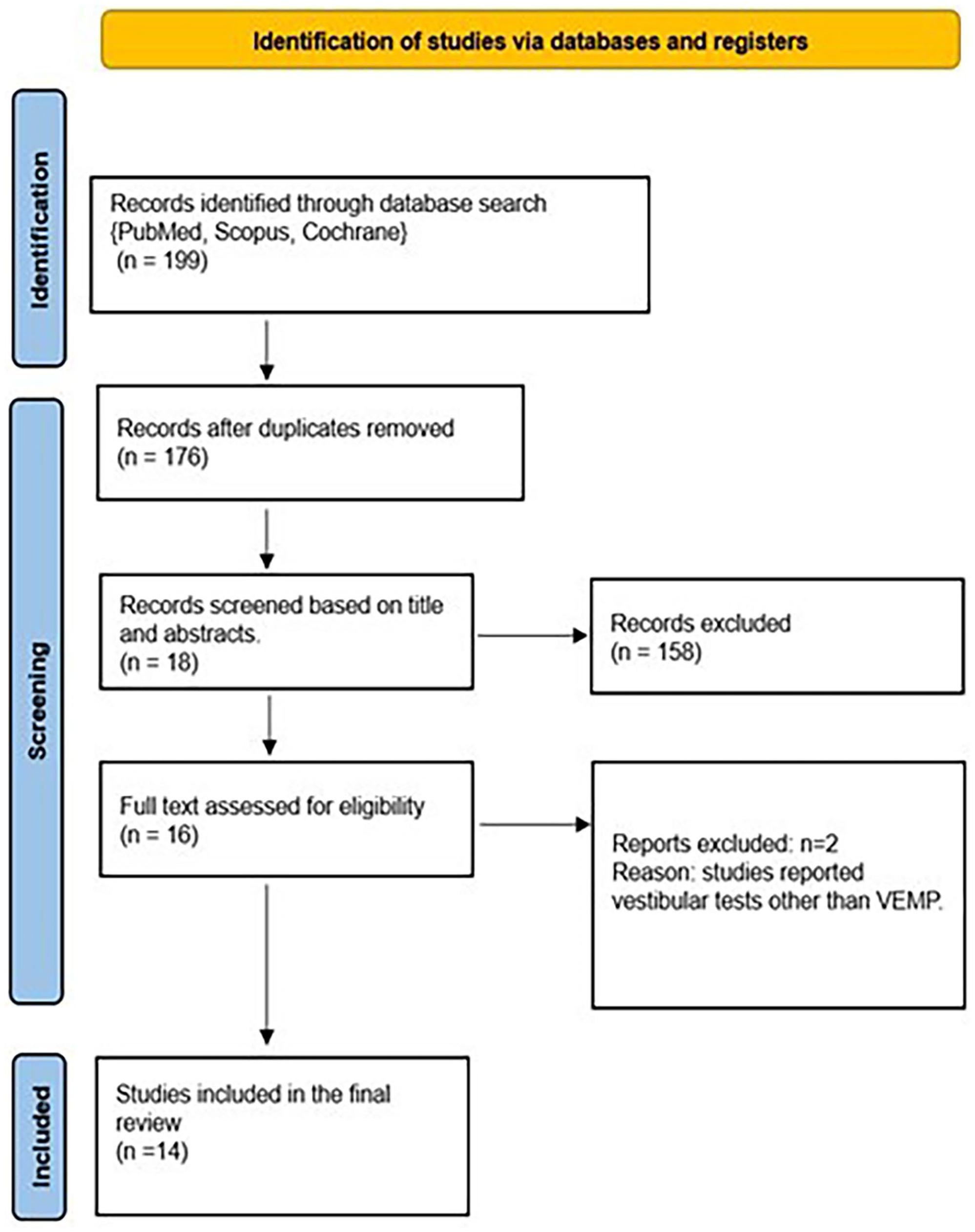
PRISMA flowchart of the process followed for the systematic review.
A total of 14 studied which explored the VEMP findings in patients with otosclerosis was included for the final stage. The details about type of VEMP and VEMP findings in case of otosclerosis was extracted from the included study which is presented in Table 1.
Characteristic of Included Study.
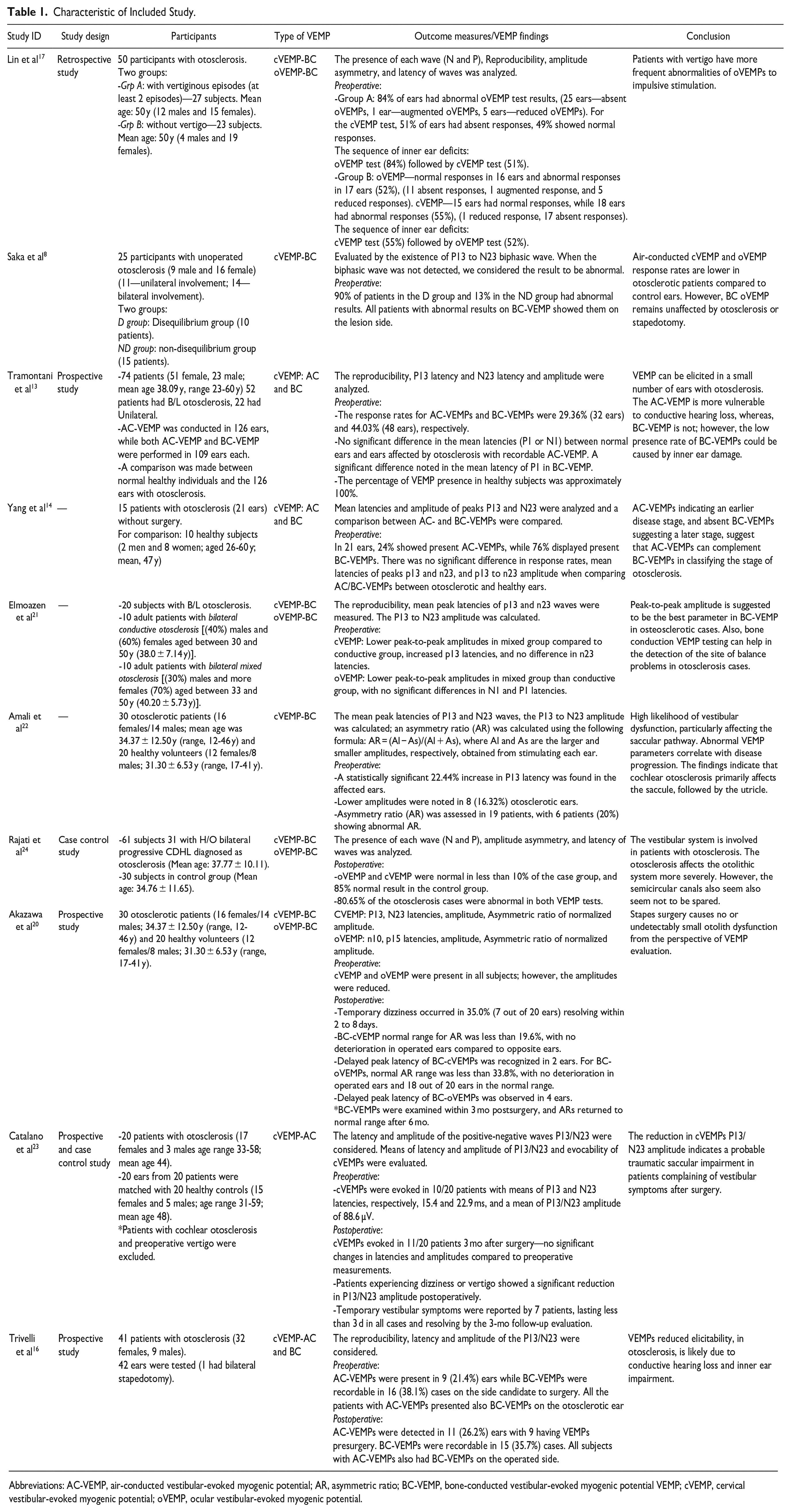
Abbreviations: AC-VEMP, air-conducted vestibular-evoked myogenic potential; AR, asymmetric ratio; BC-VEMP, bone-conducted vestibular-evoked myogenic potential VEMP; cVEMP, cervical vestibular-evoked myogenic potential; oVEMP, ocular vestibular-evoked myogenic potential.
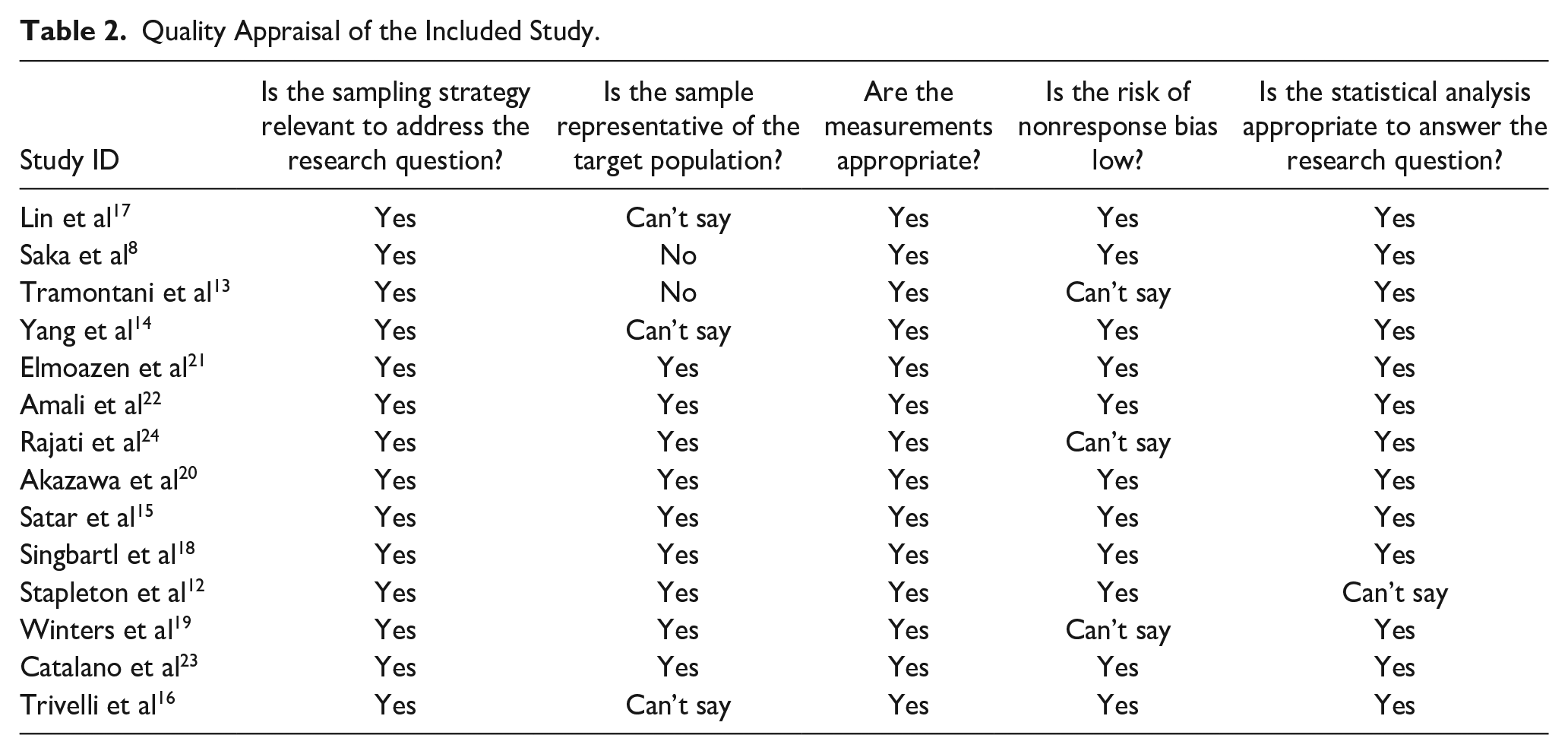
The methodological quality rating was done using MMAT as shown in Table 2.
Quality Appraisal of the Included Study.
Discussion
Although the most common method to evaluate the vestibular function using VEMP is via air conduction (AC) mode, many studies included in this review have found that employing the AC mode may be contraindicative in case of individuals with otosclerosis. As VEMP is known to be influenced by conductive pathologies, most of the authors used bone conduction (BC) VEMP to investigate the effects of otosclerosis on vestibular structures.
Air-Conducted Cervical and Ocular VEMP Findings
As otosclerosis is typically considered a conductive pathology, the expectation initially is for the air-conducted VEMP responses to be absent preoperatively, with the assumption of their restoration postsurgery. 12 However, variations in these responses were observed in these individuals.
Tramontani et al 13 discovered that air-conducted cVEMP response rates were lower than bone-conducted responses. They noted a significant difference in latency for bone-conducted responses but not for air-conducted ones. This led them to suggest that the presence of air-conducted cVEMP before surgery indicates a less affected inner ear compared to bone-conducted cVEMP. Preoperative recordable AC-VEMPs had significantly lower preoperative ABG, and lower means of AC and BC pure-tone averages (PTA) than those with absent AC-VEMPs. Yang elaborated on this idea, discussing how the AC cVEMP responses could offer insights into progression of the disease. The presence of AC cVEMP might suggest an earlier stage of the disease, while its absence, along with bone-conducted cVEMP, could imply a later stage. 14
While comparing the operated and unoperated ears, Satar et al found that the response rates were reduced in both air-conducted oVEMP and cVEMP, regardless of surgery. Interestingly, higher cVEMP response rates were noted postsurgery when compared to the preoperated data indicating positive surgical effects. Although lower response rates of cVEMP than the oVEMP suggests a potential saccular dysfunction. 15
The preoperative elicitation of AC-VEMPs is notably lower than that of BC-VEMP, possibly due to the presence of an ABG resulting from conductive hearing loss. The increase in the AC-VEMP elicitation postoperatively may primarily result from the closure of the ABG following the surgery. Absent AC-VEMPs postsurgery could imply inner ear damage. 16
Bone-Conducted Cervical and Ocular VEMP Findings
Utilizing a bone conduction stimulus result in a straightforward linear acceleration at the mastoids, whereas AC stimulation does not lead to this skull acceleration but instead moves the stapes, influencing the flow of endolymph. Consequently, BC stimulation holds an advantage over AC stimulation by bypassing the structures which would otherwise affect the VEMP response in cases of otosclerosis. 17
While investigating about the balance issues and bone-conducted VEMP findings, Singbartl et al 18 reported 3 patients complaining of dizziness out of 23 patients with otosclerosis, and all 3 patients exhibited normal BC-VEMP results. In contrast, Yang and Young 14 found 2 out of 5 patients complaining of vertigo (40%), showing absence of BC-VEMP response.
Saka’s study revealed a strong association between balance issues and abnormal BC-cVEMP findings where 90% of the individuals with balance problems showed abnormal BC-cVEMPs, suggesting a link to saccular dysfunction. 8
Tramontani’s investigation yielded intriguing preoperative patterns, indicating that mean ABG, AC, and BC PTA did not affect BC-VEMP elicitation. Furthermore, they observed prolonged latencies of P1 and N1 in BC-VEMPs in otosclerotic ears compared to normal ones, attributing this to the persistence of BC-VEMPs in advanced otosclerosis cases. Additionally, they proposed inner ear damage due to ototoxic substances from osteosclerotic lesions as a potential cause for the relatively low occurrence rate of BC-VEMPs presurgery. 13
Yang and Young, 12 that the mean air-bone-gap was higher in those individuals whose BC-VEMPs were absent, and when the BC PTA mean was greater than 30 dB, BC-VEMPs were found to be usually absent. Their study also studied the correlations between presence of BC-VEMP and types of patterns of conductive loss. While half of those with present BC-VEMP showed low tone type of a configuration, other half of them had an upward-sloping type of conductive hearing loss. As the disease progresses, the upward sloping type would gradually worsen and cause a flat conductive loss and about 80% of them showed absent BC-VEMP in these individuals. Thus, revealing that as the disease progresses, the response rates of BC-VEMP also decrease.
Concerning post stapes surgery outcomes, BC-VEMP response after stapes surgery was reported in 3 articles. Singbartl et al 18 and Trivelli et al 16 both observed the appearance of BC-VEMPs postoperatively, indicating a potential benefit of surgery on vestibular function. However, Winters et al’s 19 findings suggested minimal utricle damage from stapes surgery, whereas in a study by Akazawa reported no deterioration of VEMPs on the operated ear postoperatively in any cases. 20
When considering which parameters of the BC-VEMP could best help in understanding the effects of otosclerosis, are most informative in understanding the effects of otosclerosis, Elmoazen et al 21 and Amali et al 22 have both suggested that peak-to-peak amplitude is the most valuable metric. They argue that abnormalities in peak-to-peak amplitude are consistently observed in affected populations, indicating that this parameter can effectively capture alterations in BC-VEMP responses associated with otosclerosis.
Catalano’s study highlighted the clinical significance of BC-cVEMPs, showing a higher frequency of abnormal BC-cVEMPs in osteosclerotic patients with vestibular symptoms. Additionally, a significant reduction in P1/N1 amplitude postoperatively hinted at a possible saccular impairment in symptomatic patients after surgery. 23
Limitations and Future Directions
This review focuses solely on studies published in English, which may introduce language bias and overlooked relevant findings published in other languages. Additionally, the exclusion of literature from nonindexed resources and case reports may have resulted in the omission of valuable insights from alternative sources. Another limitation is the lack of available studies establishing a correlation between VEMP findings and presence of symptoms. However, a promising direction for future research is suggested by a study which identified a correlation between ABG findings and the presence of bone-conducted VEMP results. Remarkably, response rates were observed to decrease when the ABG exceeded 30 dB, indicating that ABG levels could potentially influence the presence or the absence of BC-VEMP responses. Future investigations could explore this relationship further to elucidate its clinical significance.
Conclusion
In comparing the effectiveness of AC and BC modes for eliciting VEMP responses in otosclerosis patients, it was observed that preoperatively, the AC mode often yielded poor response rates due to conductive pathology, whereas the BC-VEMP proved valuable in determining otosclerosis stages before surgery. However, postoperatively, interpretations differed: a presence of BC-VEMP suggested intact vestibular structures postsurgery, while its absence could indicate vestibular trauma, though other factors like stimulus intensity or efficacy of the fitted piston could influence the results. On the other hand, AC-VEMP responses postsurgery suggested resolution of conductive pathology or absence of lasting otosclerosis effects. Regarding VEMP type, while many studies indicate cVEMP as more affected, indicating saccular dysfunction, some findings suggest comparable response rates between cVEMP and oVEMP.
Footnotes
Availability of Supporting Data
Data are embedded in the manuscript as it’s secondary research.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval and Consent to Participate
This study is a systematic review based on already published data, where no human participants are involved; therefore, ethical approval not applicable.