
Abstract
CSF leak-related pneumocephalus is a rare complication of endoscopic transsphenoidal surgery (ETSS) and has been reported in previous studies. We are presenting a rare case of subdural pneumocephalus, unassociated with CSF leak, that developed in the sellar and suprasellar regions. This complication was diagnosed in an adult male 1 week after the removal of a large tumor in the same site via ETSS. The patient presented with a severe headache and visual deterioration. He was diagnosed by a CT scan and managed emergently via ETSS. The headache was relieved immediately after surgery, and the recent visual deterioration was reversed the next day. As far as we have reviewed in the context of complications of ETSS, no previous study has reported such a complication of pneumocephalus unassociated with CSF leak following ETSS. As a conclusion, pneumocephalus can occur with or without CSF leakage as a complication of ETSS, and it may be avoided by a good (water-tight) sealing of the surgical site.
Introduction
When indicated, endoscopic transsphenoidal surgery (ETSS) is an excellent choice for approaching sellar and suprasellar tumors. 1 Although it has been reported with a low rate of postoperative complications, ETSS may still cause serious complications such as carotid artery injury, CSF leakage, and meningitis. 2 Tension pneumocephalus is another possible and serious complication of ETSS. Pneumocephalus, also known as intracranial aerocele, can be a sequela of CSF leak according to Horowitz. CSF leak-related pneumocephalus has been reported as a complication of ETSS in several previous case reports. We aim to describe a rare case of postoperative aerocele, unassociated with CSF leak, in the sellar and suprasellar regions. To our knowledge, this is the first case presentation reporting such a complication of ETSS.
Case Presentation
A 44-year-old male was referred to the hospital one day after he had received a diagnosis of a compressive pituitary mass.
Patient’s complaints started 8 months before the presentation as a mild episodic headache, which then increased gradually in severity and duration. About 2 months before the presentation, he also developed a mild visual impairment in his right eye. As the patient reported, he was seen by an ophthalmologist who attributed the mild visual impairment to a right eye cataract and placed him under observation, without medical documentation or further investigations. Later on, the headache became worse, and the visual impairment rapidly progressed in both eyes. At that point, the patient finally consulted a neurologist who obtained an emergent MRI.
MRI scan (Figure 1) showed a sellar and suprasellar mass. This finding prompted the neurologist to refer the patient to the hospital.
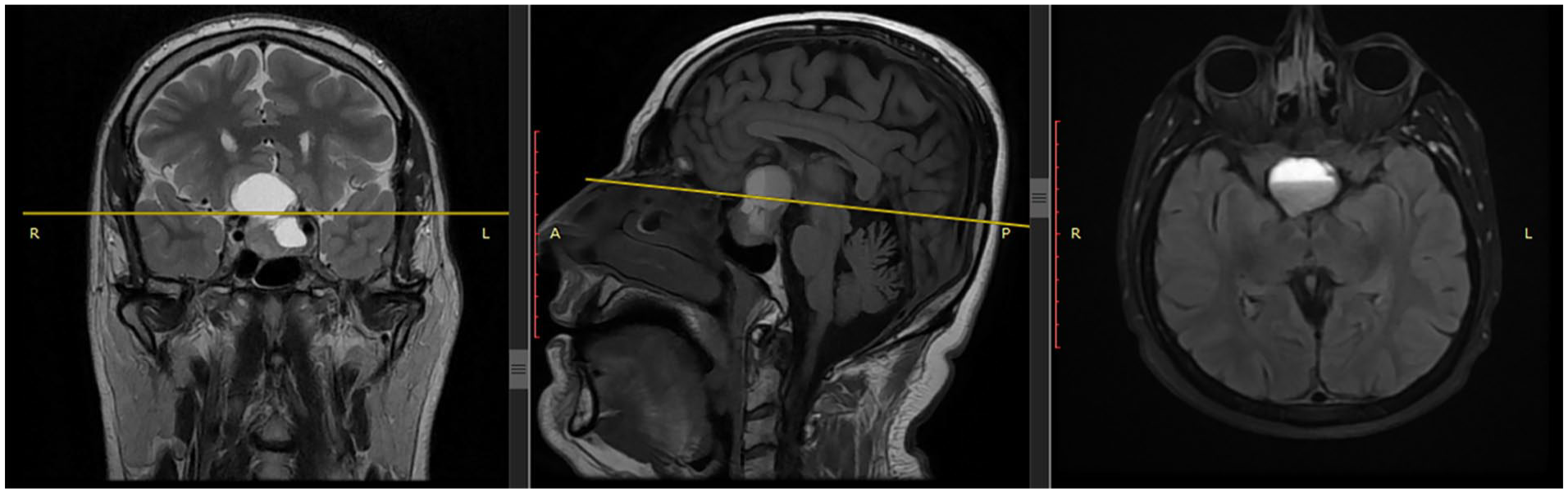
MRI images showing a mass in the sellar and supracellar regions.
In the hospital, the patient presented with a chronic headache unresponsive to medication, bitemporal hemianopsia, visual acuity of 0.4 in the left eye, and only light perception in the right eye. A fundoscopy revealed severe pallor of the right optic disc and moderate pallor of the left optic disc. Laboratory tests showed hyperprolactinemia (2466 ng/ml) with normal levels of TSH and cortisol.
A surgical decision was made promptly by a multidisciplinary team that consisted of a neurosurgeon, an otolaryngologist, and an endocrinologist. The patient underwent preoperative assessment and was clear of comorbidities, then, he was scheduled for an urgent surgery.
Next day, the patient underwent an endoscopic transsphenoidal excision of the mass. On the day 1 after surgery, the patient reported only mild intermittent headaches with improved vision in his left eye. As he reported, he was able to read again using his left eye. Three days later, the patient was discharged home without any noticed surgical complications.
One week later, the patient presented with a severe, progressive headache and total blindness (NLP) in his right eye. He noted that the headache started one day earlier after several bouts of sneezing. There were no symptoms or signs of CSF leak. A CT scan showed a large aerocele in the sellar and suprasellar regions, contained within the borders of the excised mass’s area, without any extension into the brain parenchyma (Figure 2).
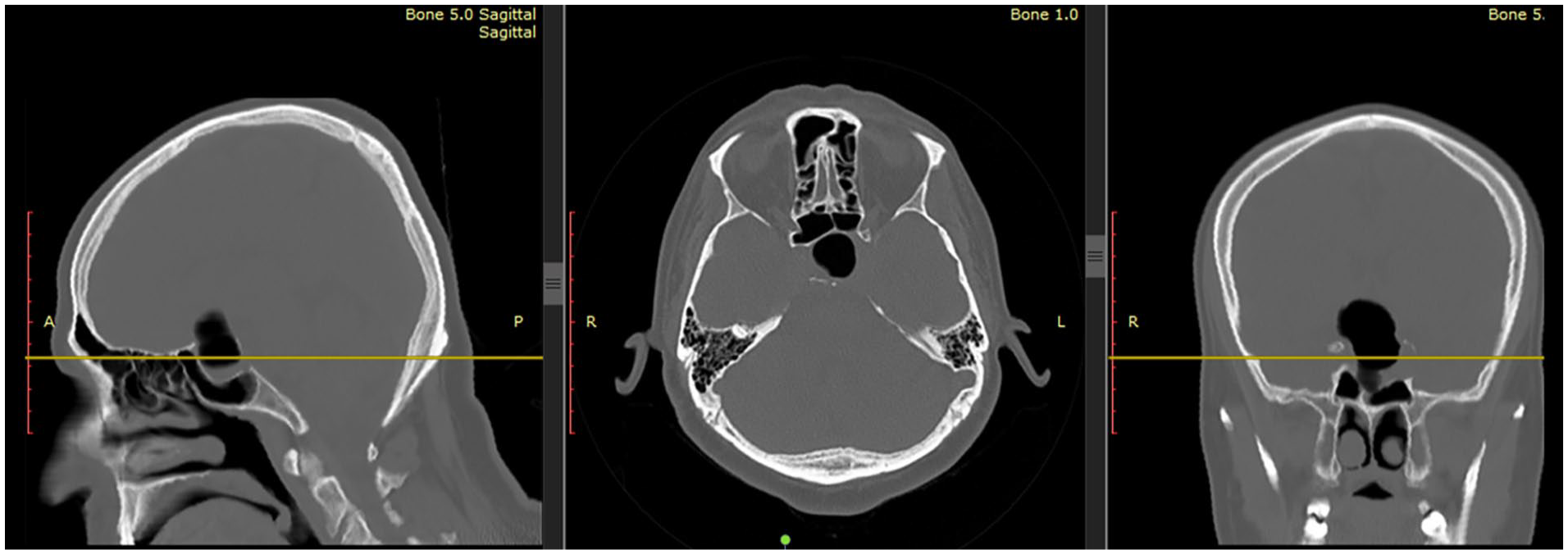
CT scan performed one weak after excising the mass shows an aerocele in the sellar and supracellar regions.
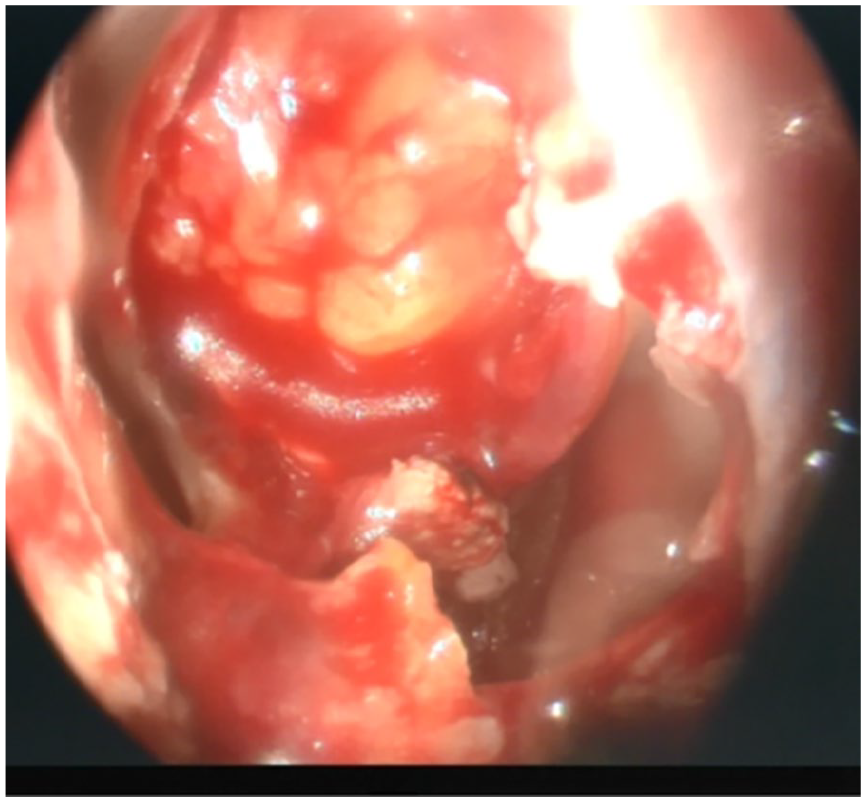
The patient underwent an emergent surgical exposure which revealed bilateral hanging-down of the subarachnoid space into the sella turcica, forming a one-way valve without any CSF leak (Figure 3). as we believed, that valve mechanism permitted air to enter the surgical site during sneezing bouts, without penetrating the subarachnoid space. The air had no way out due to the ptotic subarachnoid space which was blocking the entrance immediately after sneezing. the surgical exposure, along with the absence of CSF leak, has confirmed that the aerocele was subdural without any penetration into the subarachnoid space. Figure 4 shows the probable entrance site of air.
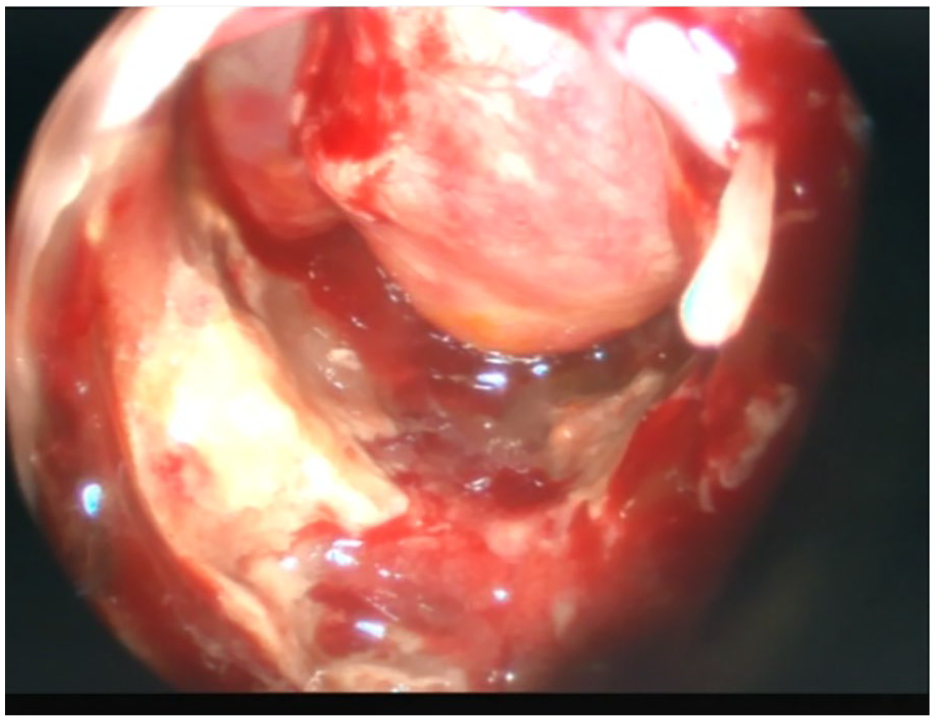
Intraoperative image showing a hanging-down subarachnoid space forming a one-way valve for air entrance in the middle.
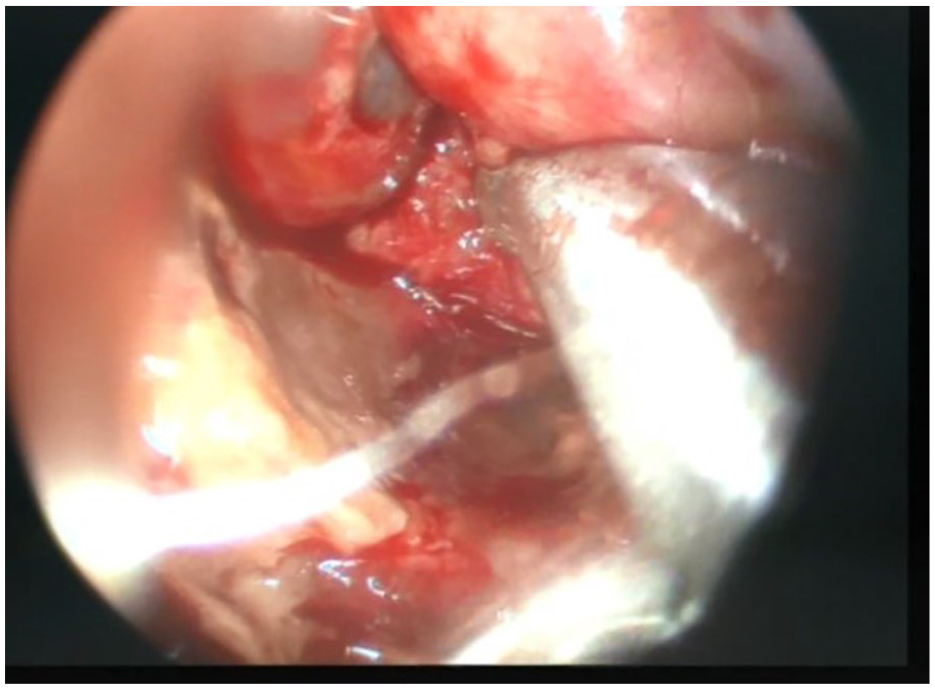
Intraoperative image while retracting the subarachnoid space, showing the air entrance site.
The case was managed by gently retracting the subarachnoid space and that caused the aerocele to be evacuated spontaneously without further manipulations. An intraoperative X-ray was performed and showed complete absence of air in the surgical site (Figure 5), compared with the preoperative image (Figure 6). Then, we reconstructed the floor of sella turcica with fat and fascia lata grafts using a multilayer closure technique (water-tight sealing) (Figure 7).
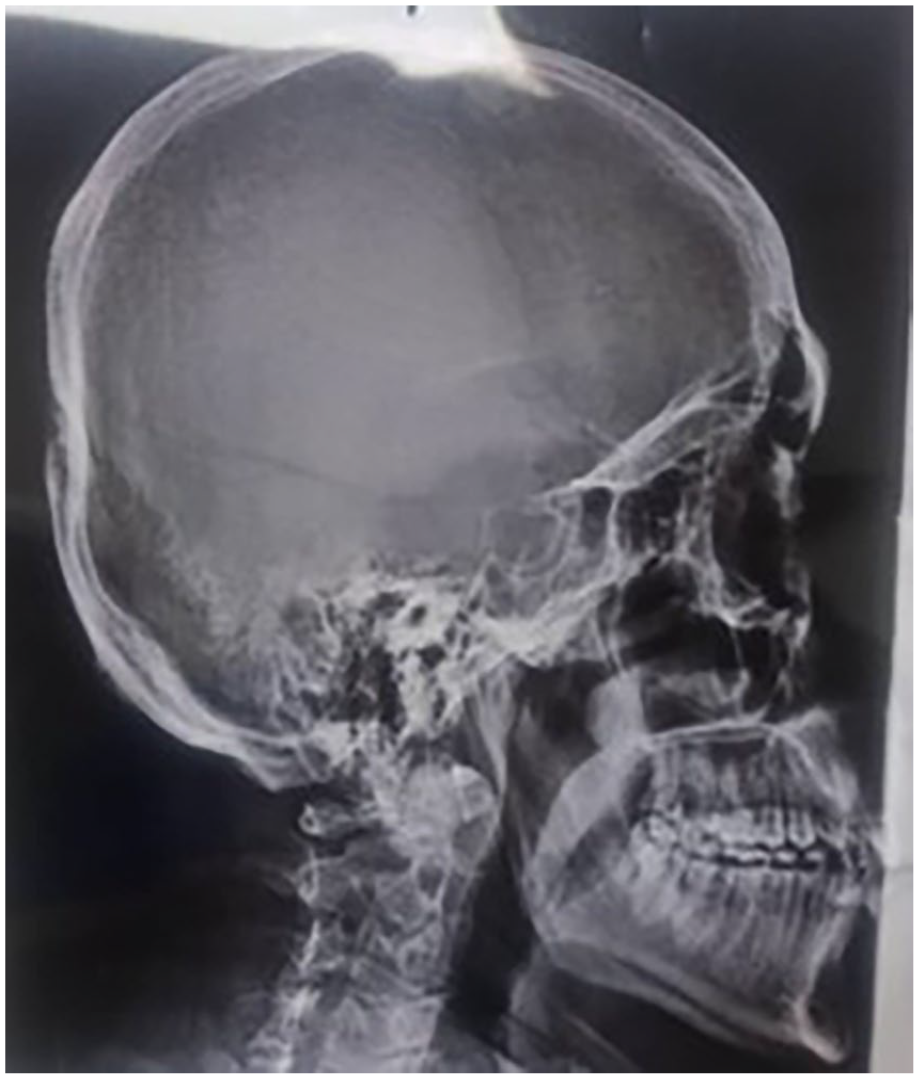
Intraoperative plain X-ray demonstrates the absence of air at the surgical site.

Preoperative CT sagittal scout image showing an aerocele in the sellar and supracellar regions.
Intraoperative image of the surgical site after performing a multilayer closure.
The patient’s headache has resolved immediately after surgery. On the day 1 after surgery, light perception in the right eye was restored. The patient was discharged home 3 days later. During the 2-month follow-up, the patient didn’t develop any new complaints. However, the visual impairment hasn’t shown any further improvement yet. The pathology result was consistent with pituitary adenoma. Recent laboratory tests have shown normal serum levels of free T4, prolactin, and glucose.
Discussion
Pneumocephalus, also known as intracranial aerocele or pneumatocele, is a well-known condition defined as a collection of air within the cranial cavity. 3 Anatomically, it can be epidural, subdural, subarachnoid, or intraparenchymal. 4 According to etiology, aerocele can be traumatic, infectious, neoplastic, iatrogenic, spontaneous, or congenital. Iatrogenic causes include transcranial surgeries, transsphenoidal surgeries, positive pressure ventilation, and other procedures. 4
There are several theories that may give explanations regarding the pathophysiology of pneumocephalus. The main two are Dandy’s theory of “ball valve,” 5 and Horowitz’s “inverted-soda-bottle effect.” 6 Dandy’s theory describes the unidirectional flow of air into the cranial cavity with no way out. Horowitz’s theory states that excessive CSF leak through a defect in the meninges leads to intracranial hypotension, which triggers air to influx through the same defect until a balance is achieved between intracranial and extracranial pressures. An enlarging pneumatocele can have a mass effect that may lead to intracranial hypertension and neurological deterioration. In this situation, it is called tension pneumatocele and is considered a life-threatening condition. 7
Clinical findings vary widely according to the site and size of pneumocephalus. In most cases, it is asymptomatic; however, it may cause symptoms ranging from mild headache to brain herniation and cardiorespiratory arrest in severe cases. 3 Head CT without contrast is still considered the gold standard for diagnosis.3,7 Given that most cases of pneumocephalus are asymptomatic and the air usually gets absorbed spontaneously, management can be conservative in asymptomatic patients. However, it requires emergent surgical decompression when clinical signs appear. 8 Our patient had a severe headache with further deterioration in his vision without any other symptoms. Intracranial hypertension and compression of the optic chiasm may explain his symptoms. The emergent surgical exposure and subsequent management prevented further complications, relieved the headache immediately after surgery, and helped restoring light perception in the right eye the next day.
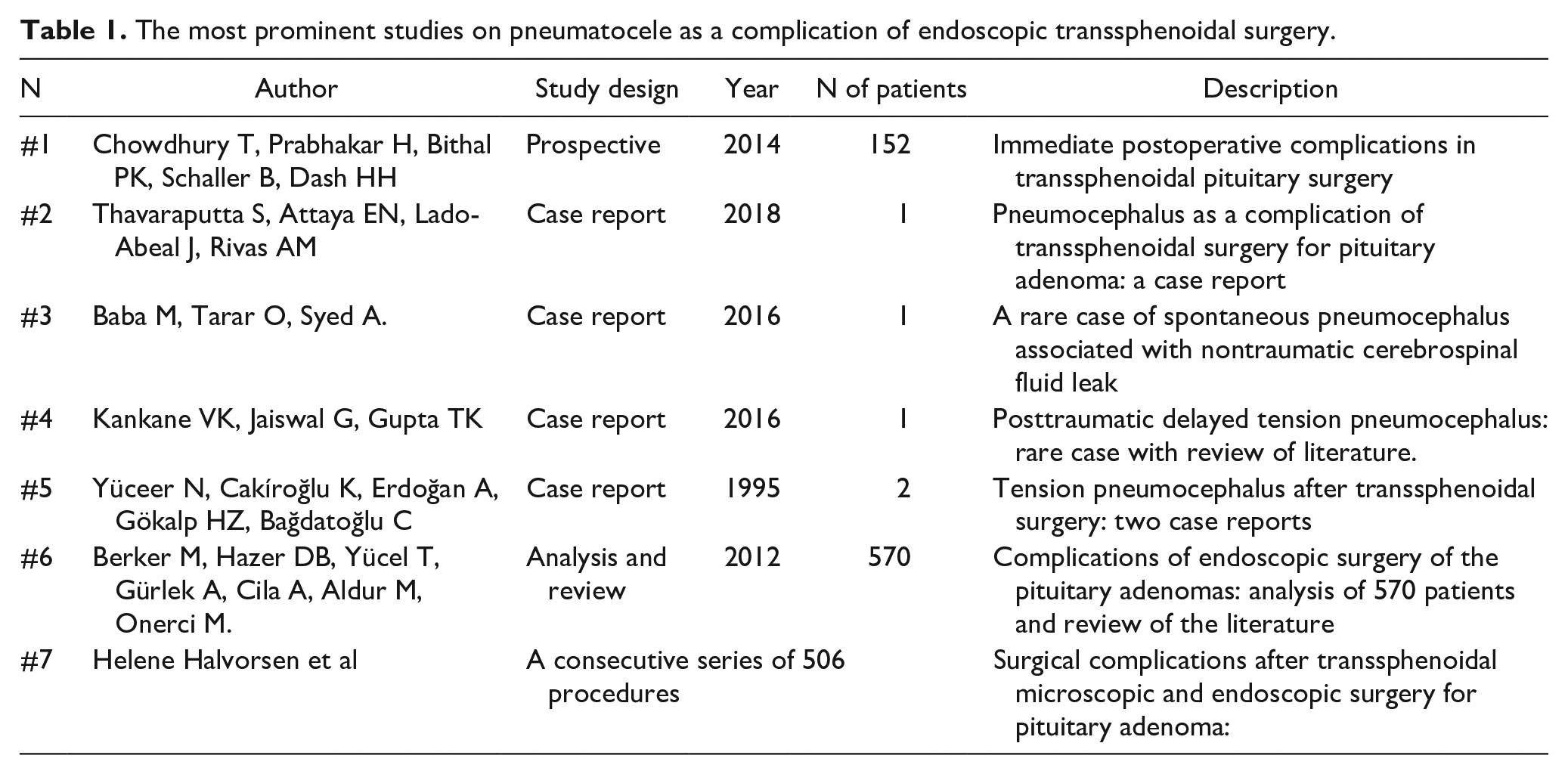
Our case represents a rare complication of ETSS. We have reviewed many studies concerning the complications of ETSS (examples of the most related studies are listed in Table 1). CSF leak was mentioned in several studies as a complication of ETSS. According to Horowitz, it may cause pneumocephalus due to evert-bottle effect. 6 Some studies have reported pneumocephalus as a sequela of CSF leak after ETSS (the second study listed in Table 1 is an example). However, our review showed that no previous study has described a similar case of subdural aerocele unassociated with CSF leak as a complication of ETSS. What is unique in our case is that there was no CSF leak. The complication was due to a mechanical process, which may be explained by Dandy’s theory, as described above.
The most prominent studies on pneumatocele as a complication of endoscopic transsphenoidal surgery.
The patient benefited from the successful management of the tumor, which improved his vision and relieved his headache, as well as from the subsequent rapid diagnosis and management of the aerocele.
On the other hand, there was a delay in diagnosing the tumor. as we believe, that delay occurred for two reasons. The first reason is the low health awareness of the patient and his family, which led him to seek appropriate medical consultation for his headache only after the disease had already progressed. The second reason is the poor previous ophthalmologic consultation, which was also undocumented.
Conclusion
Pneumocephalus can occur as a complication after ETSS in the absence of CSF leak and may be prevented by good sealing of the surgical site. Surgeons must consider this complication among other complications of ETSS.
Footnotes
Author Contributions
Abdulrahman Awad was the main surgeon in both surgeries and he supervised this manuscript; Amjad Al-Ali was an assistant surgeon in the second surgery. He wrote and revised this manuscript; Aghyad Ahmad diagnosed the primary tumor, and he was an assistant surgeon in the first surgery. He also revised this manuscript; Hussein Al-Abdullah was a surgeon’s assistant in the second surgery. He also revised this manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethic Approval
No ethical approval was required.
Informed Consent
A signed informed consent has been obtained from the patient to publish this case presentation.