
Abstract
Keywords
Introduction
The practice of hiring one’s own trainees is known as “self-hiring” and within some educational research has been referred to as “academic inbreeding.” In academia, this practice is said to be as old as the modern university. 1 In the university, the pros and cons have been debated with most pro arguments pointing toward hiring known entities who have been on extended interviews during training and most con arguments point toward lack of diversification of thought processes. In university settings, self-hiring is generally frowned upon with many institutions having either formal or informal policies prohibiting widespread self-hiring. Self-hiring has been well-described in university settings but has not yet been thoroughly explored in medical settings. In medical academia, self-hiring may be unique from that in university academia due to the multiple levels of post-graduate education that physicians undergo, including medical school, residency, and possible fellowship training. For continuity of patient care, there likely exists bias toward hiring those with a similar philosophical approach to the management of common disease entities. However, the concerns are similar to those expressed in non-clinical environments, as self-hiring in the medical setting likely carries a degree of confirmation bias and may also be a barrier to innovation.
Within the field of Otolaryngology—Head and Neck Surgery (O-HNS) a commonly expressed perspective is that self-hiring is rampant, although no studies have specifically addressed the topic for academic faculty hires. Residency match data has been used to show that medical students tend to match in a wide range of training programs. Studies showed that approximately half of candidates left their geographic region for training in the pre-COVID era, compared to a higher proportion of candidates matching at their home program in the post-COVID era (22% matched at home program pre-COVID and 30% post-COVID).2,3 Other hiring practices which have been studied within faculty and leadership positions include gender and racial disparities.4,5 These reports indicate that much work remains to be done to improve gender and racial diversity, with most ascribing to the “leaky pipeline paradigm” in which parity of hiring faculty members lags behind parity of undergraduate, graduate, and post-doctoral training. 5 In other words, until the potential pool of workforce candidates is appropriately diverse, it will be impossible for most O-HNS programs to have accurate representation based on gender and race. While much attention has been focused on gender and racial diversity, academic diversity (or the diversity of education/training background) and its role in self-hiring has not garnered such scrutiny. This is despite the wide availability of residency graduates with diverse academic backgrounds, with over 120 O-HNS training programs nationwide graduating residents yearly. The goal of this study is to investigate the prevalence of preferential hiring practices, particularly self-hiring, within O-HNS in the United States, focusing on top-ranked programs whose graduates represent the majority of those pursuing academic careers.
Methods
This study was exempt from review with the MUSC IRB as all data used was publicly available. For this study, O-HNS residency program rankings for the 2021 to 2022 academic year were obtained utilizing the Doximity Residency Navigator tool sorted by reputation. 6 These reputation rankings are based on a composite of voluntary surveys sent annually to current and graduated residents of O-HNS programs. Respondents can nominate up to 5 programs for these reputation rankings. According to Doximity, survey results over 3 years are pooled for their calculations. Doximity utilizes several weighting systems to account for self-nominations and program size. Self-nominations are accounted for via alumni versus non-alumni classifications, and program size is accounted for weighing inverse to the size of program alumni respondents. Nominations from more recent graduates are also weighted more heavily than less recent graduates. A list of the otolaryngology residency programs ranked 1st to 40th was obtained from these Doximity Residency Navigator reputation rankings for the 2021 to 2022 academic year available at the time of study initiation. From online O-HNS residency program directories and faculty profiles outlined in Supplemental Appendix 1, a list of all program faculty members along with their educational and training affiliations for medical school, residency, and fellowship (if any) were extracted. In order to create a network map of hiring connections between departments, interconnections of residency training programs to department of faculty appointments were evaluated quantitatively for departments #1-10. This was done by counting the number of individuals in each department list who trained at any program ranked #1-10, including those who completed residency training at the same department in which they were faculty. The network of faculty at these #1-10 departments completing residency at #1-10 programs was evaluated visually with a network analysis graph using Python 3. The number of faculty among all 40 departments who completed residency training at 1 of 4 groupings or tiers (programs #1-10, #11-20, #21-30, #31-40) were determined, with a fifth tier being all departments not included (#41+). These values were also stratified by in-group values (ie, faculty at programs #1-10 who completed a residency at a #1-10 program). Faculty leadership status, namely Departmental Chairs (DCs) and Program Directors (PDs) was also collected and used to stratify faculty.
Statistical Analysis
All graphs and figures were created with Microsoft Excel 365 (Microsoft, Redmond, WA, USA) and Python version 3.9.13 (Python Software Foundation, Wilmington, DE, USA). Comparison of proportions was performed with MedCalc 20.218 (MedCalc Software Ltd., Ostend, Belgium). For both text and tables, categorical variables (fellowship training, medical school, residency training) were presented as frequency (n) percentage (%). The total number of same-department affiliations for each individual at a given department was counted. “Prior Affiliation Ratio” was calculated by dividing the total prior affiliations in a given department by the total number of faculty in each department. “Prior Affiliation Average” was calculated by summing the total prior affiliations in a given department and dividing by the number of previously affiliated faculty.
Results
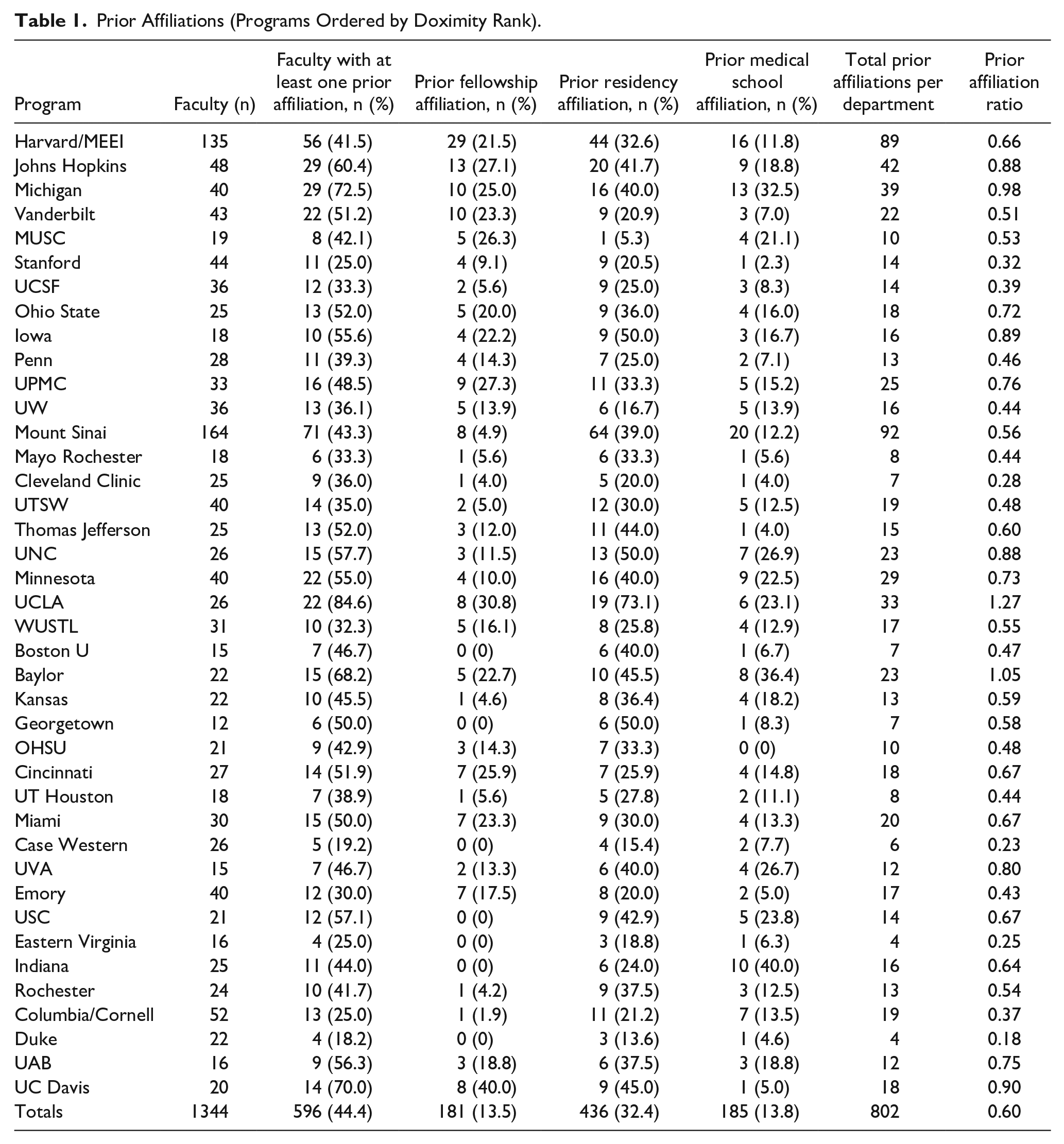
A total of 1344 clinical faculty were identified. Five hundred and ninety-six (596) individuals were identified as having at least one prior affiliation with their current department, or 44.4% of all included faculty. Overall, 181 (13.5%) individuals completed fellowship, 436 (32.4%) completed residency, and 185 (13.8%) completed medical school at their current department. Totals for each department are listed individually in Table 1. Figure 1A demonstrates the percentages of faculty with prior affiliations to their current department, and Figure 1B shows the percentages of faculty who completed various levels of medical training at their own institution/department: medical school, residency, and fellowship. Overall, there were 802 sum total prior affiliations among all clinical faculty members across all departments. The overall prior affiliation ratio for the 40 included departments was 0.60. The prior affiliation ratio for each individual department is included in Table 1. The 7 departments with the highest prior affiliation ratio, with values greater than 0.8, are shown in Table 2 part A along with the departments’ respective percentage of affiliated faculty and Prior Affiliation Average. Table 2 part B demonstrates the same information for the 7 departments with the lowest prior affiliation ratio, with values less than or equal to 0.4. The remaining departments ranged from 0.43 (Emory) to 0.8 (UVA).
Prior Affiliations (Programs Ordered by Doximity Rank).
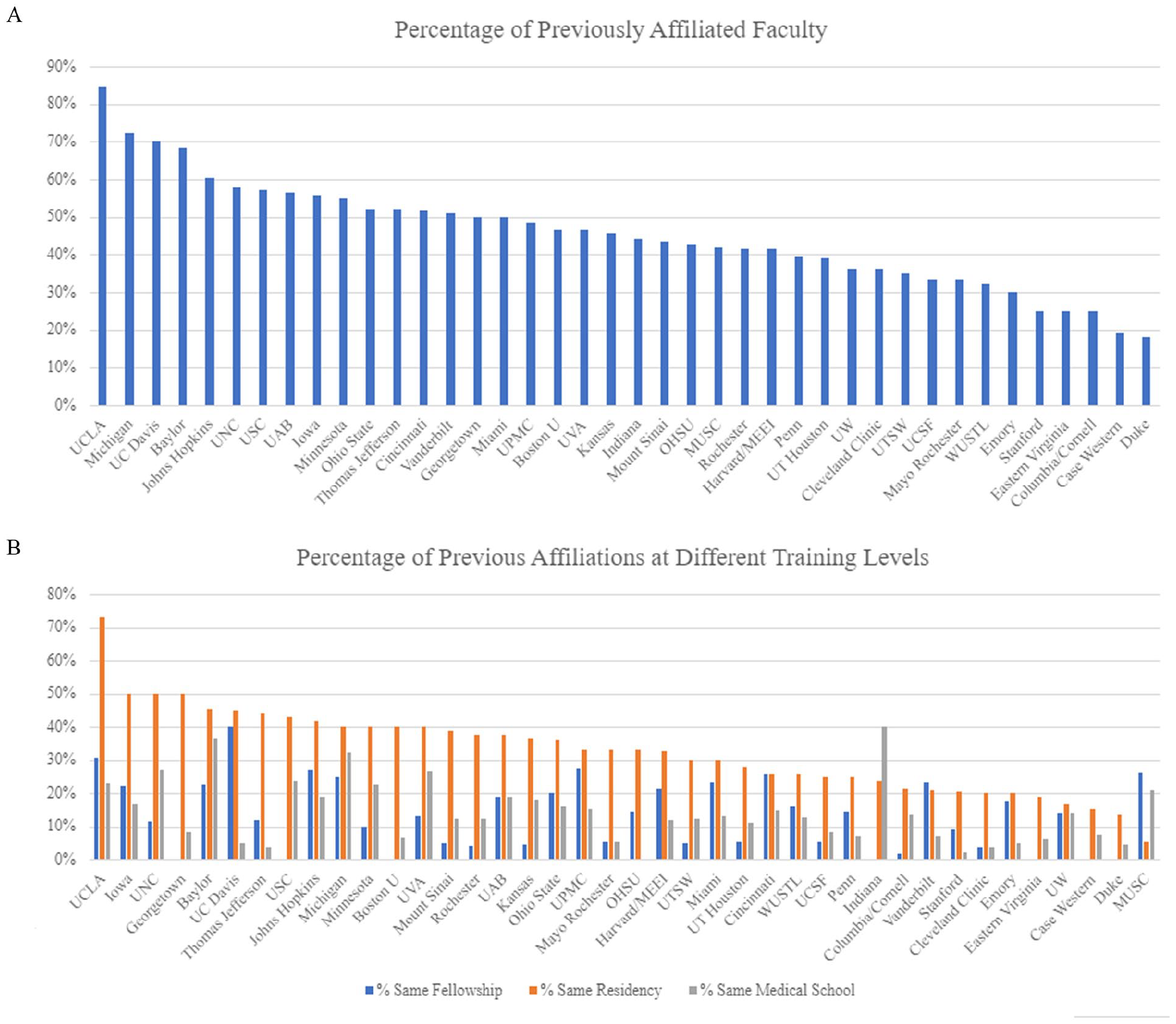
Percentage of Self-Hired Faculty by (A) Department and (B) Training Level.
Degree of Self-Hiring at Departments Correlated with High or Low Prior Affiliation Ratio.
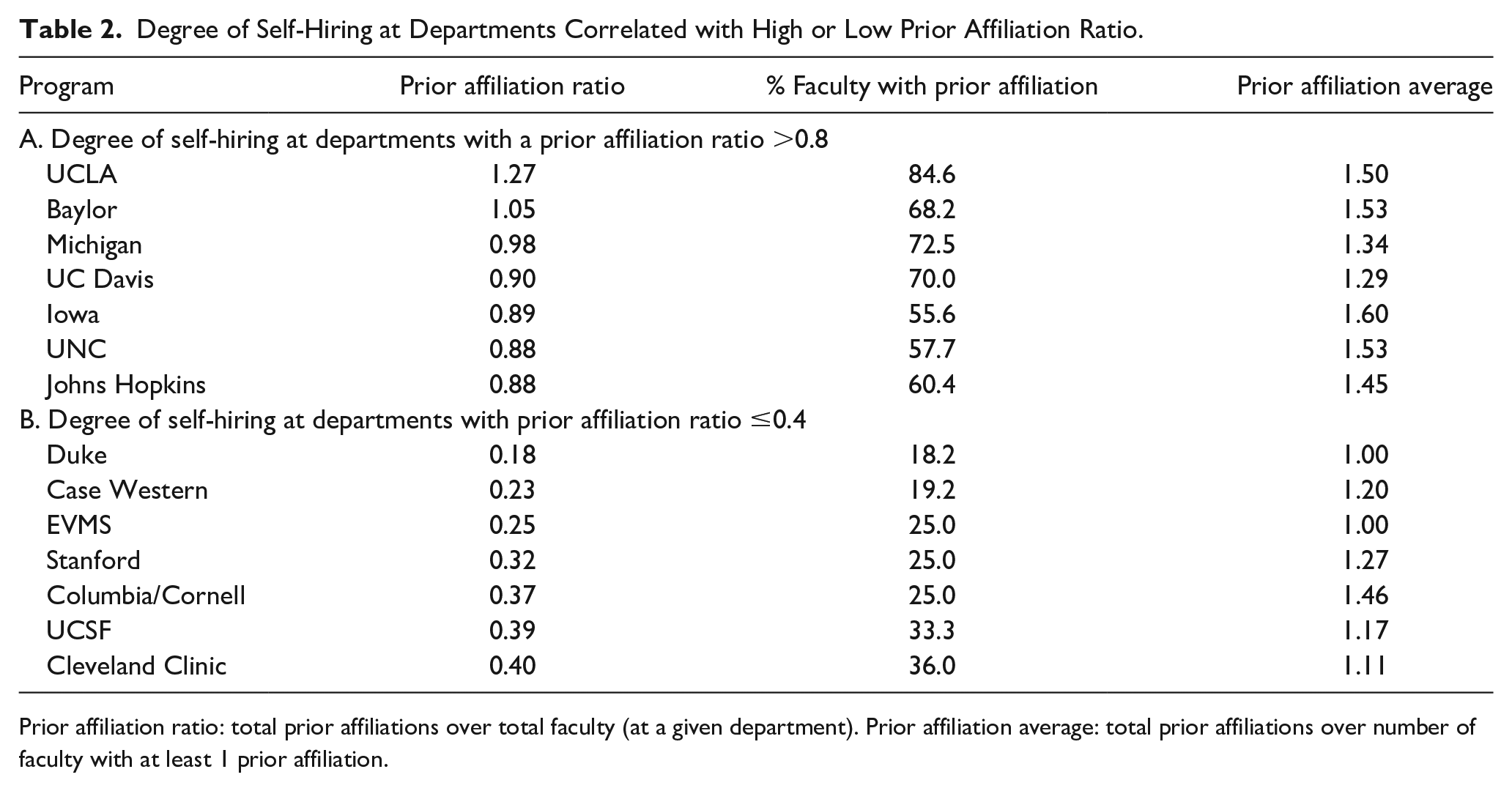
Prior affiliation ratio: total prior affiliations over total faculty (at a given department). Prior affiliation average: total prior affiliations over number of faculty with at least 1 prior affiliation.
In order to inspect the hiring patterns of highly ranked departments, we created a network map of departments ranked #1-10 (Figure 2). Each node (seen as blue circles) represents a department, with node size being proportional to department size in number of clinical faculty. There are both interdepartmental and intradepartmental arrows. Interdepartmental arrows demonstrate the hiring of residents from 1 department as clinical faculty in another. Intradepartmental arrows indicate residents being hired as faculty in their own departments. Arrow width or thickness is proportional to the number of individuals hired along each inter- or intradepartmental connection. This can be used to compare interdepartmental connections between different departments, as well as to compare the interdepartmental and intradepartmental arrows of a single department. The spreadsheet used to generate this network map, which includes the actual numbers along each interdepartmental and intradepartmental connection, is available in Supplemental Appendix 2.
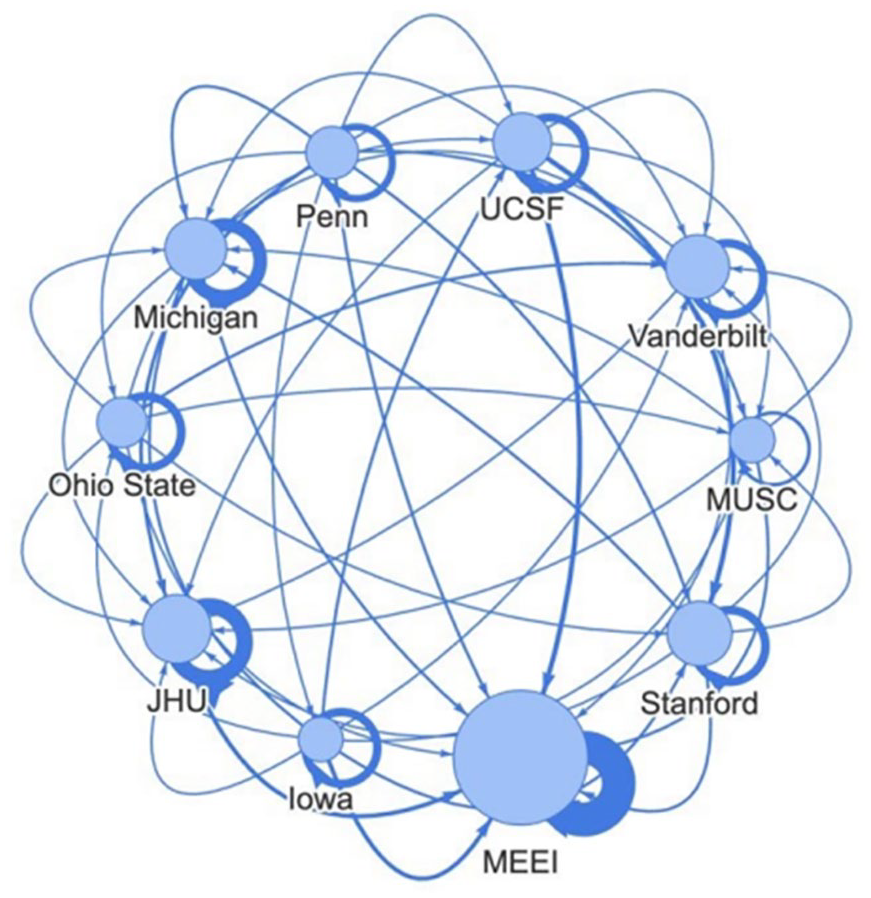
Network Map of O-HNS Departments #1-10. Arrows indicate the movement of residents from the department of their training to the departments hiring them as faculty.
We also examined the residency programs where all included faculty trained. Departments were separated into 4 tiers of 10 departments each: Departments #1-10, Departments #11-20, Departments #21-30, and Departments #31-40 with a fifth tier being unincluded departments (#41+). The percentages of faculty who completed each tier of residency program are shown in Table 3, including a fifth tier for faculty employed at a top 40 department who completed a residency program outside the top 40 (Departments #41+). 37.89% of faculty from Departments #1-5 completed a Tier 1 Residency, while 7.55% of faculty from the remaining Departments #6-40 completed a Tier 1 Residency.
Where Did Faculty and Department Leadership Complete Residency Training.
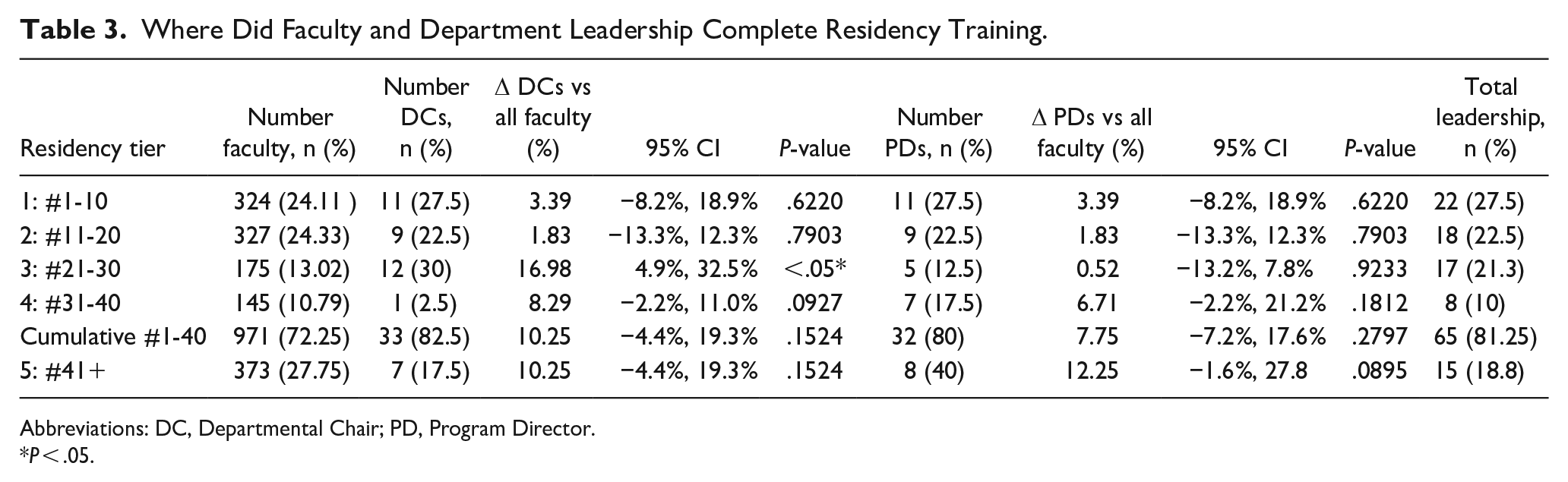
Abbreviations: DC, Departmental Chair; PD, Program Director.
P < .05.
Tables 2 through 5 examine rates of self-hiring specifically among departmental leadership. Table 3 demonstrates where overall faculty from all included departments completed their residency training by tiers, as well as specifically where departmental leadership (DCs and PDs) completed residency training. A comparison of proportions was performed between the rates of overall self-hired faculty for each tier versus the rates of leadership self-hiring for each tier. Overall, there was not a significant difference between the rates at which leadership versus faculty, in general, were self-hired for all tiers except for Tier 3 between overall faculty and self-hired DCs. Table 4 shows the quantity of any prior affiliations (medical school, residency, or fellowship) among both DCs and PDs for the department at which they currently work, with 40% of DCs and 62.5% of PDs having some prior affiliation. Table 5 demonstrates a comparison of proportions between tiers at which department leadership completed residency. There is significant difference between Tiers 1-4 and Tier 5 for both DCs and PDs (P < .0001). It was also found that the difference between Tiers 1-3 was significantly different from Tiers 4 and below for both DCs and PDs as well (P < .0001 and P = .0263, respectively). The differences between Tiers 1 to 2 and Tiers 3 to 5 did not show a significant difference for either DCs or PDs.
Department Leadership with Any Previous Affiliation to Their Current Department.
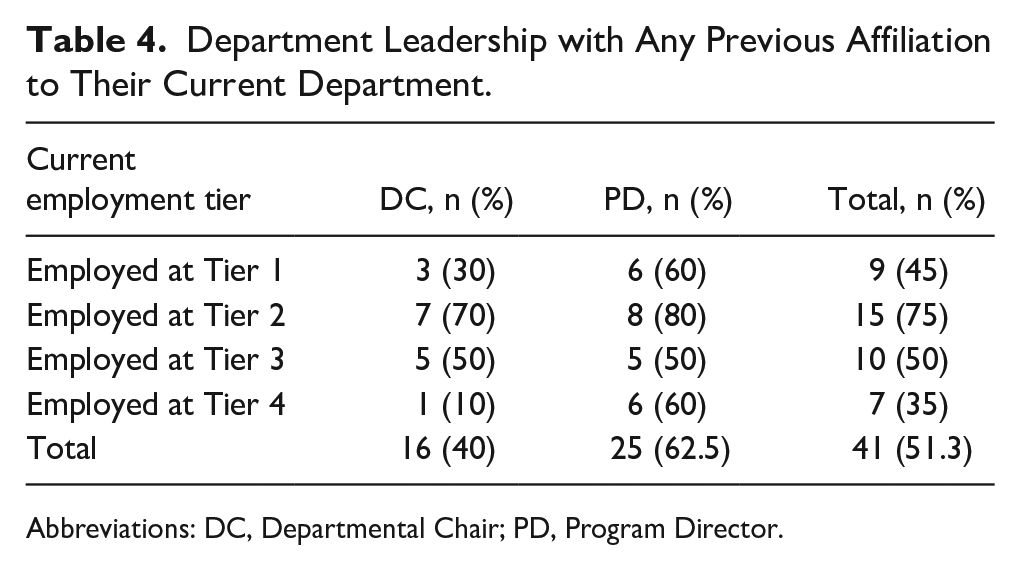
Abbreviations: DC, Departmental Chair; PD, Program Director.
Comparison of Proportions in Self-Hired Leadership from Higher Versus Lower-Ranked O-HNS Residencies.
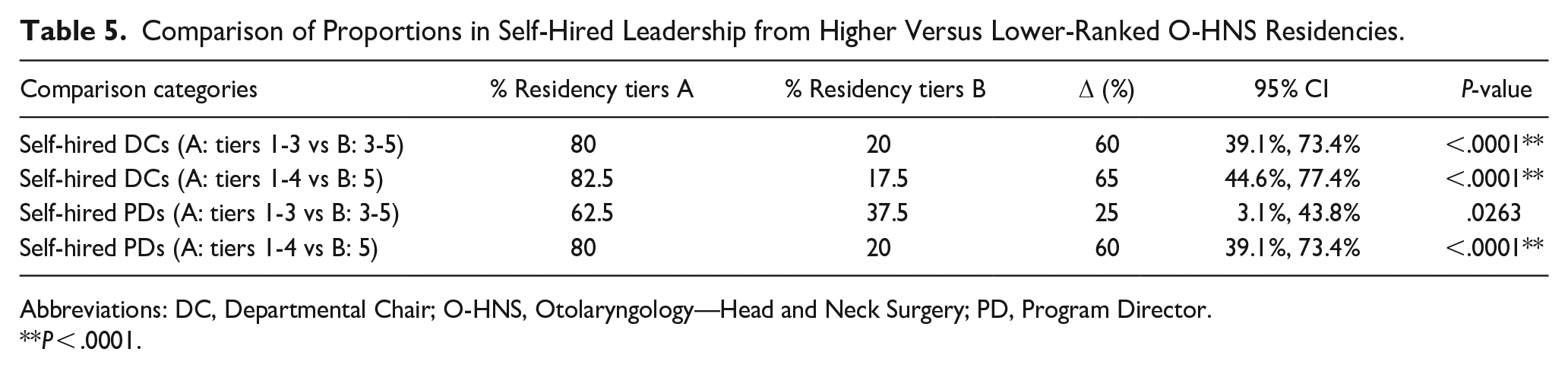
Abbreviations: DC, Departmental Chair; O-HNS, Otolaryngology—Head and Neck Surgery; PD, Program Director.
P < .0001.
Figure 3 examines the residency tiers from which departments make their faculty hires, with Figure 3A including intradepartmental hires (self-hiring) and Figure 3B excluding them to control for self-hiring. The same 4 tiers of O-HNS departments previously used were color coded by rank: #1-10 are blue, #11-20 are orange, #21-30 are gray, and #31-40 are yellow. The 4 corresponding tiers of residency programs where faculty previously completed O-HNS training are indicated in 4 spots along the x-axis. The percentages of faculty currently working in a given department tier who completed training at an indicated residency tier are totaled as shown in Figure 3. Figure 3A shows that each department tier has a peak in its corresponding residency tier, implying that departments hire faculty who completed residencies at similarly ranked departments. However, this is primarily attributable to self-hiring practices, as the rates of hiring from each residency tier normalize once intradepartmental hires are excluded (Figure 3B).
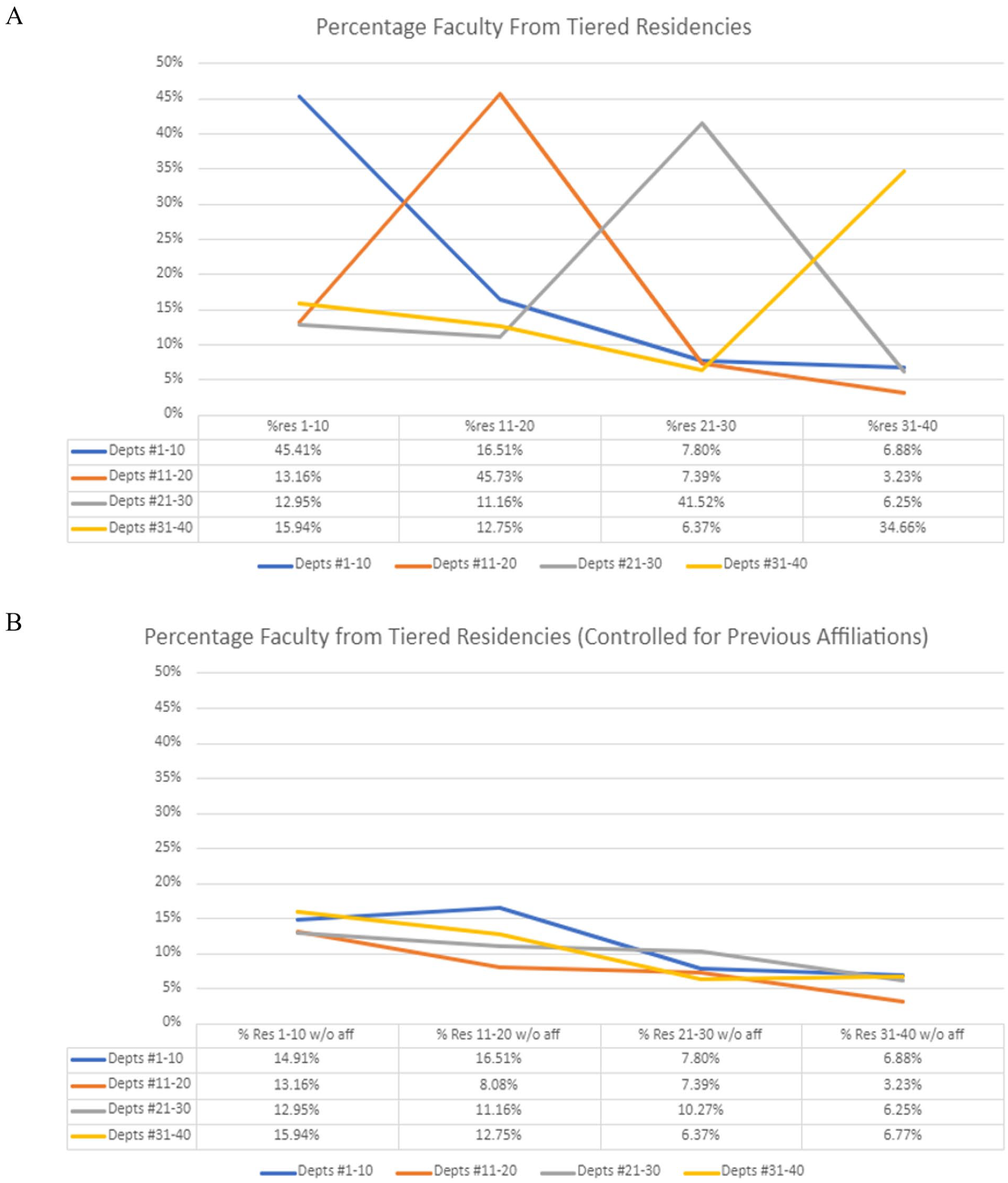
Percentage of faculty by (A) residency tier and (B) residency tier controlled for prior affiliations.
Discussion
It is apparent that preferential hiring practices, especially self-hiring, are present in the top 40 ranked O-HNS departments on Doximity as they heavily gravitate toward hiring their own trainees. From departments included in our study, nearly half of all faculty, about 44%, have at least 1 prior affiliation with their own department (see Table 1 and Figure 1). This also becomes evident upon inspection of the Network Map (Figure 2) in which the increased thickness of nearly every intradepartmental hiring arrow indicates that the top 10 ranked departments hire a significant portion of their faculty from their own pool of trainee graduates. No interdepartmental connections seem to be of particular significance (eg, Department A tends to consistently send graduates to Department B) and none are as strong as intradepartmental hiring patterns. Further proof for this phenomenon is found in comparing Figure 3A to Figure 3B. In Figure 3A, peaks in each residency tier indicate that departments hire faculty from resident graduates of departments within their own tier. However, once self-hires (resident graduates hired on at their own department) are removed as shown in Figure 3B, the peaks disappear. Thus, what seems to be a favoritism toward hiring residents from similarly ranked departments is simply the result of self-hiring.
The training paradigm of medicine is unique in that there are 3 possible training sites that can be considered for prior affiliation: medical school, residency, and fellowship(s). Thus, a novel metric to measure self-hiring in the unique context of medical education and training is warranted. Prior Affiliation Ratio, defined as total number of affiliations within a department divided by number of faculty within the department, allows one to determine the degree to which various departments practice self-hiring. Another way to understand this ratio as it relates to the extent of self-hiring is by jointly examining 2 pieces of information: the percentage of self-hired faculty and the average of affiliations of all the self-hired faculty members (“Prior Affiliation Average”). This gives an idea of how many faculty at a given department are self-hires as well as the average amount of training a self-hired faculty member has done at their department. Multiplying these 2 terms will similarly give the prior affiliation ratio. These metrics can all be compared for the departments with the highest and lowest Prior Affiliation Ratios shown in Tables 2 parts A and B.
When assessing prior affiliation ratio, a given individual can range from zero prior affiliations with their department, to a maximum of 3 (meaning they attended medical school, residency, and/or fellowship at the same department where they are now faculty). While any given department will have a mix of faculty with multiple affiliations or without any prior affiliations, a large numeric value of prior affiliation ratio is illuminating. A prior affiliation ratio of 1 indicates that, on average, every single faculty in that department has at least one prior affiliation with their department. Seven of the included departments had a prior affiliation ratio greater than 0.8, 2 of which surpassed 1.00. The University of California Los Angeles had the highest prior affiliation ratio at 1.27 meaning, on average, each faculty completed one prior UCLA training affiliation, and a quarter of faculty also had a second UCLA training affiliation. In contrast, Duke had the lowest prior affiliation ratio at 0.18, meaning less than a fifth of their faculty had any prior training affiliations. A similar trend has also been shown among the leadership of Canadian academic O-HNS departments, as they noted a statistically significant association between location of residency training and department of employment. 7
It has been established that the hiring practices of prestigious departments outside medicine follow an intensely hierarchal pattern. 8 A later study by the same group showed that as much as 80% of university faculty across the country come from a small, consistent group of prestigious universities and that this pattern held true across multiple different fields. 9 They also showed that only 5-23% of these faculty were able to find a position at a university or institution more prestigious than the one where they received their doctoral degree. Our data shows that this is also true within academic O-HNS departments. While 38% of faculty from O-HNS Departments #1-5 completed a residency ranked #1-5, only 7.5% of the remaining faculty from Departments #6-40 completed a residency ranked #1-5. This does not consider the remaining programs ranked below #40 on Doximity, where the figure is likely to be even lower.
It is important to consider the impact that self-hiring may have on the training and productivity of O-HNS departments. It has potential to provide both risks and benefits, and even more unclear is whether it is the risks or benefits that dominate in O-HNS. Several authors and studies have examined both the real and perceived risks and benefits of this phenomenon in university settings, and many of their discoveries may translate to academic O-HNS departments. One study found that university professors who are self-hired view it as a primarily positive experience, despite a majority of professors viewing it as a detrimental practice overall. 1 Many simply see self-hiring, good or bad, as an inevitable part of any academic career, and it has been shown to have a presence in institutions across the world. 10 Some of the perceived benefits of self-hiring include conservation of time, money, and energy for both the institution and faculty in the hiring process. Proponents also claim that self-hiring is important to maintain the established culture of a given department as well as its reputation or prestige, 1 and may even be a key process in the development of newer departments and their desired cultures. 11
This may be especially true in departmental leadership hires, as they have a more significant and direct influence on department direction and culture. Our data shows that high rates of departmental leadership among highly ranked O-HNS departments, both Chairs and Program Directors, are self-hired (Table 4) and that higher-ranked departments tend to hire leadership from their own or similarly ranked departments (Table 5). Leadership don’t seem to be hired at significantly different rates compared to overall faculty (Table 3). While our data is unable to determine why this is occurring, most conjecture would center around the reputation of the department. In general, highly ranked departments included in this study have been well established for a significant amount of time and thus may be intending to maintain or augment culture rather than establish it as previously mentioned. DCs and PDs who were trained within the culture and reputation of highly ranked departments may feel a responsibility to continue to self-hire or hire from programs of similar rank to uphold well-established reputations. This may also be a result of increased familiarity with their own or similarly ranked departments.
Although proponents highlight certain potential benefits, a generalized perception is that self-hiring poses more harm than good.1,11 Perceived risks of the phenomenon labeled in some literature as “academic inbreeding” include diminished scientific productivity, extra-departmental information exchange, and efficacy in teaching and learning. Multiple studies have established that scientific research productivity and extra-departmental information exchange at universities are both decreased in what is labeled “inbred,” or self-hired, faculty compared to their “non-inbred,” or non-self-hired, counterparts12,13 resulting in fewer peer-reviewed publications. They even found that the productivity of “non-inbred” faculty suffers when hired at institutions with heavy levels of self-hiring. 13 While one of these studies did find that “inbred” faculty actually spend more time and energy in teaching pursuits than “non-inbred” faculty, 13 the question remains as to the efficacy and usefulness of what is being taught. 11 Just as research creativity and innovation may be curbed by “academic inbreeding” and lack of faculty mobility, so too can teaching strategies become stagnant and outdated. As Horta describes, 11 well-established teaching structures supported by “academic inbreeding tend to maintain often obsolete learning styles, pedagogical practices, and knowledge.”
As academic O-HNS departments are also teaching institutions, this risk is present in O-HNS residency training as well. If departments continue to hire their own trainees, the same thought processes, ideas, and techniques are perpetuated. Residents who later become faculty in their own department may teach future residents the same things they were taught, and one may question whether this can stagnate innovation and limit new approaches to O-HNS surgery and patient care. While this might not be inherently negative, it may limit the technical and mental tools available to residents upon graduation.
Since self-hiring does maintain some benefits in spite of these risks, and may even be crucial to the development of young academic departments, Horta et al. proposed a potential best practice 13 : that a department maintain a small cohort of self-hired faculty to grow and preserve departmental culture and outreach, while the remainder of the department is supplemented with non-self-hired faculty who can engender innovation, improve scientific productivity, and inject new ideas into established teaching models. Future research in this area could examine the extent to which self-hiring impacts scientific productivity and residency training efficacy in O-HNS.
Limitations
One of the limitations of this study is that it does not include all academic O-HNS departments in the United States. By restricting our search to the first 40 departments on Doximity, we limit the comparisons we are able to make that could be potentially even more significant between lower-ranked departments and the higher-ranked included departments. We anticipate expanding our research to more extensively incorporate departments #41+ that were not included in the present study. Another limitation is that the 2021 Doximity rankings were used as those were the most current rankings available at the time of extraction; however, they no longer reflect the current rankings. We anticipate that this does not strongly affect our results as most departments remain at a similar rank over subsequent years. Another limitation is the bias inherent in rankings. While no ranking system is perfect, we felt that Doximity most closely aligns with our aims in this study as it focuses more on prestige and training reputation than other rankings such as US. World News Report or Blue Ridge rankings. An additional limitation of our study was that we did not factor in other demographics such as gender, race, or leadership position in the present study, which remains a potential area for future research. Our network map (Figure 3) is limited in that it does not account for residents who leave their department for fellowship and then return as faculty afterwards, which potentially mitigates the stagnation of ideas and techniques. Similarly, our study does not consider previous academic positions; faculty may have worked in other departments initially before eventually taking a position with the department where they completed their residency. Data regarding previous academic positions was seldom available and, if present, only included the most recent academic position and not a full work history.
Conclusion
Highly ranked O-HNS departments rely heavily on self-hiring of trainees in making faculty and leadership hiring decisions. It is unclear whether this phenomenon poses more benefit or risk to O-HNS departments, but efforts should be made to insure against the established negative effects seen in other fields. This can be done by promoting awareness of preferential hiring practices, particularly self-hiring, and making conscious investments in changing long-held opinions which tend to be non-evidence based while establishing transparent and meritocratic hiring practices for departmental leadership in addition to all faculty.
Supplemental Material
sj-docx-1-ear-10.1177_01455613241275320 – Supplemental material for Assessing Academic Preferential Hiring Practices in Highly Ranked Otolaryngology Departments
Supplemental material, sj-docx-1-ear-10.1177_01455613241275320 for Assessing Academic Preferential Hiring Practices in Highly Ranked Otolaryngology Departments by Brendon K. Warner, Christopher C. Munhall, Sunny Shah, Chada Pitiranggon, Terence James M. Camilon, Shaun A. Nguyen and Robert F. Labadie in Ear, Nose & Throat Journal
Supplemental Material
sj-xlsx-2-ear-10.1177_01455613241275320 – Supplemental material for Assessing Academic Preferential Hiring Practices in Highly Ranked Otolaryngology Departments
Supplemental material, sj-xlsx-2-ear-10.1177_01455613241275320 for Assessing Academic Preferential Hiring Practices in Highly Ranked Otolaryngology Departments by Brendon K. Warner, Christopher C. Munhall, Sunny Shah, Chada Pitiranggon, Terence James M. Camilon, Shaun A. Nguyen and Robert F. Labadie in Ear, Nose & Throat Journal
Footnotes
Authors’ Note
Presented at AAO-HNSF 2022 Annual Meeting in Philadelphia, PA on September 14, 2022.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Dr Robert F. Labadie is a consultant for Spiral Therapeutics and receives NIH funding for other projects.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.