
Abstract

The coming decade will demonstrate the greatest expansion of human spaceflight since the Apollo era. NASA’s Artemis Program and the massive expansion of the private aerospace industry indicate a need to fully comprehend health challenges faced by astronauts. However, while current missions involve healthy, professional astronauts, future missions will likely include tourists and private crew members who may have preexisting conditions that predispose them to otolaryngologic complications. Thus, there remains a need to explore the relationship between the field of otolaryngologic health and space travel. This perspective article will explore the potential rhinological and sinus health risks these individuals might face during spaceflight.
A study in 2015 aimed to examine crew-member medication use aboard the International Space Station (ISS) and Space Shuttles. 1 Prolonged symptoms were defined as lasting for more than 7 days and congestion/allergy emerged as the primary reasons for astronauts to utilize medications. The grouped category of decongestants and antihistamines was found to have a total single use rate of 2.432 per all crew members aboard the ISS and 0.80 per all crew members aboard the shuttles. 1 This represents the average number of times these medications were used across all crew members for the duration of the mission. This discrepancy in usage could possibly be attributed to the duration of the mission as ISS missions are of longer duration in comparison to the shuttle program.
Understanding the physiologic and environmental factors is crucial for understanding the changes to otolaryngologic health during spaceflight (Figure 1). The most accepted mechanism for sinonasal symptoms in microgravity is physiologic fluid shifts. This manifests as cranial redistribution of a large volume of fluid, originating from the lower extremities, upon transitioning from a higher to lower gravity environment. This redistribution occurs rapidly into the head and neck tissue compartments, manifesting as sinus congestion and facial swelling. 2
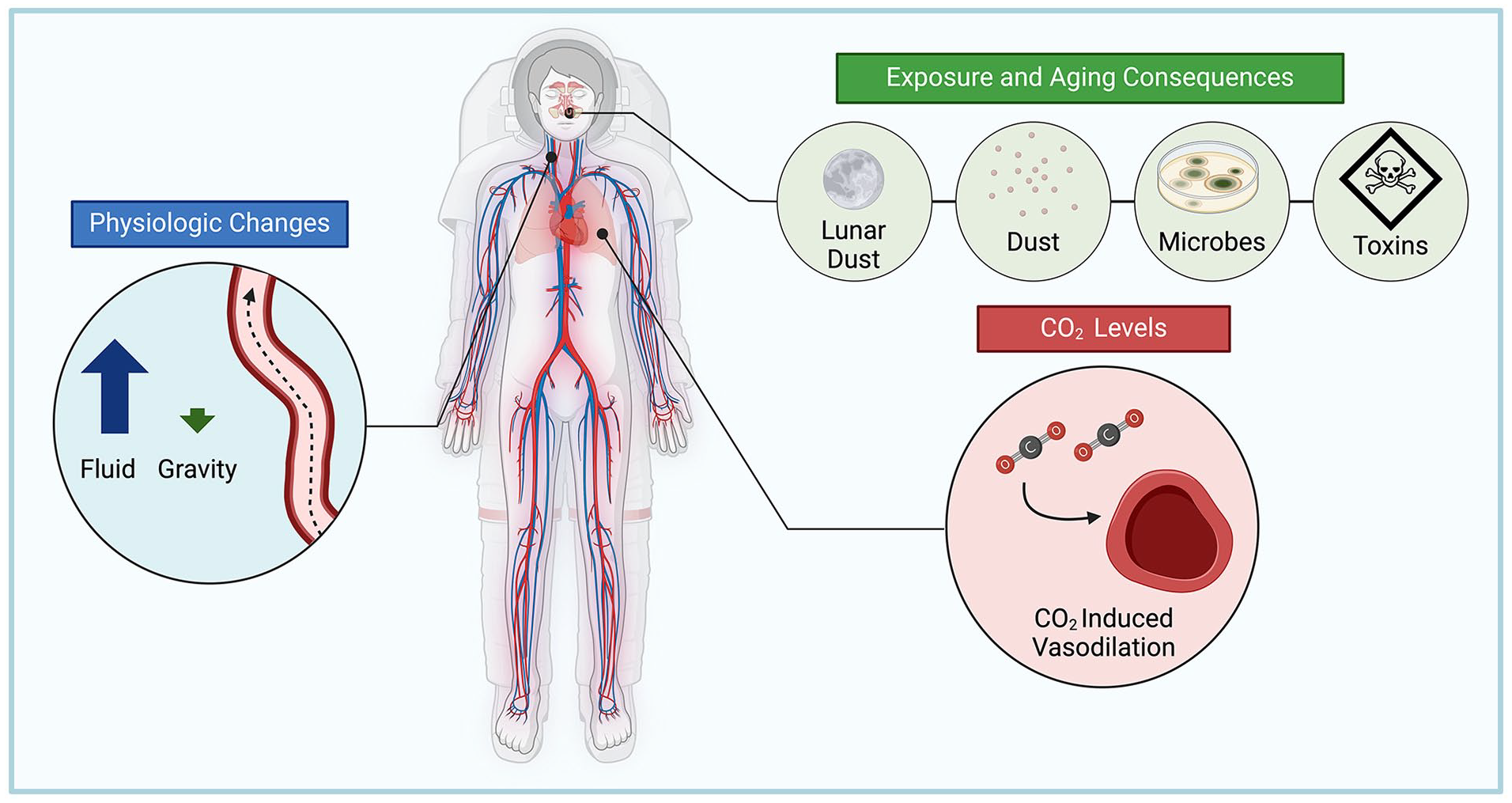
Current known and possible causes of sinonasal congestion for astronauts (created with Biorender.com).
Other potential causes of spaceflight-associated sinonasal congestion are elevated CO2 levels and aging of the ISS.3-5 Station age has been cited as a factor due to increased dust particles, microorganisms, and toxic contaminants. Dust particles were postulated to increase sinonasal symptoms after Expeditions 30 and 31 (December 2011 to July 2012), where astronauts reported greater allergic sensitivity to the cabin compared to previous trips. Upon analyzing samples from the ISS, Perry and Coston found significant debris from clothing lint, hair, nail clippings, food, plastic, and paper, particles large enough to be trapped in the upper airways and trigger inflammation. 4 Astronauts typically undergo a thorough medical evaluation and history assessment for allergies that may interfere with regular duties. Though specific tests for allergies were not identified in public documents, it is indeed possible that an individual’s specific sensitivity and immune function could play a critical role in their response to the unique environment onboard the ISS. We hypothesize that this may have an even greater impact in the years to come when one considers the expansion of spaceflight to private individuals who may present with a broader range of health conditions and comorbidities. Microorganisms have also been implicated as a previous study reported an odds ratio of greater than 2.5 (P = .0172) for in-flight medical events to occur when overall microbe counts were above the acceptable limit. High surface counts of fungi and bacteria correlated the most with these medical events as opposed to air counts. 5 This suggests an interesting link between hand-to-surface contact that astronauts utilize to translate in the microgravity environment. Toxic materials onboard the station, from the off gassing of materials, fluid lines, and waste management systems, have also been identified as another aging consequence.
Return to the lunar surface poses its own unique challenges. Reexamination of the Apollo-era health complications has highlighted the role of lunar dust in causing nasal symptoms as 33% of all medical complaints were related to this category. 6 One theory posits that the fine particulate nature of lunar dust produces mechanically abrasive sharp edges that may cause type IV hypersensitivity. 6 A recent in vitro study has, however, indicated a lack of response to lunar dust, suggesting that the allergenicity risk may be low. 7 Regardless, the role of lunar dust should be explored further since it will be tracked inside modules post extravehicular activity. The potential for a response to Martian dust must be considered in the years to come.
Another factor implicated in microgravity-based sinus congestion is elevated CO2 levels. The lowering of extracellular pH by CO2 leads to increase in signaling pathways involving nitric oxide, cyclic nucleotides, and prostanoids contributing to increased head and neck vasodilation and vascular headaches. Anecdotal reports aboard the ISS indicate a lower threshold of CO2 for the onset of headaches when compared to levels on earth. 8
As space exploration expands, comprehending advanced otolaryngologic health challenges becomes increasingly imperative. We suggest exploration and insight into the nature of additional otolaryngologic complications to better prepare for the expansion of spaceflight to the general population.
Footnotes
Data Availability Statement
Data sharing not applicable to this article as no datasets were generated or analyzed during the current study.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Omar G. Ahmed is a consultant for Aerin Medical and Medtronic ENT. Masayoshi Takashima is a consultant for Neurent Medical and Medtronic ENT. The authors have no other funding, financial relationships, or conflicts of interest to disclose.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Statement
Our institution does not require ethical approval for such review articles/editorials.
Patient Consent
Not applicable.
Trial Registration Number/Date
Not applicable.