
Abstract
Multiple endocrine neoplasia type 2B (MEN2B) syndrome is a rare genetic disorder primarily driven by mutations in the RET proto-oncogene. MEN2B exhibits diverse symptoms affecting multiple organ systems, with mucosal neuromas being a prominent feature. These benign tumors contribute to the syndrome’s clinical variability, alongside medullary thyroid carcinoma and pheochromocytoma. The article presents a case study of a young girl diagnosed with MEN2B, complicated by laryngeal neuromas leading to respiratory distress post-thyroidectomy. Laryngeal neuromas are exceedingly rare, underscoring the importance of recognizing such manifestations for proper airway management, especially during surgical interventions. Despite its rarity, MEN2B presents significant clinical challenges, requiring early detection, genetic counseling, and multidisciplinary management for improved outcomes. Clinicians must remain vigilant for rare manifestations like laryngeal neuromas to prevent serious complications, particularly during surgical procedures.
Introduction
Multiple endocrine neoplasia type 2B (MEN2B) syndrome is a rare genetic disorder primarily caused by germline mutations in the RET proto-oncogene, which plays a critical role in the regulation of cell growth and proliferation. 1 MEN2B is mainly caused by 2 genetic mutations of the RET gene, M918T mutation in exon 16 in 95% of cases, and A883F in less than 5% of patients. 2 Prevalence studies suggest that MEN2B syndrome is rare, with an estimated incidence of approximately 0.2 in 100 000 individuals worldwide. 3 However, due to its rarity and variability in clinical presentation, accurate prevalence rates may vary across different populations.
Symptoms of MEN2B syndrome are diverse and can affect multiple organ systems. One of the hallmark features of MEN2B syndrome is the presence of mucosal neuromas, which are benign tumors arising from nerve tissue. These neuromas commonly affect the mucous membranes of the lips, tongue, and inner lining of the eyelids. The onset of mucosal neuromas in MEN2B syndrome typically occurs in early childhood or infancy, usually during the first decade of life, although they may become more prominent with age. 4 These neuromas tend to proliferate and can be observed in various locations within the oral cavity and ocular region. In addition, mucosal neuromas may also develop in other areas such as the gastrointestinal tract, conjunctiva, and nasal passages, contributing to the diverse clinical presentation of the syndrome. 5
Aside from mucosal neuromas, individuals with MEN2B syndrome may also develop other characteristic features, including medullary thyroid carcinoma (MTC) and pheochromocytoma. The age at presentation varies depending on the type (M918T vs A883F) and time of mutation (de novo vs germline). 6 Early diagnosis and appropriate management of MEN2B syndrome are crucial to mitigate the risk of complications associated with endocrine tumors and to improve patient outcomes. Genetic testing plays a pivotal role in the identification of RET gene mutations, enabling early intervention and surveillance for associated malignancies.
We present the case of a young girl diagnosed with MEN2B, found to have laryngeal neuromas complicating extubation after thyroidectomy.
Case Report
This is the case of a 5-year-old girl that presented to the outpatient clinic for right neck mass of 8 months duration. Perinatal history was relevant for neonatal sepsis and constipation at birth. No relevant familial history of syndromes. Physical examination was suggestive of enlarged lymph nodes that are nontender, hard, and fixed with no skin changes. A computed tomography (CT) scan and magnetic resonance imaging (MRI) were ordered and showed a large anterior mediastinal mass causing tracheal deviation with a conglomerate of enlarged cervical, paratracheal, and subcarinal lymph nodes (Figure 1). A CT-guided biopsy of an enlarged lymph node showed MTC, with TTF1, PAX-8, calcitonin, and chromogranin positive. Laboratory workup showed an elevated calcitonin level (40 K) and normal urine catecholamine levels. Genetic testing was positive for the pathogenic variant in RET (p.Met918Thr), confirming the MEN2B diagnosis.
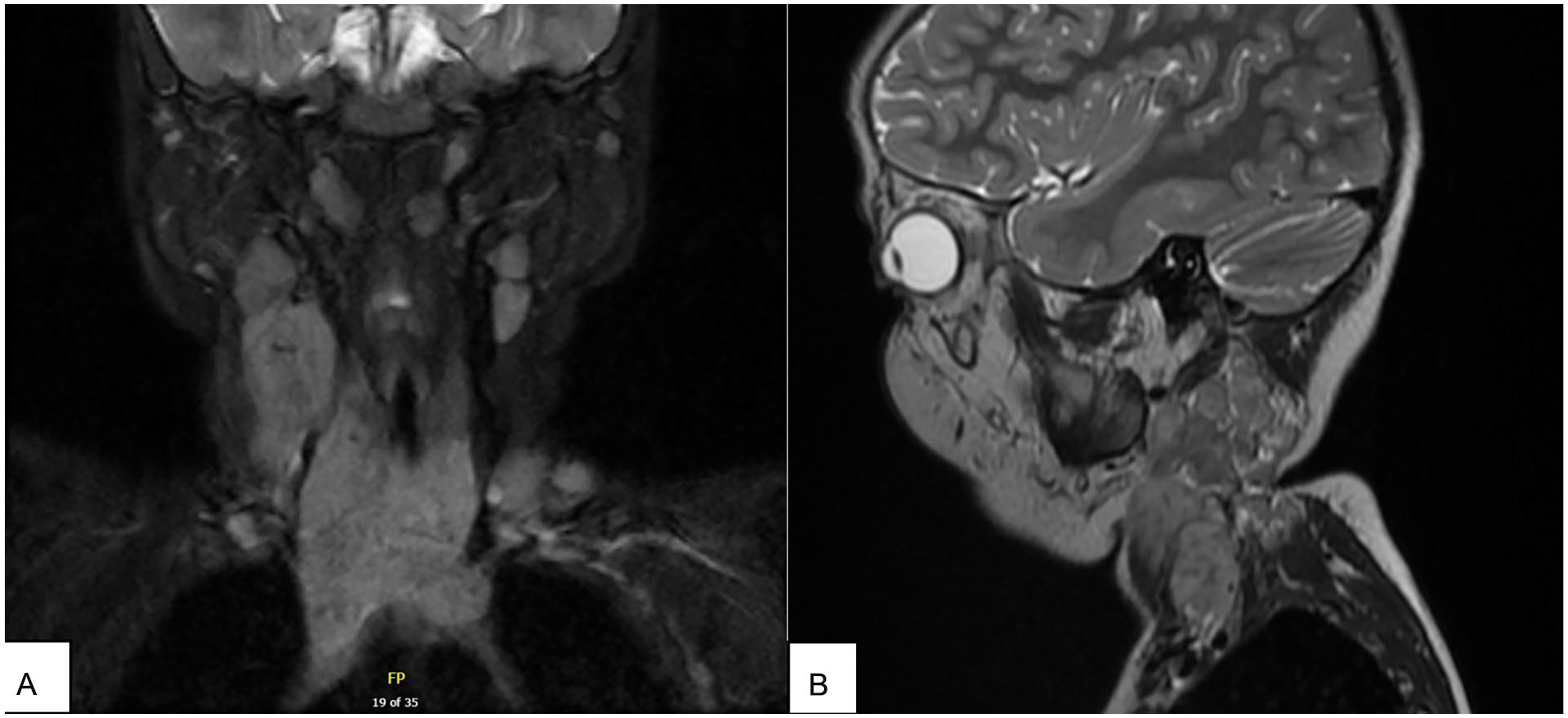
Coronal (A) and sagittal (B) MRI images showing the large mediastinal mass with enlarged cervical lymph nodes. MRI, magnetic resonance imaging.
The patient was taken to the operating room for tumor debulking and modified right neck dissection. The right sternocleidomastoid and jugular veins were sacrificed and dissection carried to the prevertebral space. After the surgery, the patient was extubated; however, she had severe stridor with respiratory distress and required re-intubation.
She was scheduled for diagnostic bronchoscopy during which mucosal lesions were found at the vocal folds bilaterally (Figure 2). The lesions were removed and biopsies confirmed mucosal neuromas, positive for S-100 (Figure 3).
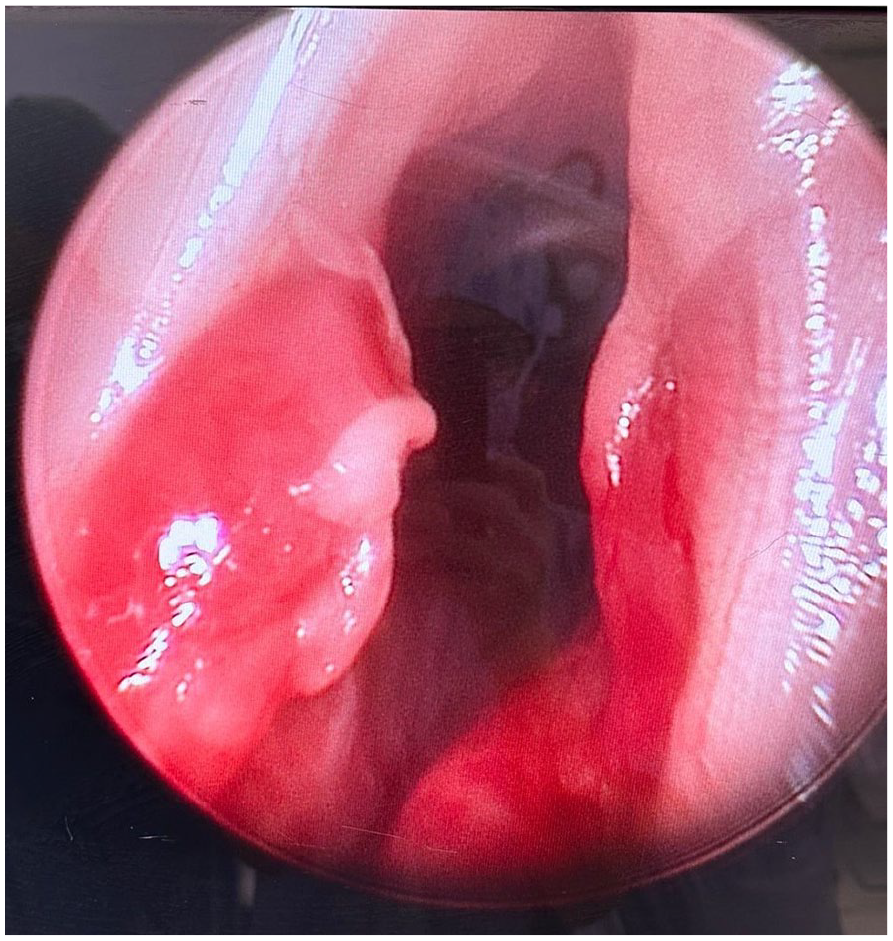
Laryngeal neuromas found during bronchoscopy.
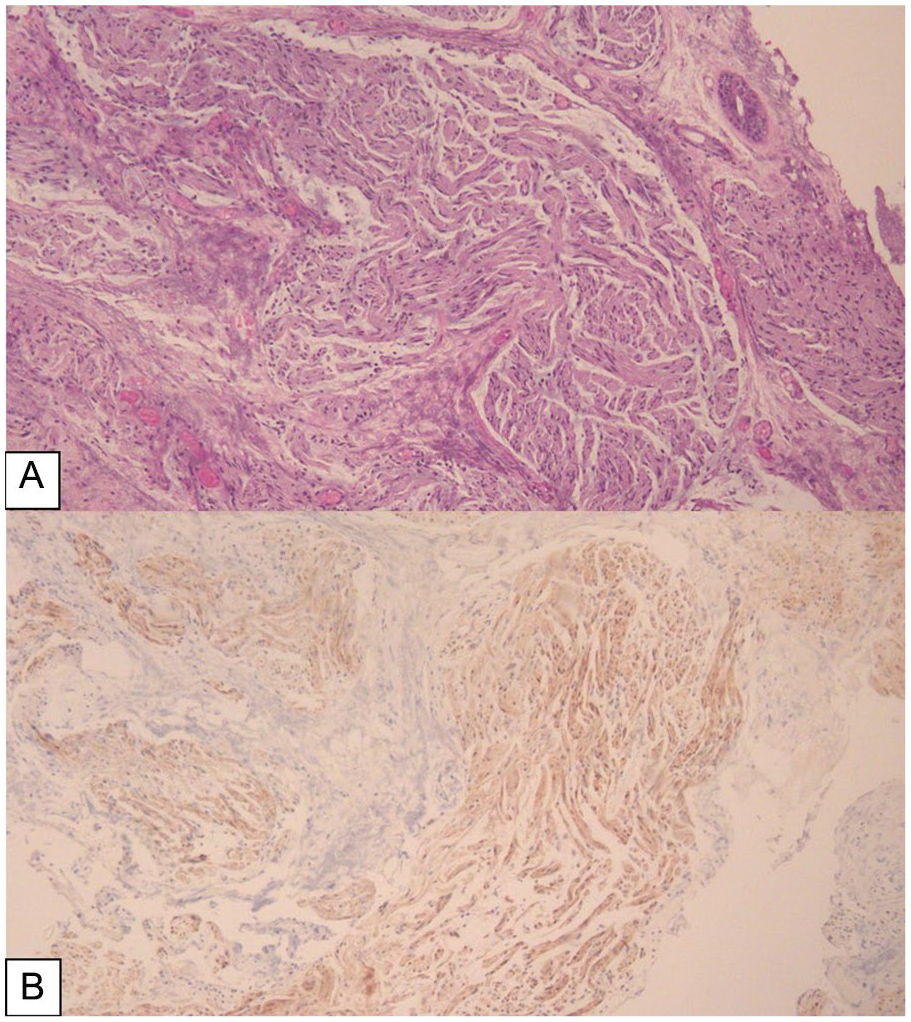
Pathology slides of laryngeal specimen taken during the laryngoscopy/bronchoscopy. (A) Well-circumscribed collection of spindle cells surrounded by multiple vessels, consistent with a mucosal neuroma (H&E, ×10). (B) Immunohistochemical staining highlights S-100 positivity confirming neural nature of spindle cells (S-100, ×10). H&E, hematoxylin and eosin.
The patient was later discharged with no complications and started on immunotherapy for residual disease as adjuvant therapy. Genetic testing for the entire family was recommended.
Discussion
MEN type 2 is divided into 3 subtypes: MEN2A, MEN2B, and familial MTC. 7 The clinical course of MEN2B is the most aggressive of the MEN 2 neoplasias characterized by MTC, pheochromocytoma, mucosal neuromas, ganglioneuromatosis, and marfanoid appearance developing relatively at an early age. 8 Mucosal neuromas of the larynx are extremely rare, with our case being the first report of laryngeal neuromas in the Middle East. Globally, there has been limited documentation of mucosal neuromas in the larynx and its exact incidence of laryngeal mucosal neuromas is uncertain.
In our case, the laryngeal neuromas were accidentally pointed out during general anesthesia causing noticeable stridor on extubation and requiring re-intubation due to airway obstruction.
To the best of our knowledge, there are only 7 case reports that have described laryngeal mucosal neuromas as part of MEN2B. The first reported case in 1988 by Lesourd et al described the case of a 28-year-old women with MEN2B in whom multiple laryngeal mucosal neuromas were identified on autopsy. 9 Similar to our case, Ghosh et al reported the case of an 11-year-old girl diagnosed with MEN2B in whom laryngeal neuromas were accidentally found during general anesthesia and were then excised. 10 Also, Inoue et al reported a case of MEN2B with laryngeal mucosal neuromas after intubation. 11 Kudo et al described bilateral arytenoid mucosal neuromas, in a 23-year-old woman with MEN2B, that were extirpated during her thyroidectomy for MTC. 12 There are reported cases of patients with MEN2B who presented with laryngeal symptoms years after thyroidectomy and were found to have multiple laryngeal mucosal neuromas throughout the glottis and subglottis.13-15
MEN2B is a rare disease, and MEN2B with laryngeal mucosal neuromas is an even rarer entity. It is possible that there are potentially more cases that have not been diagnosed clinically or reported in the literature. These laryngeal neuromas can potentially compromise the airway in patients with MEN2B. Therefore, it is critically important for ENT specialists to recognize laryngeal mucosal neuromas for proper airway management and for suspecting MEN2B if such a diagnosis has not already been made.
We suggest keeping a low threshold when a patient presents with symptoms of dysphonia and dysphagia in the context of a MEN2B diagnosis. We favor a systematic approach where flexible laryngoscopy factors into the management algorithm, especially when scheduling these patients for surgery.
Conclusion
Despite its rarity, MEN2B syndrome poses significant clinical challenges due to its variable presentation and potential for serious complications. When suspecting MEN2B and planning for any surgical intervention under general anesthesia, always rule out laryngeal neuromas to prevent airway problems during intubation/extubation. Early detection, genetic counseling, and multidisciplinary management are essential for optimizing patient care and improving long-term outcomes for individuals affected by this complex condition.
Footnotes
Data Availability Statement
The data included in this study are available from the corresponding author, (R.A.B.), on reasonable request.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval
Our institution does not require ethical approval for reporting individual cases or case series.
Informed Consent
Written informed consent was obtained from the individual(s) for the publication of any potentially identifiable images or data included in this article.