
Abstract
Objective:
This review set out to examine the applicability of transcutaneous laryngeal ultrasonography (TLUSG) for the assessment of laryngeal function after thyroidectomy.
Methods:
An integrative review of the literature was performed using Medline/PubMed, LILACS, and SciELO databases. The methodological quality of the studies was analyzed using the appraisal tool for cross-sectional studies.
Results:
All 8 included articles investigated laryngeal function with regard to the risk of vocal fold immobility after thyroidectomy. The results regarding the diagnostic power of TLUSG for this assessment are controversial, and there is a tendency to use this examination as a screening procedure for subsequent confirmation by flexible laryngoscopy.
Conclusions:
Transcutaneous laryngeal ultrasonography is a viable, noninvasive, and useful tool to assess laryngeal function after thyroidectomy, but current available evidence suggests that it does not replace flexible laryngoscopy for the diagnosis of vocal fold immobility.
Introduction
Ultrasonography (USG) is a technique in which high-frequency acoustic echoes are reflected inside the human body and converted into graphic signals that, in turn, are electronically decoded on a displayed image that can be recorded and used for immediate or later analysis. 1 Overtime, advancements in USG have allowed more detailed investigations that can be assessed both quantitatively and qualitatively, not only from a morphological point of view but also from a functional one. 2
Transcutaneous laryngeal ultrasonography (TLUSG) is a technique that specifically assesses the neck structures. 3 -6 It is considered to have an applicability index of over 90% 4 and does not expose the patient to radiation. 7,8 According to some studies, TLUSG can be used as an alternative to fiberoptic flexible laryngoscopy 9 and can provide real-time imaging to examine laryngeal function. 8,10 In this regard, TLUSG has become an alternative to investigate laryngeal sequelae in surgical cases involving the anterior cervical region, such as a thyroidectomy. 3,4,7
Thyroidectomy is the preferred surgery for the treatment of certain thyroid diseases 11 and is one of the most frequently performed procedures in the world. Although it is considered a safe procedure, with low morbidity and mortality close to 0%, 12 it can cause laryngeal immobility or vocal fold immobility as iatrogenic factors, which compromise the vocal pattern, impair swallowing, and lead to significant complications in the patient’s quality of life. 13 It is also evident in the literature that this type of iatrogenesis occurs in 1.8% of cases, 1.4% of which are transient and 0.4% permanent, and in many cases results in dysphonia, dysphagia, and dyspnea. 14
Laryngeal examination using a flexible laryngoscope is still considered the reference standard to assess vocal fold function before and after thyroidectomy. 15,16 By contrast, TLUSG is not invasive, uncomfortable, or painful and has been described by some studies as a viable and reliable examination to assess laryngeal function. 4,17,18 Since the test may be performed in real-eating situations and even at the bedside, TLUSG has also been used for the assessment of some biomechanical swallowing parameters to complement the functional assessment of patients with oropharyngeal dysphagia. 19,20
Although the literature describes TLUSG as an alternative to assess the functional integrity of the larynx, it is still necessary to better understand the situations in which this examination can be effectively included in thyroidectomy clinical routine. Therefore, the aim of this study was to seek scientific evidence for the applicability of TLUSG to assess laryngeal function after thyroidectomy.
Materials and Methods
This integrative literature review utilizing the following steps 21 : (1) preparation of the research question; (2) definition of the descriptors and keywords; (3) selection of articles according to the eligibility criteria; (4) collection, data extraction, reading, and critical analysis of articles; (5) interpretation and discussion of the results; and (6) synthesis of the information and presentation of the review.
Search Strategy
The article search was based on the following research question: “What is the applicability of TLUSG for the assessment of laryngeal function after thyroidectomy?” The Medline/PubMed, LILACS, and SciELO databases were consulted. The articles were obtained by cross-referencing the following search terms: (“ultrasonography” OR “ultrasonics” OR “laryngeal ultrasonography” OR “TLUSG” OR “laryngeal ultrasound” OR “ultrasound” OR “transcutaneous laryngeal ultrasonography”) AND (“thyroidectomy” OR “thyroid-surgery”). The search considered articles published between January 2008 and July 2018 in Portuguese, English, and Spanish.
Eligibility Criteria
Articles were included that addressed TLUSG as a diagnostic tool for laryngeal function in patients undergoing partial or total thyroidectomy. The following publication and study types were excluded: literature reviews, editorials, letters to the editor, and conference proceedings; studies using TLUSG only for the diagnosis of thyroid nodules or therapeutic purposes; animal studies; studies that indicated the use of TLUSG in the methods, but did not describe the examination’s findings in the results; and studies that included patients in the sample who underwent other types of surgery in the neck region.
Data Collection and Analysis Procedures
Initially, 2 reviewers independently conducted a database search and selected articles by reading the title and abstract. Duplicate articles were excluded, and the remainder were read in their entirety. In cases of disagreement, a third reviewer was asked to make a decision. After defining studies that met the eligibility criteria, the following data were extracted to comprise the analysis matrix: author, year of publication, place of origin, study objectives, sample characteristics, methodological procedures (including examinations performed, time of assessment, type and positioning of the transducer used, and blinding of evaluators), and conclusions. The methodological quality of the studies was analyzed by appraisal tool for cross-sectional studies (AXIS), a critical analysis tool used to assess the quality and risk of bias in cross-sectional studies. 22 This was followed by analysis and critical discussion of the results, together with a synthesis of the information obtained and presentation of the review in this article.
Results
A total of 2697 articles were initially located. After applying the eligibility filters, the final sample comprised 8 articles. The selection process is shown in Figure 1.
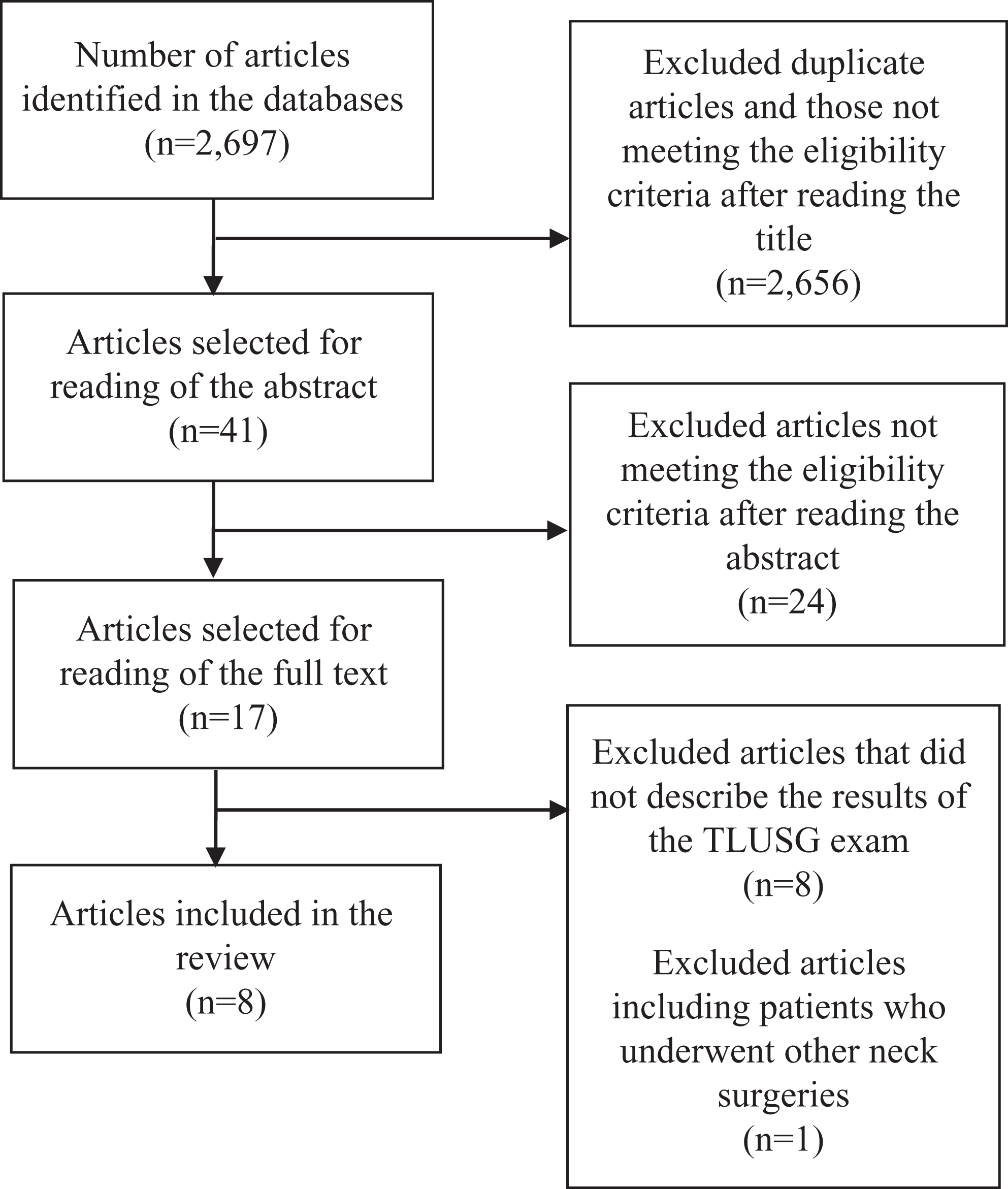
Article selection flowchart.
The selected studies were analyzed according to the findings presented in the analysis matrix (Table 1). The methodological quality of the studies included in this review is presented in Table 2, according to the AXIS tool criteria.
Summary of Studies Using Transcutaneous Laryngeal Ultrasonography (TLUSG) to Assess Laryngeal Function After Thyroidectomy.
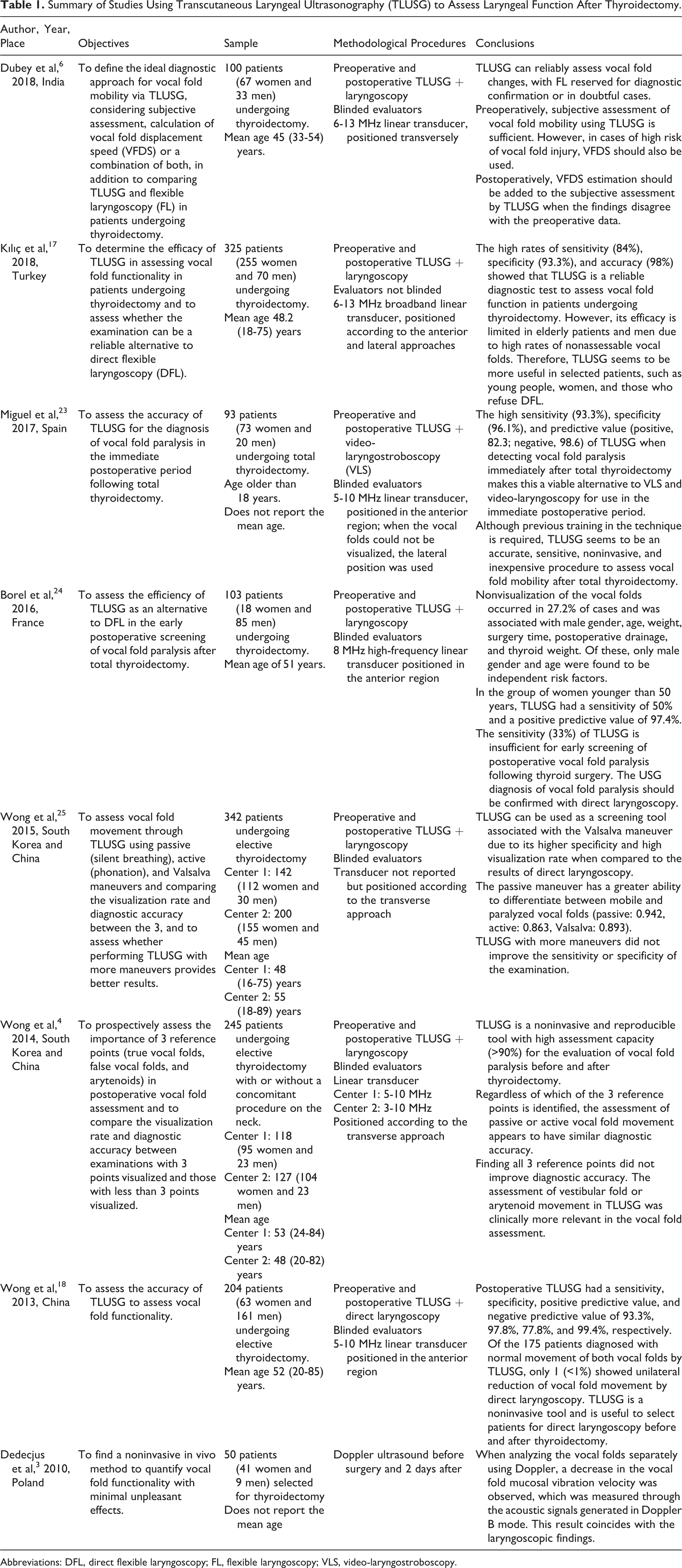
Abbreviations: DFL, direct flexible laryngoscopy; FL, flexible laryngoscopy; VLS, video-laryngostroboscopy.
Classification of Methodological Quality of the Studies Using the Appraisal Tool for Cross-Sectional Studies (AXIS).a
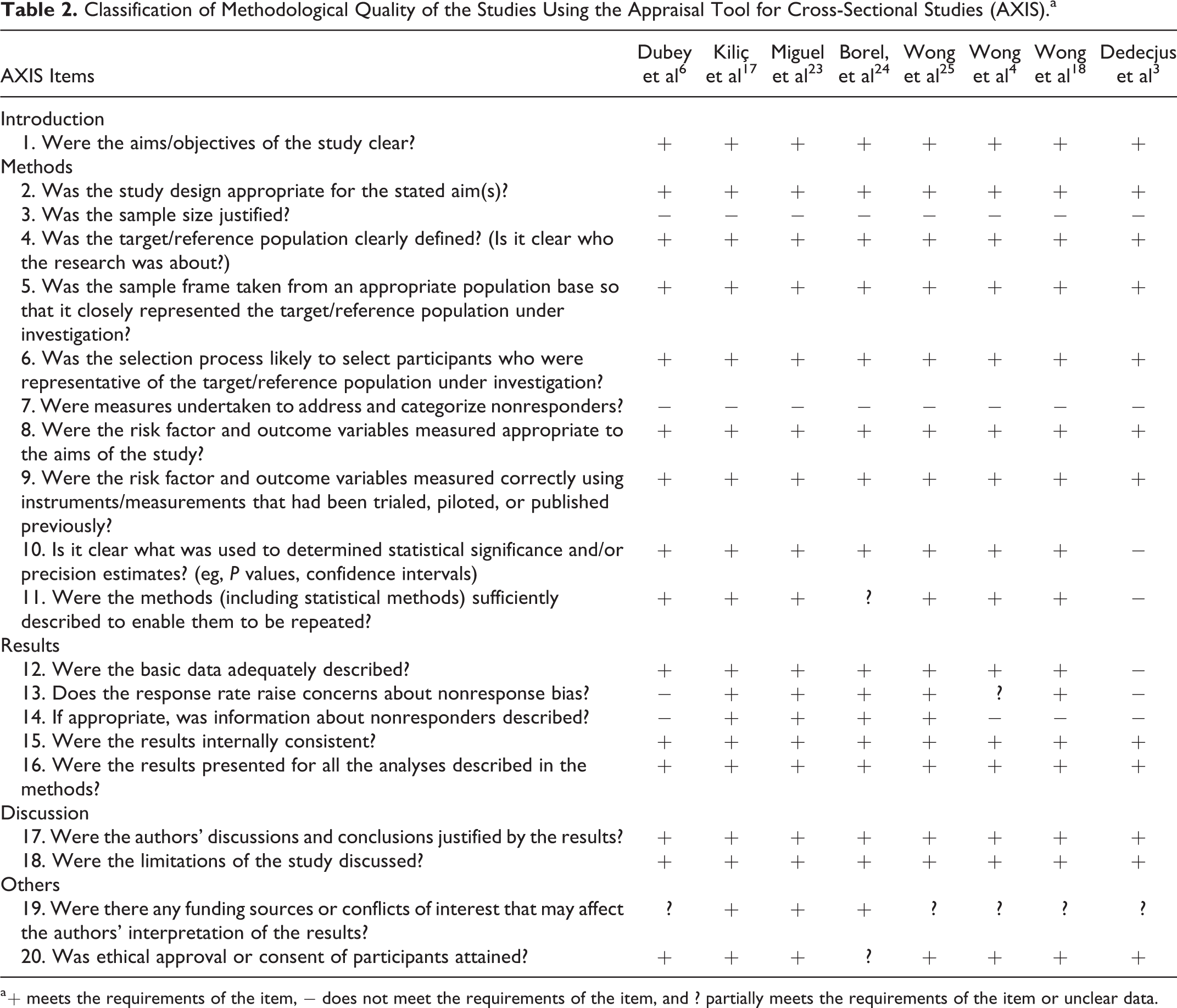
a + meets the requirements of the item, − does not meet the requirements of the item, and ? partially meets the requirements of the item or unclear data.
Discussion
This review included 8 studies conducted in Eastern and Western European and Asian countries that involved research using TLUSG to assess laryngeal function after thyroidectomy. Two of these were partnerships between institutions in South Korea and China, 4,25 and 1 was based in China, 18 1 in Japan, 1 in Turkey, 17 1 in Spain, 23 1 in France, 24 1 in Poland, 3 and 1 in India. 6 No studies based on the Americas were found.
With regard to the year of publication, the first article was published in 2010. 3 There was 1 article published in 2013, 18 1 in 2014, 4 1 in 2015, 25 1 in 2016, 24 1 in 2017, 23 and 2 in 2018. 6,17 Starting in 2013, publications in this field emerged on an annual basis, which demonstrates the scientific community’s interest in contributing more systematic data on laryngeal function after thyroidectomy to find an alternative method of performing this investigation.
With regard to gender and age, the diagnosis of thyroid diseases is prevalent in females and those with advanced age. 26 Therefore, a predominance of female and elderly volunteers was expected in all studies included in this review.
In general, the studies used TLUSG after thyroidectomy to investigate vocal fold mobility with regard to the risk of immobility associated with the surgical procedure. Thyroidectomy is one of the most common surgeries in the world, and recurrent laryngeal nerve (RLN) paralysis is a significant complication 27 that has a negative impact on voice, swallowing, and quality of life. 13,28
Most studies compared the results of TLUSG with laryngoscopic assessment using flexible or rigid fiberscopes, 4,6,17,18,24,25 which was expected because laryngoscopic examination is the reference standard when assessing RLN function and vocal fold mobility before and after thyroidectomy. Only 1 study used videostroboscopy for this purpose. 23
In terms of methodology, blinding attempts to eliminate possible biases that may arise due to the behavioral and psychological aspects involved in human research. In most of the studies included in this review, 4,6,18,23,24,25 the evaluators were blinded to the results of the examinations, which is a necessary precaution when determining the actual sensitivity and specificity rates required to reliably diagnose vocal fold immobility.
Overall, the methodological quality of the studies included in this review was satisfactory according to the AXIS tool criteria. Items that were not properly covered will require attention in future studies on the subject, especially with regard to the description of sample size calculation and the approach to nonresponders or nonassessed patients. Such information is important to leverage evidence and was omitted in some articles. Even fundamental issues such as the existence of funding sources, conflicts of interest, and the participants’ ethical approval were also unclear in some studies. 3,4,6,18,24,25
The transducer type used in the studies was linear, but the bandwidth varied, ranging from approximately 5 to 10 MHz. The most common position was transverse in the anterior or lateral region, but vertical positioning has also been proposed in other studies. Positioning appears to be a variable that should be better studied in TLUSG, given that some researchers 29 state that the viewing rate of a lateral vertical procedure is better than that of a middle transverse procedure. The authors argue that the reference points used for the transverse approach are the true vocal folds and that these are more difficult to visualize due to the poor ultrasonic permeability of air. Moreover, the transverse approach uses the viewing of arytenoid cartilage as a reference. Instead of being classified according to the reduction in vocal fold mobility, RLN paralysis or paresis is classified based on fixation of the muscular process of the arytenoid cartilage. The limitation of this procedure is the impossibility of synchronous observation of the right and left vocal fold movements, which increases the examination time and presents greater difficulty in detecting differences in vocal fold movements. 29
More studies are needed to further the discussion on the tasks requested during the examination. One study showed that the Valsalva maneuver permitted a better viewing rate and specificity. 25 This same study compared this and 2 other maneuvers: a passive maneuver (normal breathing) and an active maneuver ([a] vowel phonation). It was found that TLUSG can be used as a screening tool when using the Valsalva maneuver, which avoids subjecting patients to direct laryngoscopy. 25
Two studies 13,18 assessed the accuracy of TLUSG for the diagnosis of vocal fold immobility after total thyroidectomy. De Miguel et al 23 investigated the accuracy in the immediate postoperative period. The examination was performed with the transducer positioned transversally, and a passive maneuver (slow breathing) and active maneuver ([a] vowel phonation) were used. When the vocal folds were not visible, the lateral approach was used. Transcutaneous laryngeal ultrasonography was performed after the surgical procedure in the postanesthetic recovery room. The results showed that TLUSG is a viable option compared to direct laryngoscopy and videostroboscopy, with a sensitivity of 93.3% and specificity of 96.1%, and can be performed in the immediate postoperative period.
Wong et al 18 used the same methodology proposed in the study described above 23 at between 7 and 10 days after thyroidectomy. They found that TLUSG is a noninvasive and useful tool, with a sensitivity of 93.3% and specificity of 97.8% for selecting patients to undergo direct laryngoscopy. The results of these 2 studies showed that TLUSG is feasible and useful, both in the immediate and late postoperative periods, for patients undergoing thyroidectomy.
In contrast, the results of 2 other studies 18,24 showed that TLUSG is insufficient for the definitive diagnosis of vocal fold immobility after thyroidectomy. Borel et al 24 assessed the efficiency of this examination as an alternative to direct flexible laryngoscopy in the first or second postoperative day. Due to the relatively poor performance of TLUSG for the diagnosis and assessment of vocal fold paralysis, with a sensitivity of 33%, a specificity of 95%, a positive predictive value of 42%, and a negative predictive value of 89%, the authors reported that diagnosis by TLUSG should always be confirmed by direct flexible laryngoscopy and that it may be useful only as a means of screening for subsequent referral to laryngoscopy.
Another study 18 evaluated the accuracy of TLUSG to assess pre- and post-thyroidectomy vocal fold function. It revealed that when the examination was performed after surgery, it had a sensitivity, specificity, positive predictive value, and negative predictive value of 93.3%, 97.8%, 77.8%, and 99.4%, respectively. Despite the high values, the study has some limitations, such as the low number of patients with vocal fold immobility. The authors suggested that TLUSG should be used as a tool for patient selection before and after thyroidectomy and should not be used as an alternative to direct laryngoscopy.
Only one study 3 reported a sensitivity of TLUSG of 100% when comparing the preoperative and postoperative period. The assessment criterion was a 50% reduction in vocal fold displacement velocity between the preoperative and postoperative examination. This method detected all patients with postoperative vocal fold immobility. However, this was a pilot study with a small number of cases, and the authors were unable to clearly define the association between the vocal fold displacement speed values and a diagnosis of vocal fold immobility.
Because the results regarding the diagnostic power of vocal fold immobility by TLUSG are controversial, there is a tendency to consider TLUSG as a screening procedure 18,24,25 for subsequent diagnostic confirmation by direct laryngoscopy, thus avoiding the need for an invasive procedure in cases where it would not be necessary. Laryngoscopy, whether direct or flexible, remains the most specific test to confirm the diagnosis of vocal fold immobility, with a success rate of 99%. 24
Some studies indicate that the male gender and advanced age are variables that may interfere with good visualization during the TLUSG examination. 17,24 The different angle in men and calcification of the structures in the elderly patients are factors that limit the performance of the test and that are strongly associated with the number of patients with vocal folds classified as nonassessable by TLUSG.
Although TLUSG is noninvasive and readily available, 6 it requires acquisition of knowledge, practice, and accumulating experience to achieve an efficient, accurate, and proficient examination. 30 A study by Wong et al 30 investigated the learning curve of TLUSG in vocal cord assessment. After a short standardized training program, 8 surgical residents with no previous experience in ultrasound technique were able to master TLUSG skills after 7 examinations and assess vocal cord function consistently and accurately after 40 TLUSG. 30 Apart from being an easy-to-learn examination, 6 TLUSG requires initial training to gain proficiency in performing the technique. 6,23 In view of this, there is a limitation if no professional with experience is available to perform the training.
The studies included in this review investigated laryngeal function after thyroidectomy and considered vocal fold immobility as a major negative impact on the voice, which affects patients’ social relationships and quality of life. This review found no evidence from the selected studies on the applicability of TLUSG for other purposes, even though the literature indicates the use of TLUSG in other populations as a noninvasive method to assess parameters related to swallowing, such as tongue thickness 31 and hyolaryngeal displacement. 19,32,33 Only one study 23 briefly discussed the relationship between vocal fold immobility and dysphagia, which is characterized by episodes of increased tracheal aspiration. In addition to the voice, swallowing can be affected after thyroidectomy, 34 that is, TLUSG may be a promising procedure for the investigation of this function in these patients.
Conclusions
Transcutaneous laryngeal ultrasonography is a viable, noninvasive, and useful method to assess laryngeal function after thyroidectomy, especially changes in vocal fold mobility. However, it is not possible to confirm that TLUSG can replace direct flexible laryngoscopy for the diagnosis of vocal fold immobility. Although the results are controversial, TLUSG provides a good viewing rate of laryngeal structures, which should encourage further research, including the use of this procedure for other purposes such as analyzing swallowing-related parameters.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.