
Abstract
Granulomatosis with polyangiitis (GPA), formerly Wegener’s granulomatosis, commonly presents primarily with otitis media and hearing loss, as well as upper and lower respiratory symptoms. However, facial nerve paralysis is a rare manifestation of this uncommon necrotizing vasculitis. We report a patient with facial paralysis accompanied by otitis media. In further studies, our patient was diagnosed with GPA, which was neglected before. In such a presentation, acute suppurative otitis media is the most likely cause of the facial paralysis, but GPA must also be considered, especially in cases with new-onset, painful serous otitis, acute otitis media, or pale granulation tissue in the middle ear, in adults with no previous history of Eustachian tube dysfunction.
Introduction
Granulomatosis with polyangiitis (GPA), formerly Wegener’s granulomatosis, is an autoimmune disorder, characterized by necrotizing granulomatous inflammation with pauci-immune vasculitis, typically affecting small vessels. GPA is part of a spectrum of disease states, labeled antineutrophil cytoplasmic antibody (ANCA) associated vasculidites (AAV). Other components of AAV include granulomatosis with polyangiitis, microscopic polyangiitis, and eosinophilic granulomatosis with polyangiitis (formerly known as Churg Strauss syndrome). 1
GPA typically manifests in the upper and lower respiratory tracts and kidneys; however, any organ can be affected. Upper respiratory tract involvement occurs in 70% to 100% of cases 2 with symptoms including bloody rhinorrhea, rhinosinusitis, cough, dyspnea, and hemoptysis. Sinonasal symptoms are found in almost all cases. 3 Prior publications have reported otologic symptoms present in approximately 35% (range, 19%-61%) of cases. 4 In fact, otologic symptoms can be the initial manifestations of GPA for many patients. 5
Case Presentation
A 60-year-old female presented to us with a 1-month history of right-sided facial paralysis, maximal conductive hearing loss, and a purulent ear discharge. The patient had initially presented to an outside institution, where she was diagnosed with otitis media and underwent an urgent myringotomy and pressure equalization tube placement. During the procedure, granulation tissue was removed from the external auditory canal. Purulent discharge was noted in the middle ear space and a collar button tube was then inserted without difficulty.
On physical examination, she was noted to have a tympanic membrane perforation with a dislocated malleus (Figure 1) with grade 6/6 right facial weakness. A computed tomography (CT) scan of the temporal bone was reviewed and showed a well-developed mastoid which was fully opacified with a dislocated malleus (Figure 2). The patient was sent for laboratory testing [erythrocyte sedimentation rate (ESR), c-reactive protein (CRP), and antineutrophil cytoplasmic antibody (ANCA)], magnetic resonance imaging (MRI) of the internal auditory canals and facial nerve electromyography (EMG).
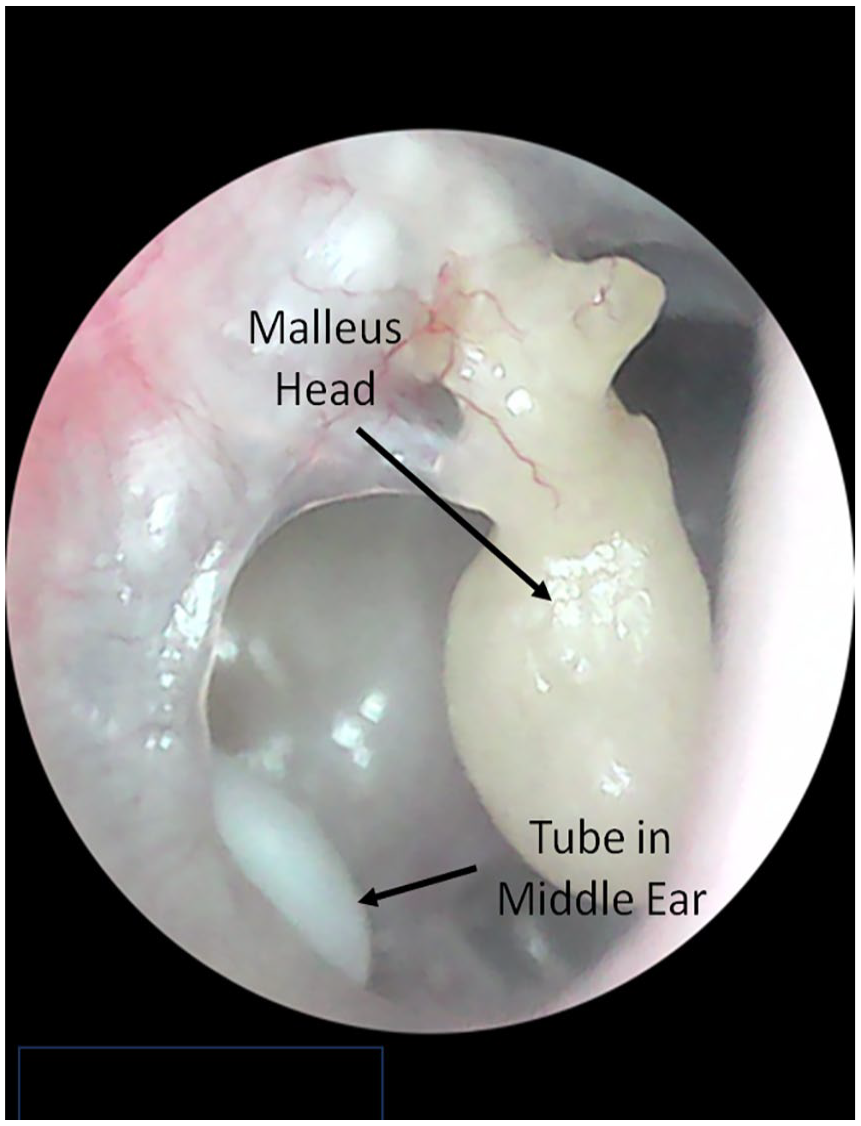
Otoscopic image of the patient’s tympanic membrane showing perforation and the dislocated malleus head. The previous white collar button tube can be seen in the middle ear.
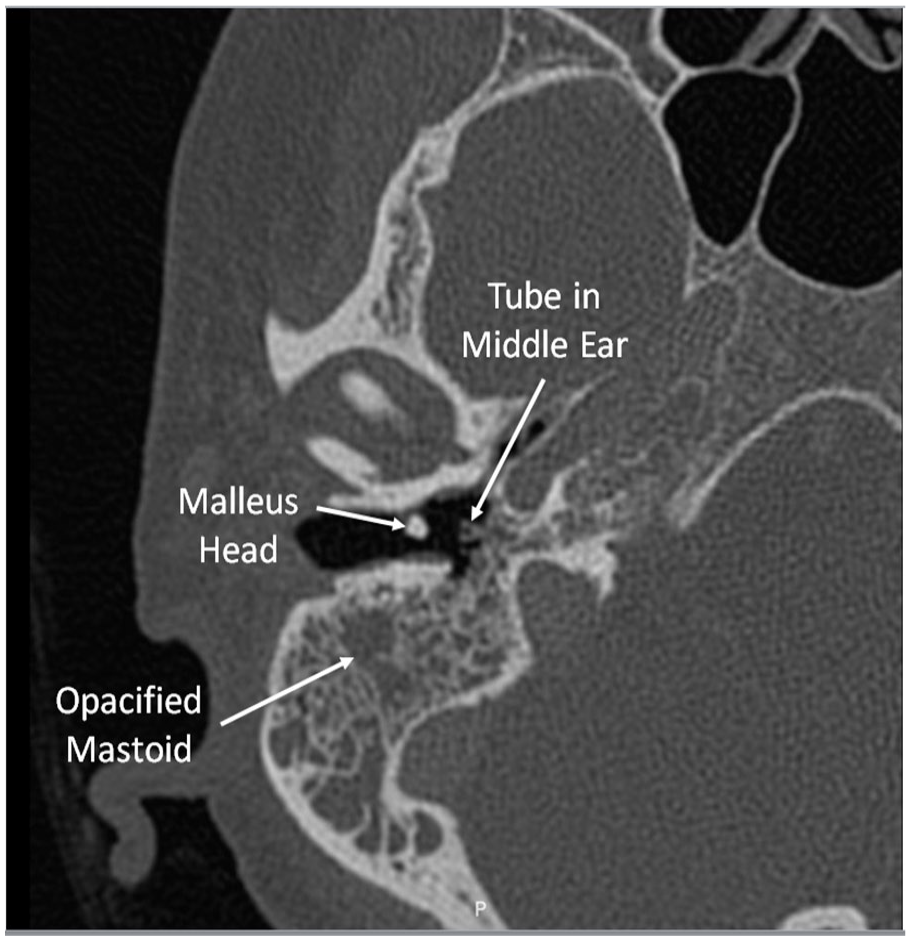
Axial CT of temporal bones showing the dislocated malleus head and opacification of the mastoid on the right side.
The patient did not perform the laboratory testing or EMG but had the MRI performed. The MRI showed enhancement of the mastoid mucosa and the dura (Figures 3 and 4). Due to the concern of the radiologist for potential early meningitis, cortical mastoidectomy was performed which found pale granulation tissue (Figure 5). ANCA blood testing was performed and was noted to be positive.
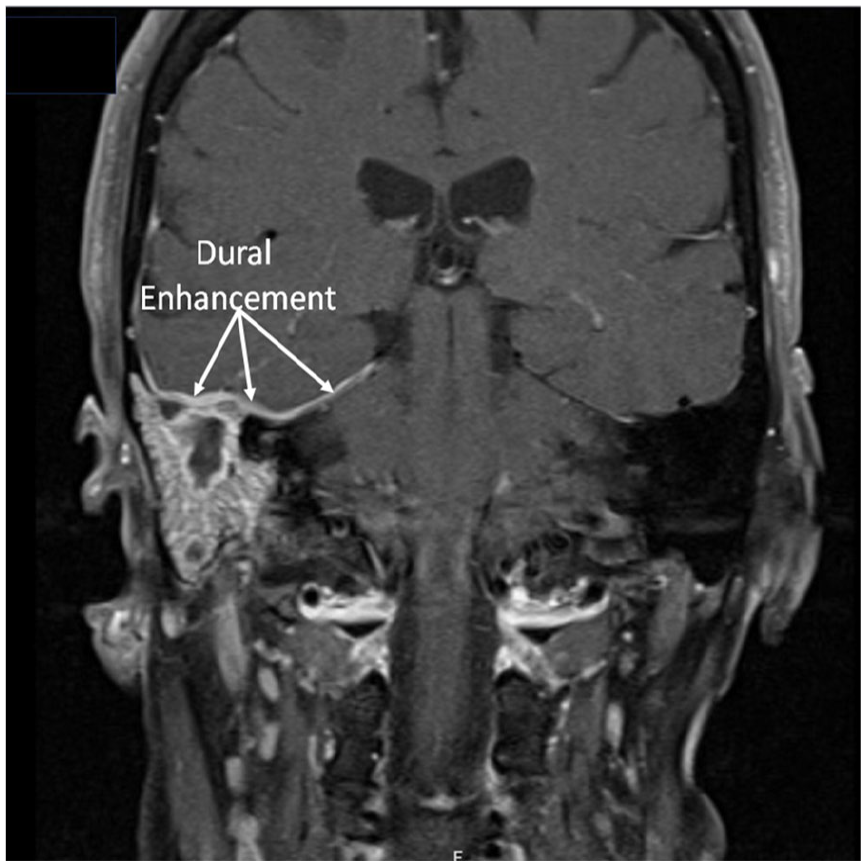
Coronal T1 post-gadolinium MRI of internal auditory canals showing enhancement of the mastoid mucosa and dura (arrows).
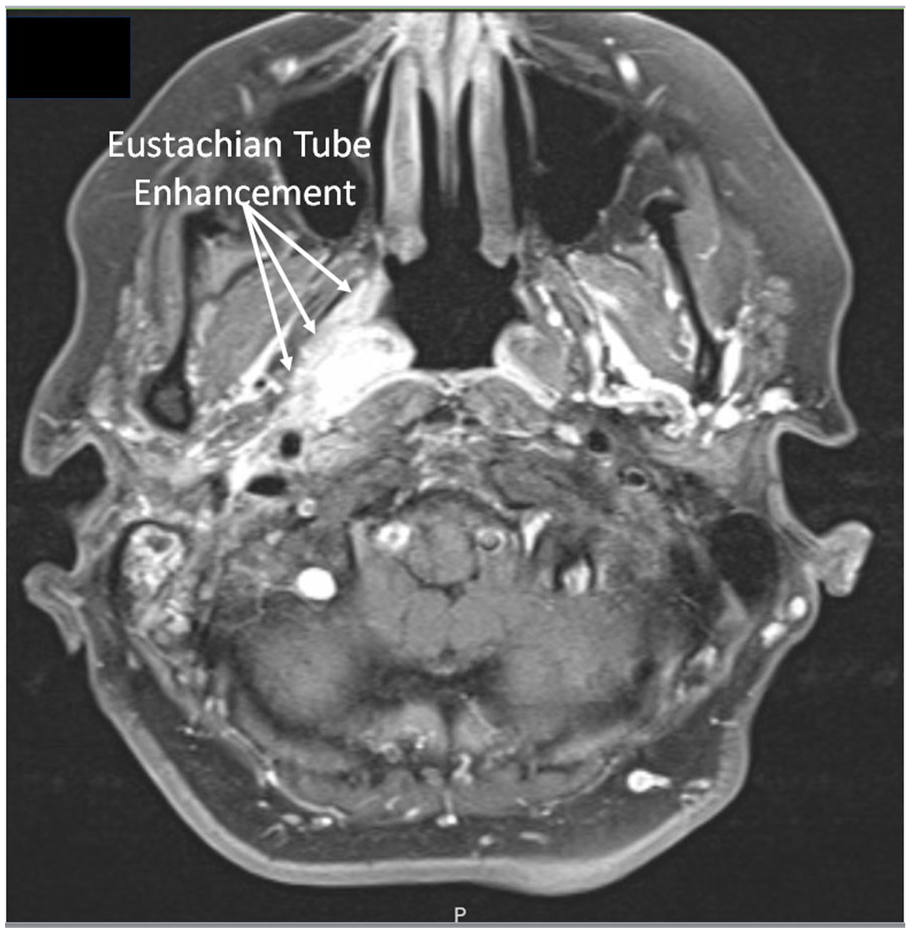
Axial T1 post-gadolinium MRI of internal auditory canals demonstrating intense inflammation in the right Eustachian tube.
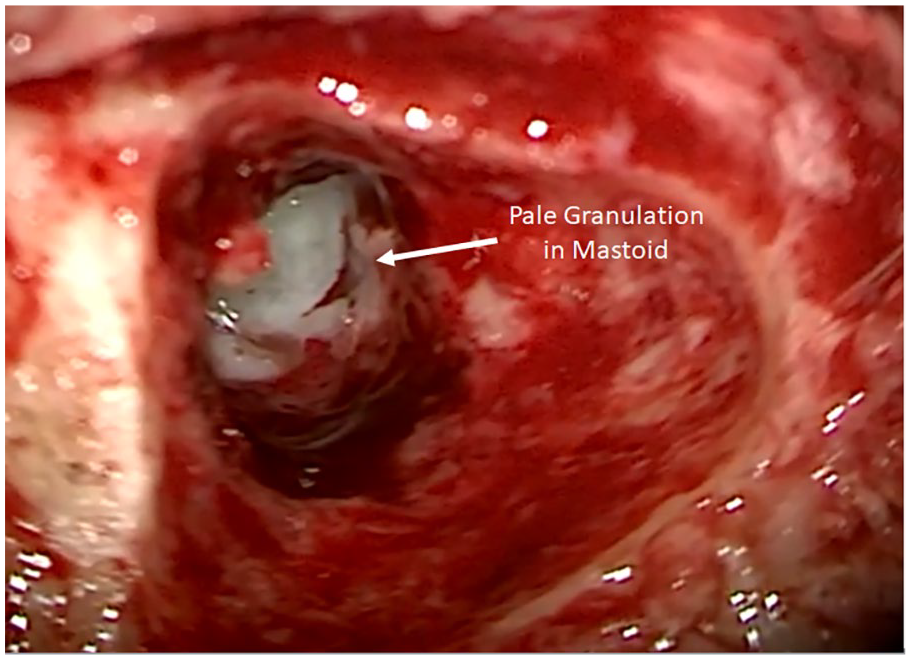
Intraoperative image of the right mastoidectomy showing pale granulation tissue in the mastoid which is characteristic of GPA.
Discussion
This case underscores the importance of considering and thoroughly evaluating GPA in adult patients presenting with acute otitis media and facial paralysis. In addition, in patients with serous otitis media and otalgia, GPA should be suspected and a workup should be performed. In the United States, GPA has 5 years prevalence of 2.6 to 3.2 cases per 100,000 persons. 6 In an otolaryngology or tertiary neurotology practice, GPA could conceivably present even more frequently, suggesting that GPA may have been missed prior to referral due to a low index of suspicion. Several case series have documented that otologic symptoms as the primary manifestations of GPA7-9; therefore, GPA should always be considered in the differential diagnosis of inflammatory middle ear disease with or without facial paralysis in adults with no previous otitis media history.
In adults with no previous history of Eustachian tube dysfunction painful serous otitis, acute otitis media, or pale granulation tissue in the middle ear raises the suspicion for GPA. This is especially true if the patient presents with facial paralysis in combination with the above symptoms. When suspicious, it is highly recommended that the patient be tested for ANCA, ESR, and CRP. We additionally obtain a urinalysis as the inflammatory markers (ESR, CRP, and ANCA) can fluctuate with the disease severity but the urinalysis can show signs of damage to the kidneys from GPA. It is important to note that ANCA titers may be negative in patients with GPA, and reevaluation over time is recommended when clinical suspicion is high. While ESR and CRP are nonspecific markers, elevated results in the setting of negative ANCA titers should not eliminate the possibility of GPA. A biopsy of granulation tissue should be performed to aid in confirming diagnosis if tissue can be obtained. Urinalysis should also be considered to evaluate for proteinuria or hematuria, which are common presentations of GPA in urinary system involvement. Finally, a nasal endoscopy to evaluate for granulation tissue in the nasal cavity should be performed.
Imaging modalities are also informative as CT of the temporal bone can help to evaluate the extent of middle ear and mastoid involvement and MRI of the internal auditory canal with and without gadolinium can reveal potential masses or inflammation that may be responsible for facial paralysis. Upon diagnosis, GPA patients generally respond well to immunosuppressive therapy, though in our experience the facial nerve recovery from a grade 6 paralysis is generally no better than grade 3 in the GPA population.
Conclusion
Maintaining a high index of suspicion for GPA and other autoimmune conditions in the setting of otitis media and facial paralysis is crucial for timely diagnosis and management. Painful serous otitis, acute otitis media, or pale granulation tissue in the middle ear signal the possibility of GPA in adult patients with no previous history of Eustachian tube dysfunction. A comprehensive head and neck examination including nasal endoscopy as well as laboratory tests, including ANCA titers, ESR, CRP, and urinalysis will aid in the diagnosis. In cases where ANCA titers are negative but clinical suspicion remains high, repeating ANCA titers is recommended to address the possibility of a false-negative result. Imaging studies provide additional data that may aid in the diagnosis. Dural enhancement is often seen in patients with GPA with significant mastoid involvement. A biopsy of granulation tissue should be performed when accessible while patients are off immunosuppressive agents.
Footnotes
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Dr. Hamid R. Djalilian has equity in NeuroMedCare LLC, MindSet Technologies, Elinava Technologies, and Cactus Medical LLC. He is a consultant to NXT Biomedical. The other author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article. Our institution does not require ethical approval for reporting individual cases or case series.
Data Availability Statement
All data relating to the case have been shared in the report.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.