
Abstract
Introduction
With the widespread adoption of screening programs and advancements in thyroid ultrasound examination and fine needle aspiration biopsy (FNAB) techniques, the prevalence of papillary thyroid carcinoma has been steadily rising over the years. Among them, the proportion of papillary thyroid microcarcinoma (PTMC) with a tumor maximum diameter ≤10 mm has exceeded 50%.1,2 Currently, there is considerable controversy regarding the treatment for PTMC, ranging from active surveillance to thyroidectomy. Although surgery remains the primary method for treating PTMC, it is associated with significant surgical trauma, potential damage to surrounding nerves and parathyroid glands, postoperative scarring, and the lifelong need for levothyroxine supplementation. On the other hand, percutaneous microwave ablation (PMWA) is a minimally invasive procedure whereby microwave electrodes are percutaneously inserted into the tumor under ultrasound guidance, inducing tumor tissue degeneration, necrosis, and inactivation through thermal effects. This approach offers several advantages, such as fewer postoperative complications, smaller incisions, faster recovery, and improved aesthetics. 3 Microwave ablation (MWA) has demonstrated good safety and efficacy in treating benign thyroid nodules. Consequently, many researchers have begun to apply MWA technology to the treatment for PTMC, particularly in patients who refuse surgery, cannot undergo regular follow-up, or experience anxiety. However, MWA is employed for the inactivation of cancerous nodules without excising the surrounding lymph nodes, making it a non-tumor radical treatment. Therefore, there is considerable debate about whether MWA can be considered a routine treatment option. Thus, this study aims to perform a comparative analysis of the efficacy disparities between PMWA and surgical intervention for PTMC, to objectively assess the benefits and drawbacks of these 2 treatment approaches, and offer guidance for clinical decision making.
Materials and Methods
Search Methods
A detailed investigation was undertaken across Embase, PubMed, Cochrane Library, Web of Science, CNKI, VIP Database, and Wanfang Database up to December 2023 for clinical trials investigating ultrasound-guided PMWA or thyroidectomy as treatments for PTMC, without language restrictions. Medical Subject Headings (MeSH) terms and unstructured text terms were amalgamated for the search.
Inclusion and Exclusion Criteria
Inclusion criteria
Studies involving patients diagnosed with papillary thyroid carcinoma by ultrasound-guided FNAB or core needle biopsy.
Single nodules with a maximum tumor diameter of ≤10 mm.
No cervical lymph node metastasis (LNM) detected.
Thyroid nodules not invading the thyroid capsule or adjacent organs.
Original research articles on the treatment for PTMC using PMWA compared to conventional thyroidectomy, such as prospective or retrospective studies.
PMWA was administered to the experimental group and conventional thyroidectomy in the control group.
Reporting of at least 1 relevant parameter.
Exclusion criteria
Inability to access the full text.
Studies with incomplete data extraction.
In case of duplicate publications, only the most comprehensive and longest follow-up data were selected.
Studies with inconsistent outcome indicators.
Literature Screening and Bias Risk Assessment
A cumulative count of 442 articles was obtained, and the literature screening was independently conducted by 2 reviewers. All disparities were reconciled following consultation with a tertiary reviewer. The included studies were reviewed for ethical approval and informed consent from the patient. After the first stage, the 2 reviewers assessed the articles and decided whether they met the inclusion criteria. Additional pertinent studies were identified through a thorough examination of the references cited in the included studies. Any discordance in inclusion criteria was settled through a consensus reached with the tertiary reviewer in the review team.
Data Extraction
Two authors independently verified and extracted the literature data, which included fundamental details such as the primary author, publication year, country of origin, and study design, study duration, number of patients in randomized groups, number of patients included in the analysis, group allocation, main study results, and experiential requirements. Outcome indicators included: (1) Surgical efficacy: postoperative recurrence or LNM; (2) factors related to surgical treatment [including comparison of surgical time (minutes), intraoperative blood loss (ml), postoperative hospital stay (days), and hospitalization costs (yuan)]; (3) incidence of postoperative complications; (4) thyroid hormone levels 30 days postoperatively, including free triiodothyronine (FT3), free thyroxine (FT4), and thyroid-stimulating hormone (TSH); (5) comparison of pre- and postoperative physiological health score physical component summary (PCS)/mental component score (MCS)/short-form health survey (SF-36) scores; (6) tumor volume changes and tumor volume reduction rate.
Statistical Analysis
Continuous data were expressed as mean differences (MD) along with their corresponding 95% confidence intervals, whereas binary data were expressed as relative risk (RR) alongside their 95% confidence intervals. The heterogeneity among the included studies was assessed using the chi-square test and quantitatively assessed using the I2 statistic. A value of I2 < 50.0% or P > .1 was deemed indicative of nonsignificant heterogeneity. In the cases where the heterogeneity between studies was nonsignificant (P ≥ .1, I2 ≤ 50%), the fixed-effects model was utilized for analysis. On the contrary, if there was notable heterogeneity among the included studies (P < .1, I2 > 50%), the analysis was conducted using the random-effects model. These data underwent analysis using RevMan 5.4 software. Statistical significance was defined as a 2-sided P < .05.
Results
Characteristics of the Included Studies
A cumulative count of 442 articles was obtained. After initial screening of titles and abstracts, a comprehensive review of complete texts was conducted to ascertain final inclusion status; 9 articles meeting the inclusion criteria were selected, including 8 Chinese articles and 1 English article. The literature explicitly stated that the research protocol had received approval from the pertinent ethics committee and that patients or their families provided informed consent prior to surgery. The flowchart depicting the literature screening procedure is presented in Figure 1.
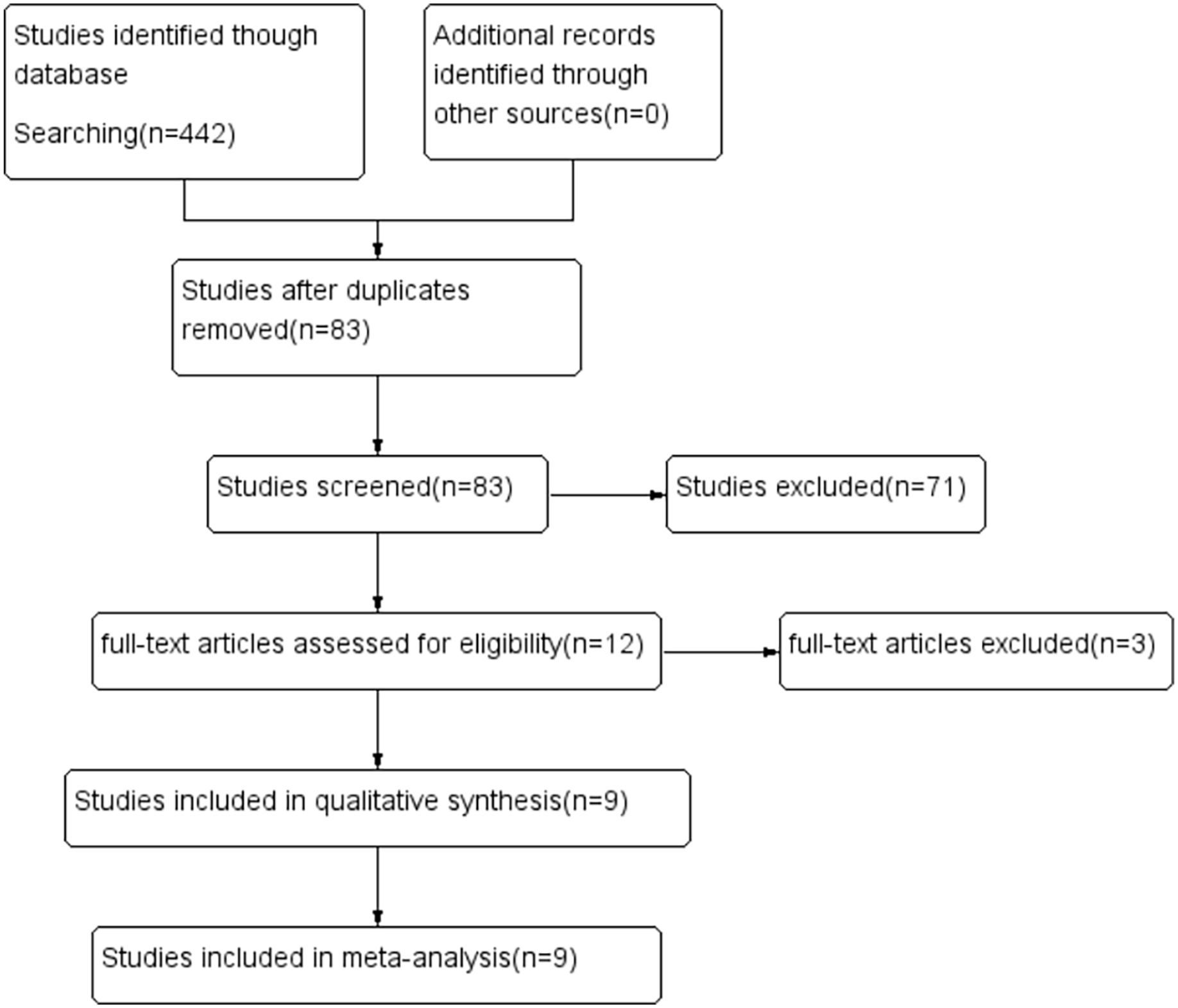
Flowchart illustrating the study selection process for the present meta-analysis.
Study Characteristics and Quality Assessment
This meta-analysis comprised a total of 9 clinical trials, and their basic characteristics are summarized in Table 1. The results of the bias risk assessment are presented in Figure 2.
Characteristics of Included Studies.
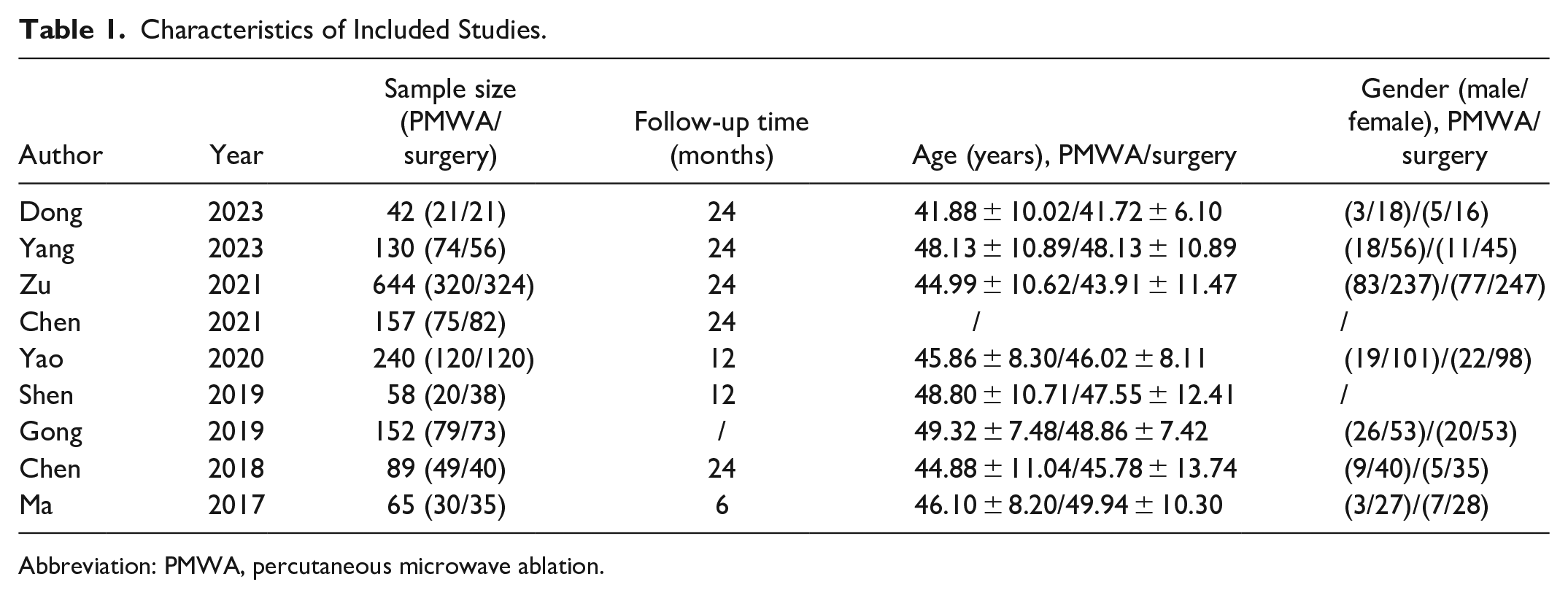
Abbreviation: PMWA, percutaneous microwave ablation.
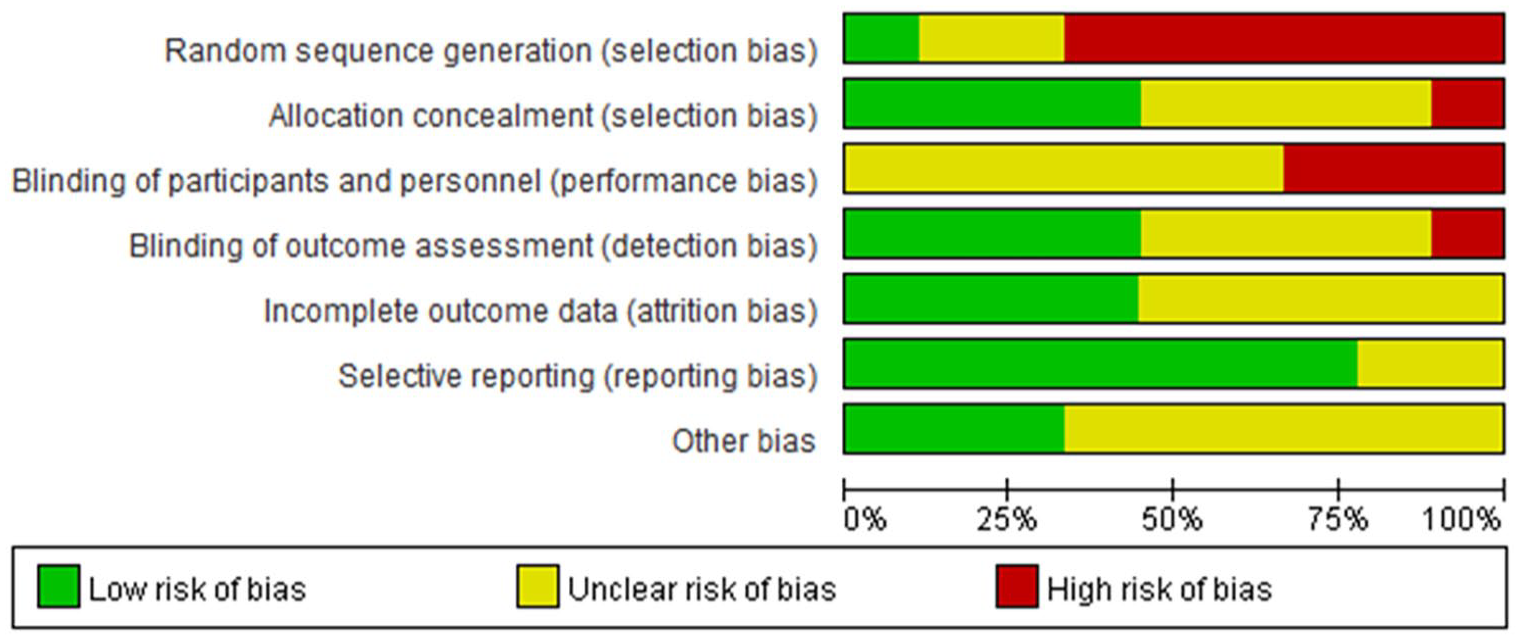
Assessment of risk of bias.
Surgical Status
Operation time
Five studies4-8 reported the operation time. Significant variability was noted between the PMWA group and the conventional surgery group (I2 = 100%, P < .00001).
Employing a random-effects model, the combined analysis showed that the operative duration in the PMWA group was significantly shorter compared to the conventional surgery group (MD = −36.36; 95% CI −55.66 to −17.06; P = .0002), with statistically notable disparities noted between the 2 cohorts (Figure 3A).
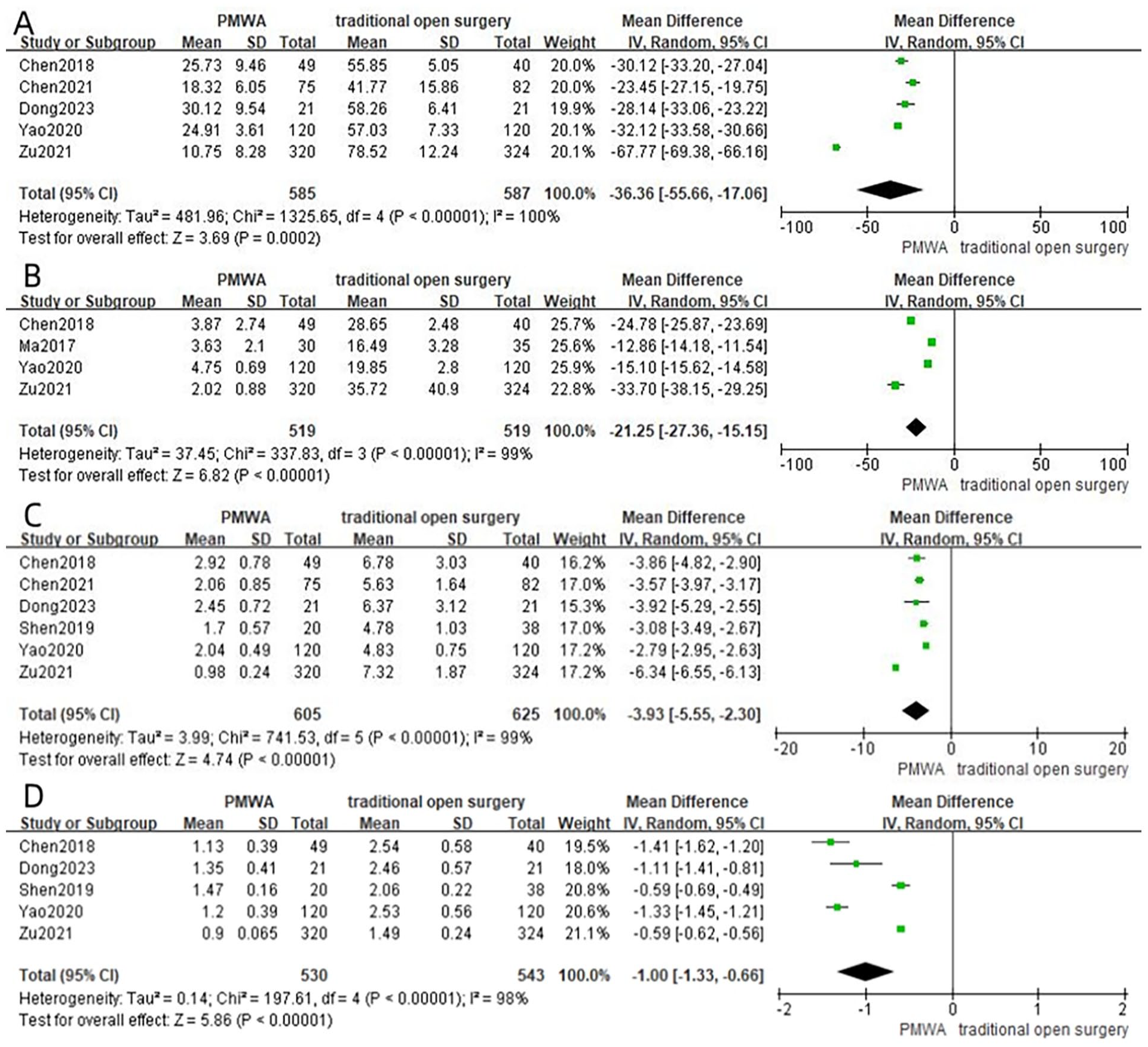
Forest plot of surgical time (A), intraoperative blood loss (B), length of hospital stay (C), and hospitalization cost (D) between the PMWA group and conventional surgery group.
Intraoperative blood loss
Four studies4,7-9 reported intraoperative blood loss. Significant heterogeneity was noted between the PMWA and conventional surgery groups (I2 = 99%, P < .00001). Employing a random-effects model, the pooled analysis showed that intraoperative blood loss in the PMWA group was significantly less than that in the conventional surgery group (MD = −21.25; 95% CI −27.36 to −15.15; P < .00001), with statistically notable distinctions between the 2 groups (Figure 3B).
Hospital stay
Six studies4-8,10 reported postoperative hospital stay. Substantial heterogeneity was observed between the 2 cohorts (I2 = 99%, P < .00001). Employing a random-effects model, the aggregated analysis revealed that the duration of postoperative hospitalization in the PMWA group was significantly shorter than that in the conventional surgery group (MD = −3.93; 95% CI −5.55 to −2.30; P < .00001), with statistically notable distinctions between the 2 groups (Figure 3C).
Hospitalization cost
Five studies4,6-8,10 reported postoperative hospitalization costs. Significant heterogeneity was observed between the 2 cohorts(I2 = 98%, P < .00001). Employing a random-effects model, the pooled analysis showed that the hospitalization costs in the PMWA group were lower than those in the conventional surgery group (MD = −1.00; 95% CI −1.33 to −0.66; P < .00001), with statistically significant differences between the 2 groups (Figure 3D).
Clinical Efficacy
Postoperative complications
Eight studies4,6-12 reported the incidence of postoperative complications. No substantial variations in heterogeneity were observed between the PMWA group and the conventional surgery group (I2 = 0%, P = .65). Employing a fixed-effects model, the comprehensive analysis suggested that the PMWA group had a reduced occurrence of postoperative complications in comparison to the conventional surgery group (RR = 0.29; 95% CI 0.21 to 0.40; P < .00001), with statistically significant differences (Figure 4A).
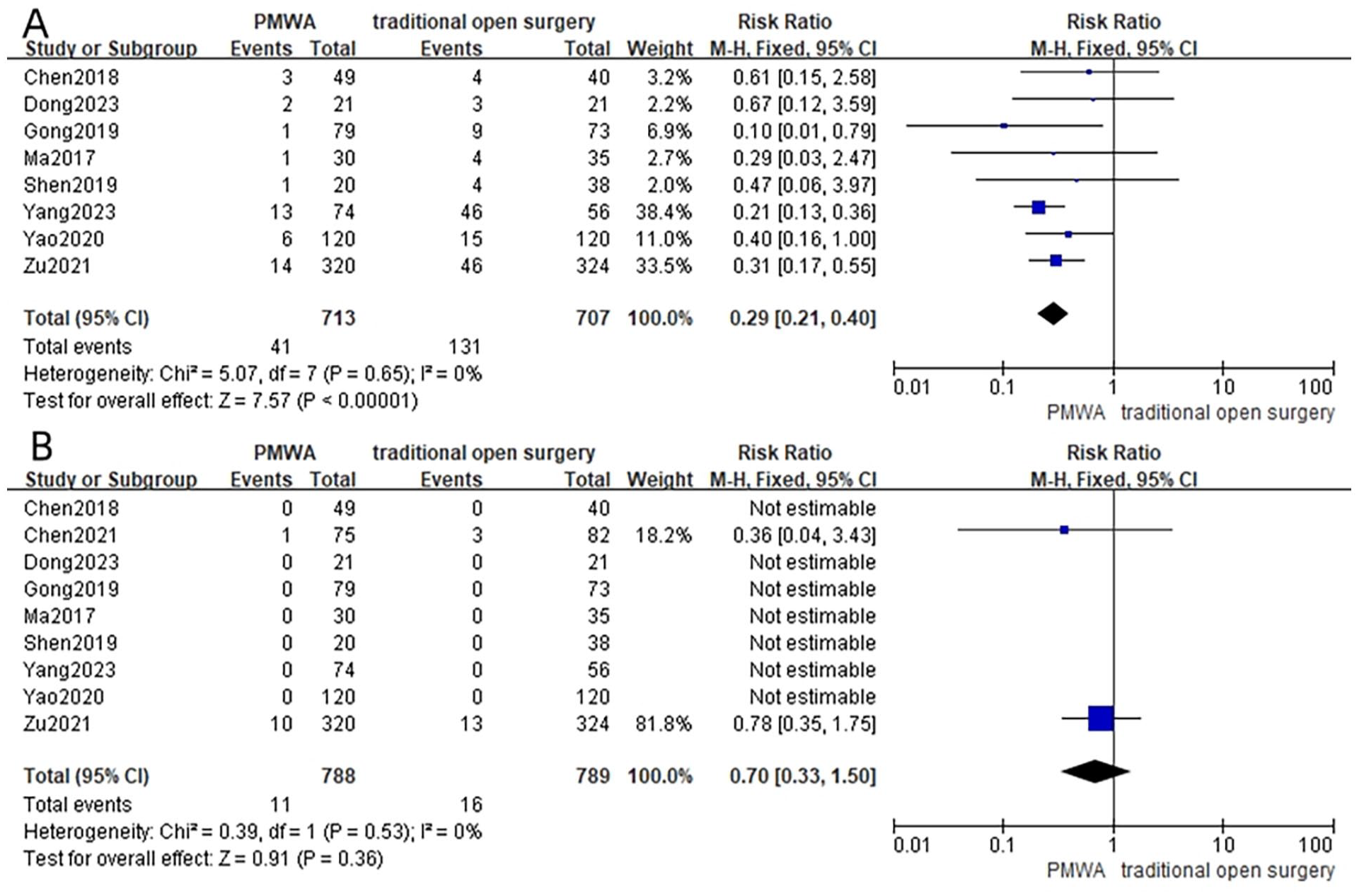
Forest plot of postoperative complications (A) and postoperative recurrence or lymph node metastasis rate (B) between the PMWA group and conventional surgery group.
Incidence of postoperative recurrence or LNM
Nine studies4-12 documented the occurrence of postoperative recurrence or LNM. There were no notable variations in heterogeneity between the PMWA group and the conventional surgery group (I2 = 0%, P = .53). Employing a fixed-effects model, the comprehensive analysis indicated that there was no statistically significant disparity in the frequency of postoperative recurrence or LNM between the PMWA group and the conventional surgery group (RR = 0.70; 95% CI 0.33 to 1.50; P = .36, Figure 4B).
Status of Postoperative Thyroid Function
Comparison of postoperative FT3 levels
Six studies4,6,7,9-11 reported the postoperative FT3 levels of patients at 30 days. Significant heterogeneity was evident between the PMWA group and the conventional surgery group (I2 = 89%, P < .00001). Utilizing a random-effects model, the comprehensive analysis revealed that postoperative FT3 levels were elevated in the PMWA group compared to the conventional surgery group (MD = 0.61; 95% CI 0.33 to 0.90; P < .00001), demonstrating statistically significant distinctions (Figure 5A).
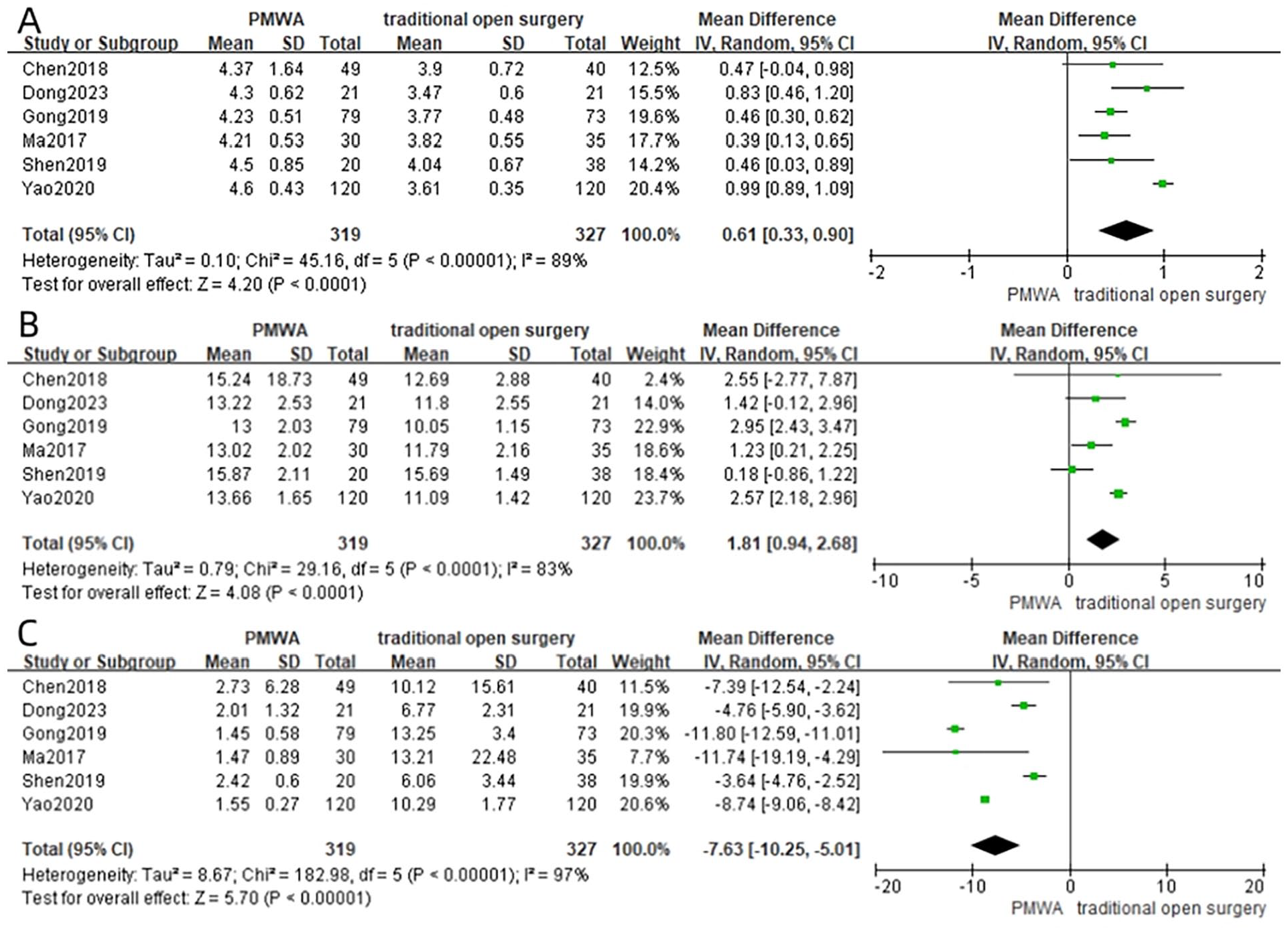
Forest plot of postoperative 30 day FT3 (A), FT4 (B), and TSH (C) between the PMWA group and the conventional surgery group.
Comparison of postoperative FT4 levels
Six studies4,6,7,9-11 reported the postoperative FT4 levels of patients at 30 days. Substantial heterogeneity was observed between the PMWA group and the conventional surgery group (I2 = 83%, P < .0001). Utilizing a random-effects model, the comprehensive analysis indicated that postoperative FT4 levels were elevated in the PMWA group compared to the conventional surgery group (MD = 1.81; 95% CI 0.94 to 2.68; P < .0001), with statistically significant differences (Figure 5B).
Comparison of postoperative TSH levels
Six studies4,6,7,9-11 reported the postoperative TSH levels of patients at 30 days. Significant heterogeneity was observed between the PMWA group and the conventional surgery group (I2 = 97%, P < .00001). Utilizing a random-effects model, the comprehensive analysis revealed that postoperative TSH levels in the PMWA group were markedly reduced compared to the conventional surgery group (MD = −7.63; 95% CI −10.25 to −5.01; P < .00001), with statistically significant differences (Figure 5C).
Postoperative Tumor Changes in the PMWA Group
Eight studies4-10,12 reported postoperative changes in tumor volume (Figure 6A) and the rate of tumor volume reduction (Figure 6B) in the PMWA group. It was observed that the pattern of tumor volume changes was consistent across the 8 studies: the tumor volume increased significantly 1 month postoperatively, followed by a gradual decrease, and by 24 months postoperatively, it largely returned to normal (Figure 6).
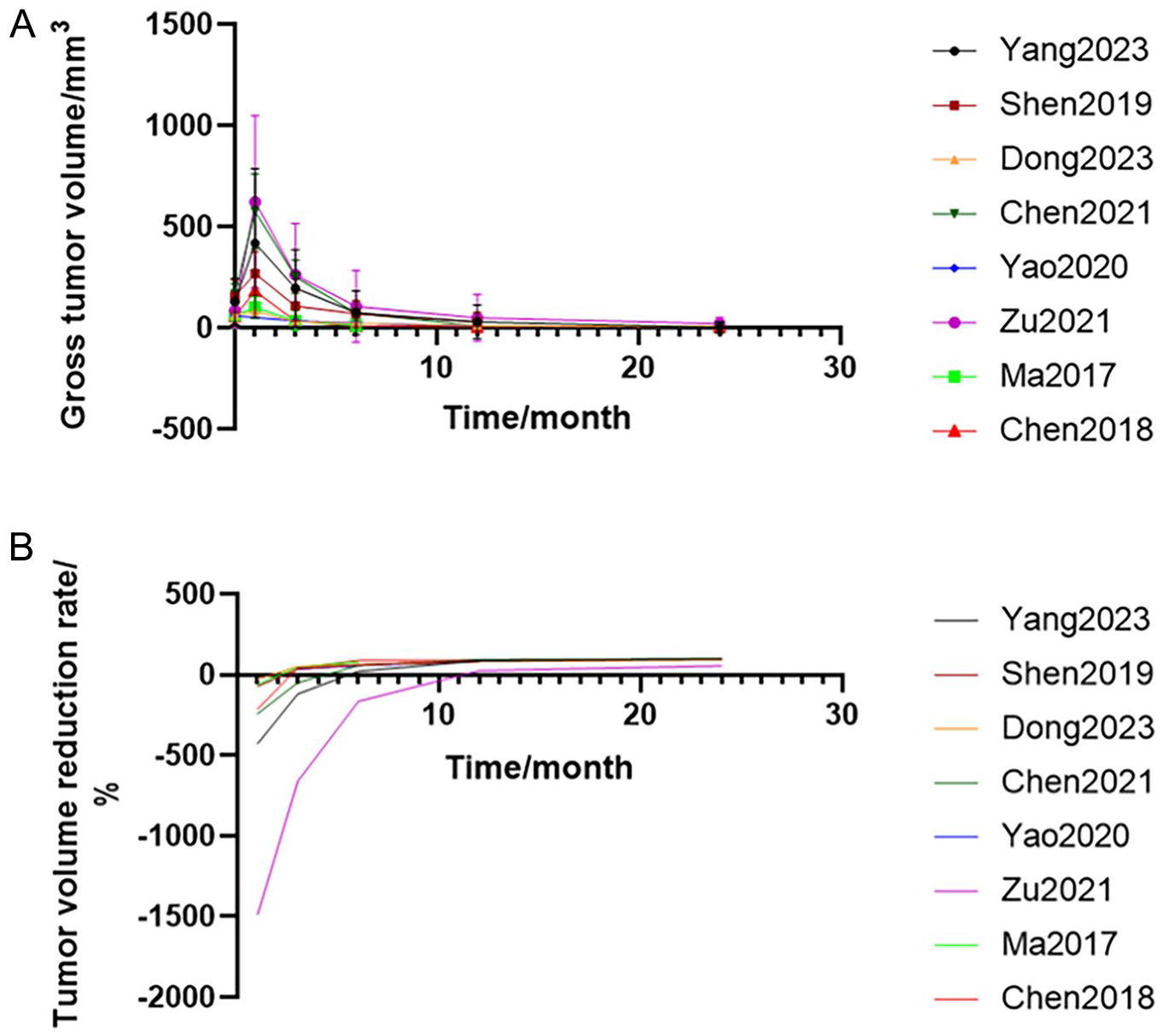
Changes in tumor volume (A) and tumor volume reduction rate (B) after surgery in the PMWA group.
PCS/MCS/SF-36 Scores at Different Time Points for Both Groups of Patients
Two studies5,12 reported the scores at different time points. There was no statistically significant divergence in PCS scores between the 2 groups before and after treatment. (P > .05). However, significant differences were observed in MCS scores at the 3, 12, and 24 month postoperative intervals (P < .05), Likewise, statistically significant disparities were noted in SF-36 scores at the 3, 6, 12, and 24 month postoperative time points (P < .05). The PMWA group demonstrated notable advantages compared to the conventional surgery group (Table 2).
Changes in PCS, MCS, and SF-36 Scores Between the 2 Groups of Patients.
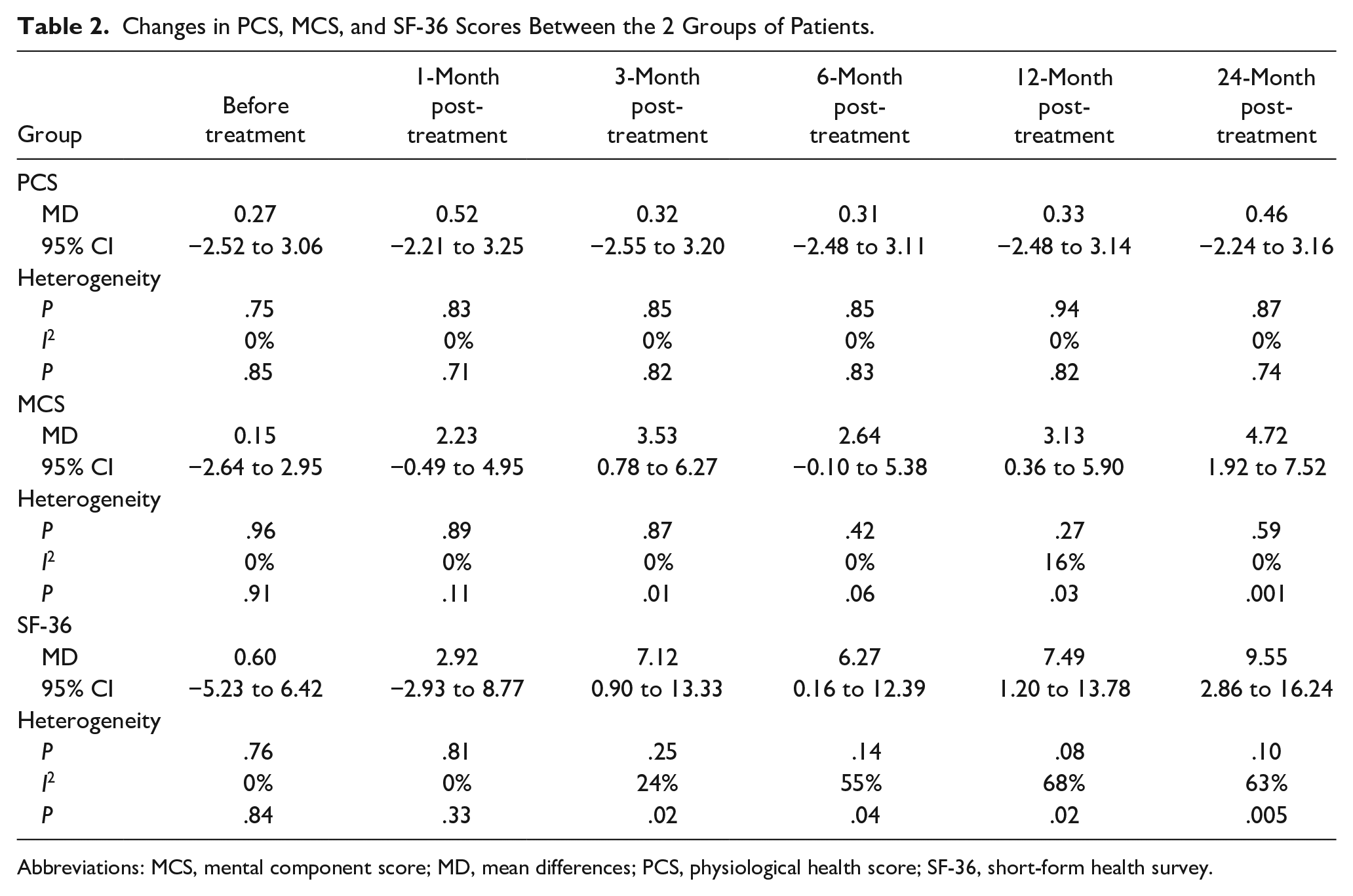
Abbreviations: MCS, mental component score; MD, mean differences; PCS, physiological health score; SF-36, short-form health survey.
Discussion
PTMC, which refers to the predominant malignant neoplasm in the head and neck region, has seen a significant increase in detection rates due to advances in ultrasound examination and FNAB techniques. In China, papillary thyroid carcinoma (PTC) ranks first in the incidence of malignant tumors in the endocrine system. 13 Over the past 30 years, the prevalence of thyroid carcinoma in the United States has increased twice, with the majority of cases being PTC, predominantly PTMC. 14 PTMC progresses slowly with a low mortality rate. The 2015 edition of the American Thyroid Association suggests close observation with thorough communication and explanation for patients with low-risk PTMC and their families. 15 However, data indicate that over a 5 year follow-up period, PTMC exhibited a 5.3% increase in volume and a LNM rate of 1.6%. 16 Therefore, proactive monitoring alone may not effectively prevent and treat PTMC. Surgical resection remains the primary treatment for PTMC. However, surgical treatment poses challenges, such as significant trauma and financial burden. Studies indicate that surgery-related complications, including recurrent laryngeal nerve injury, postoperative hypothyroidism, and permanent hypocalcemia, occur at rates of 0.2% to 1.1%, 5% to 49%, and 1%. 17 Hence, the selection of a minimally invasive, effective, and safe treatment modality has become an increasingly important clinical concern. MWA has been recognized for its value in treating benign thyroid diseases, 18 offering advantages such as precise localization, short treatment duration, and minimal complications. 19 It provides a new option for patients with PTMC. However, the comparative efficacy of PMWA and surgical treatment for PTMC lacks objective data, with limited case numbers and numerous limitations. Therefore, this study undertook meta-analysis to evaluate the efficacy of PMWA versus surgical intervention for PTMC.
The findings of this study suggest that, regarding clinical efficacy, within the selected literature, Zu reported 4 cases (4/320) of local cancer recurrence and 6 cases (6/320) of cervical LNM without distant spread in the PMWA group, whereas the surgical resection group reported 5 cases (5/320) of local cancer recurrence and 8 cases (8/320) of cervical LNM without distant spread. Chen reported 1 case (1/75) of cervical LNM without distant spread in the PMWA group, whereas the surgical resection group reported 3 cases (6/82) of cervical LNM without distant metastasis. There was no statistically significant disparity noted in postoperative recurrence or LNM between the 2 surgical approaches, suggesting that PMWA demonstrates similar therapeutic efficacy to traditional surgical resection. Miyauchi et al. 20 compared 2 groups of PTMC patients undergoing close follow-up and surgical treatment and found no statistically significant disparity in recurrence and cervical lymph node spread between the 2 cohorts. A follow-up report over a period of 5 years indicated the complete disappearance of all tumors after PMWA treatment, with a volume reduction rate of (99.37% ± 4.02%), and no occurrences of recurrence, LNM, or distant metastasis were observed postoperatively. 21 These research findings suggest that the occurrence of postoperative recurrence and LNM is low in PTMC patients undergoing MWA treatment. On the one hand, this could be attributed to the small diameter of tumor nodules, as MWA typically directly deactivates them. On the other hand, it is speculated that an anti-tumor immune response activated by thermal ablation (TA) may contribute to this effect. 22 Additionally, we ensure that the trajectory of the ablation needle aligns consistently with the trajectory of the previous fine needle aspiration procedure during entry and exit and heat coagulation of the needle tract is employed upon withdrawal, minimizing the potential for disseminated implantation caused by the ablation needle. Nevertheless, it is irrefutable that recurrence and LNM may still manifest in a minority of tumors post MWA, primarily attributed to the following factors: (1) the multicentric nature of tumor development; (2) potential for occult lymph node involvement by tumors; (3) adjustments made by operators to minimize the risk of organ injury near critical structures, which may result in incomplete ablation and residual primary tumor foci; (4) inadequate coverage of the central lymph node region during ablation, leading to suboptimal tumor eradication.
In this study, we compared the safety of PMWA and conventional thyroidectomy in terms of hoarseness, swallowing cough, hematoma, hypoparathyroidism, and postoperative pain. In the PMWA group, only 5.7% of patients (41/713) experienced mild complications, with only 1 case of permanent hoarseness, showing mild hoarseness without dysphagia and coughing after drinking water, while the rest were transient complications that resolved during the follow-up period. The frequency of complications in the PMWA group was lower compared to the excision surgery group. exhibiting a statistically significant disparity. Therefore, PMWA is safe and well-tolerated. The reasons for the low incidence of complications in the PMWA group include precise positioning using a linear array probe and real-time ablation under ultrasound guidance to ensure the complete coverage of the ablation zone and minimize the impact on normal thyroid tissue. 23 Additionally, the use of hydrodissection technology, slow and continuous injection of appropriate physiological saline around the thyroid prevents injury to the trachea, major blood vessels, and recurrent laryngeal nerve, protecting surrounding vital structures. 24 None of the patients in either group suffered from life-threatening complications, such as postoperative hemorrhage, laryngeal edema, or respiratory distress. The low incidence of complications in the PMWA group, along with fast postoperative recovery, short hospital stays, and low hospital costs, fully demonstrate the minimally invasive, efficient, and rapid recovery advantages of MWA, making it conducive for patient acceptance and cost-saving for patients and the healthcare system.
The impact on thyroid function is an important consideration in the treatment of PTMC. This study shows that, compared to traditional surgery, 30 days after surgery, the levels of FT3 and FT4 in the PMWA group are elevated. Studies have indicated that PMWA has minimal impact on thyroid function. 25 Relative to conventional surgery, PMWA is a precise treatment conducted under ultrasound guidance with minimal damage to surrounding tissues, thus maximizing the protection of normal thyroid tissue and function in patients. Therefore, thyroxine replacement therapy is not required after PMWA treatment. 26 None of the patients in either group suffered from severe complications, such as postoperative hemorrhage, laryngeal edema, or respiratory distress. This is because conventional surgery requires the removal of most or all of the thyroid tissue, leading to postoperative thyroid hormone disruption and a subsequent decline in thyroid function, necessitating lifelong thyroxine replacement therapy.
Due to the predominance of female patients with PTMC, there is often significant psychological anxiety and concerns about aesthetics, which greatly impact their quality of life. As a minimally invasive treatment, PMWA only involves 2 aspects of trauma: the puncture wound and the thermal energy from microwaves, resulting in no scarring postoperatively and a significant improvement in appearance compared to the surgical group. Studies 27 indicate that for PTMC cases with a treatment diameter of ≤1 cm and the absence of extrathyroidal extension or metastatic disease, PMWA has demonstrated a complete remission rate of 93.9%, which can greatly alleviate anxiety in the PMWA group postoperatively. Postoperatively, both groups of patients showed increases in MCS and SF-36 scores, indicating a decrease in anxiety levels and an enhancement in quality of life after treatment with both modalities. However, the discrepancies noted at different time intervals attained statistical significance (P < .05), with the PMWA group significantly outperforming the surgical excision group. Research data demonstrate that patients in the PMWA group have higher life satisfaction. Owing to the benefits of diminished pain and decreased complication rates linked with PMWA intervention, which can stimulate immune cells, enhance immune function, promote rapid recovery, and consequently accelerate disease recovery and improve the overall quality of life. For some patients in the surgical excision group, anxiety may increase due to potential surgical complications and long-term supplementation with exogenous thyroid hormones. Compared to surgical excision, PMWA is more favorable for patient acceptance and results in a higher postoperative quality of life. In a small retrospective cohort analysis 28 involving 92 PTMC patients, individuals who underwent PMWA exhibited superior quality of life throughout the 42-month follow-up duration compared to those who underwent surgical intervention.
The principle of TA is to use thermal energy to cause coagulative necrosis of lesion tissues or cells at high temperatures. Based on the ablation principle and equipment used, TA techniques can be categorized into MWA, radiofrequency ablation (RFA), and laser ablation (LA). Studies 29 have shown that TA is effective and safe for the treatment of PTMC; however, there is a variability in the rate of volume reduction of PTMC. The volume reduction rate after RFA was the highest, followed by MWA and LA, and the improvement in patient quality of life after TA was considerably better than that after thyroidectomy. The differences among the 3 techniques include the following points: (1) The ablation range and ablation energy vary, both MWA and LA have excellent performance on the ablation longitudinal axis (easily exceeding 10 mm) for PTMC. MWA performed much better than LA on the ablation orthogonal axis. MWA and LA are expected to achieve complete ablation of ≤6.70 and ≤4.69 mm PTMC separately by single-applicator fixed ablation considering a unilateral 2-mm safe margin. (2) RFA showed relatively less complications, LNM, operation time, and intra-operative blood loss, compared with other TA treatments. MWA indicated the lowest probability of recurrence; LA showed the longest hospital stays. 30 Studies 31 have shown that results are comparable at 4 years between RFA and thyroid lobectomy for low-risk PTMC.
There are still many details to consider in the treatment of low-risk PTMC with TA. The goal of TA is to reduce the volume of thyroid nodules through irreversible coagulative necrosis, ideally achieving complete ablation. A complete ablation is defined as no contrast perfusion into the ablation zone, with a minimum safety margin of 3 mm. 32 Tuttle et al. have proposed a safe margin of at least 2 mm outside the tumor lesion. 33 For PTMC located near the posterior capsule, special perioperative procedures for TA are required to prevent potential thermal damage to the surrounding normal tissues. Zheng et al. have revealed that the efficacy of TA on PTMC in the isthmus reaches 100%, and cases of recurrence, LNM, and severe complications are not reported. 34 Patients with multifocal PTMC have a higher risk of cervical LNM, making multifocality a predictor of recurrence. Studies 35 have shown that the prognostic value of multifocality is particularly significant in non-PTMC patients.
PTMC requires a multidisciplinary management strategy. Usually, low-risk PTMC has an acceptable prognosis and requires no surgical procedures. Active Surveillance (AS) is an effective method recommended to patients with very low-risk PTMCs in guidelines. 36 TA can serve as an alternative to AS and surgery for low-risk PTMC; if tumor progression occurs, surgical treatment can be performed. High-risk PTMC may be directly treated with surgery. Additionally, patients with a positive family history had more aggressive clinicopathological behaviors, suggesting that more vigilant screening and management for familial PTC may be helpful. 37 In conclusion, the procedures during the entire perioperative period should be standardized to improve the outcomes of TA in treating patients with PTMC. 38
PMWA treatment has certain indications and limitations. PMWA is appropriate for patients with low-risk PTMC (T1aM0N0). However, for individuals with a predisposition to LNM or requiring lymph node dissection, PMWA may not be the optimal choice because it cannot clear lymph nodes like traditional surgery.
This study has several limitations: (1) Non-inclusion of relevant studies published in languages other than English and Chinese may introduce publication bias. (2) The study’s sample size is limited, potentially affecting the accuracy of the analysis results. (3) The majority of studies are retrospective in nature, due to the absence of sufficient randomized, double-blind, large-scale trial data, reliance on non-randomized controlled trial data may compromise the integrity of the research. (4) The included studies were conducted in China and involved adult participants. Further research is needed to address populations of different age groups or from other regions of the world. (5) The longest follow-up period among the 9 included studies was 24 months, and further investigation is required to evaluate the long-term efficacy of the treatment.
Conclusion
Based on the research results, PMWA treatment for patients with PTMC is comparable to conventional surgical treatment in terms of efficacy. It offers advantages such as minimal trauma, quick recovery, no scarring, and fewer complications compared to open surgery. However, given the constrained sample size and abbreviated follow-up duration in existing studies, uncertainties persist regarding PMWA technology, including tumor recurrence and metastasis. These uncertainties necessitate further validation through extensive long-term follow-up studies with larger sample sizes.
Footnotes
Acknowledgements
None.
Author Contributions
Rongrong Han was involved in screening studies, data extraction, risk of bias assessment, data entry, statistical analysis, and manuscript preparation. Xiang Gao was involved in the formulation of the study, risk of bias assessment, statistical analysis, and manuscript preparation. Zhixin Ji was involved in data entry, statistical analysis, and manuscript preparation. Yao Chen was involved in study formulation, data analysis, statistical evaluation, and manuscript preparation.
Consent for Publication
The authors hereby transfer, assign, or otherwise convey all copyright ownership, including any and all rights incidental thereto, exclusively to the journal, in the event that such work is published by the journal.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethics Approval and Consent to Participate
The study was approved by the hospital ethical committee.